Article Text

Abstract
Background Changes over the last 5 years (2013–18) in the serotypes implicated in adult pneumococcal pneumonia and the patient groups associated with vaccine-type disease are largely unknown.
Methods We conducted a population-based prospective cohort study of adults admitted to two large university hospitals with community-acquired pneumonia (CAP) between September 2013 and August 2018. Pneumococcal serotypes were identified using a novel 24-valent urinary monoclonal antibody assay and from blood cultures. Trends in incidence rates were compared against national invasive pneumococcal disease (IPD) data. Persons at risk of vaccine-type pneumonia (pneumococcal conjugate vaccine (PCV)13 and pneumococcal polysaccharide vaccine (PPV)23) were determined from multivariate analyses.
Findings Of 2934 adults hospitalised with CAP, 1075 (36.6%) had pneumococcal pneumonia. The annual incidence of pneumococcal pneumonia increased from 32.2 to 48.2 per 100 000 population (2013–18), predominantly due to increases in PCV13non7-serotype and non-vaccine type (NVT)-serotype pneumonia (annual incidence rate ratio 1.12, 95% CI 1.04 to 1.21 and 1.19, 95% CI 1.10 to 1.28, respectively). Incidence trends were broadly similar to IPD data. PCV13non7 (56.9% serotype 3) and PPV23non13 (44.1% serotype 8) serotypes were identified in 349 (32.5%) and 431 (40.1%) patients with pneumococcal pneumonia, respectively. PCV13-serotype pneumonia (dominated by serotype 3) was more likely in patients in the UK pneumococcal vaccination clinical risk group (adjusted OR (aOR) 1.73, 95% CI 1.31 to 2.28) while PPV23-serotype pneumonia was more likely in patients outside the clinical risk group (aOR 1.54, 95% CI 1.13 to 2.10).
Interpretation The incidence of pneumococcal CAP is increasing, predominantly due to NVT serotypes and serotype 3. PPV23-serotype pneumonia is more likely in adults outside currently identified clinical risk groups.
- community acquired pneumonia
- Streptococcus pneumoniae
- pneumococcal conjugate vaccine
- pneumococcal polysaccharide vaccine
- replacement serotypes
- risk groups
- pneumococcal pneumonia
- non-invasive pneumococcal disease
Statistics from Altmetric.com
- community acquired pneumonia
- Streptococcus pneumoniae
- pneumococcal conjugate vaccine
- pneumococcal polysaccharide vaccine
- replacement serotypes
- risk groups
- pneumococcal pneumonia
- non-invasive pneumococcal disease
Key messages
What is the key question?
Which pneumococcal serotypes are implicated in adult pneumococcal pneumonia and which patient groups are associated with vaccine-serotype disease?
What is the bottom line?
The incidence of pneumococcal community-acquired pneumonia is increasing, predominantly due to non-vaccine serotypes and serotype 3.
Novel pneumococcal vaccines targeting emerging serotypes are needed.
Pneumococcal conjugate vaccine 13-serotype pneumonia (dominated by serotype 3) is more likely in patients in the UK pneumococcal vaccination clinical risk group while 23-valent pneumococcal polysaccharide vaccine-serotype pneumonia is more likely in patients outside the clinical risk group.
Why read on?
This large prospective cohort study is the first to describe pneumococcal serotype trends and clinical risk groups in adult patients with community-acquired pneumonia in the UK using a novel and validated multiplex immunoassay.
Introduction
Pneumococcal conjugate vaccines (PCVs) have demonstrated substantial effectiveness in reducing pneumococcal disease due to vaccine serotypes.1 2 In England and Wales, immunisation of children with a 7-valent pneumococcal conjugate vaccine (PCV7) commenced in 2006 and was replaced in April 2010 with a 13-valent pneumococcal conjugate vaccine (PCV13).3 Over the same period, individuals aged >2 years with a clinical risk factor for pneumococcal disease and all adults aged ≥65 years have been offered vaccination with the 23-valent pneumococcal polysaccharide vaccine (PPV23).3
Both PCVs have been associated with rapid and sustained reductions in overall and vaccine-serotype invasive pneumococcal disease (IPD) in young children.4 PCVs also reduce carriage in vaccinated individuals and hence prevent onward transmission to unvaccinated older children and adults. Thus, reductions in IPD and pneumococcal pneumonia have been observed across all age groups.4–7
Since 2013/14, however, overall IPD incidence due to PCV13 serotypes has plateaued in the UK, while IPD due to non-PCV serotypes has increased rapidly, especially in adults and the elderly.2 4 The USA by contrast, where PCV13 has been recommended as part of the childhood immunisation programme since 2010, has not observed such an increase in non-PCV13-serotype IPD despite large declines in PCV13-serotype disease.8
In adults, IPD accounts for <10% of pneumococcal pneumonia cases. There are therefore limited contemporary data on the range of serotypes causing pneumococcal pneumonia in adults in the UK.7 In particular, the contribution of PCV13 and PPV23 serotypes to pneumococcal pneumonia is important to inform national pneumococcal vaccine policy, especially in adults and the elderly.9 10
Since 2008, we have conducted a prospective population-based adult pneumococcal pneumonia study to determine changes in clinical disease and the responsible pneumococcal serotypes.7 11 Recently, a novel, validated 24-valent multiplex urinary immunoassay was developed to detect PCV and PPV serotypes in patients with non-invasive disease.12 We report the use of this assay in a previously unreported cohort of patients to describe a) serotype trends in adult pneumococcal pneumonia since PCV13 replaced PCV7 and b) the clinical risk groups associated with vaccine-type disease.
Methods
Study design
We conducted a prospective observational cohort study of consecutive adult patients admitted to two large university hospitals with community-acquired pneumonia (CAP) between September 2013 and August 2018. Together, these two hospitals cover the catchment for emergency admissions in the Greater Nottingham area. All patients admitted to acute admission areas were screened for study eligibility every weekday. Patients aged ≥16 years presenting with one or more symptom suggestive of lower respiratory tract infection (defined as cough, increasing dyspnoea, sputum production and fever), with evidence of acute infiltrates consistent with respiratory infection on admission radiography, and treated for a diagnosis of CAP were eligible. Exclusion criteria included hospitalisation within 10 days of index admission, a diagnosis of tuberculosis or postobstructive pneumonia. Informed consent was obtained from all study participants; if patients lacked capacity, proxy consent was sought from patient personal consultees. Demographic and clinical characteristic data were collected using a standardised proforma.
Microbiology
Baseline microbiological investigations were performed at the discretion of the clinical team. In addition, urine samples for pneumococcal-specific microbiological analyses were obtained within 72 hours of admission; Binax-NOW (Alere, Stockport, UK) assay for pneumococcal C-polysaccharide urinary antigen detection (UAD) was performed in the local microbiological laboratory,13 with the remaining volume of urine frozen at −80°C and batch transported to Public Health England (PHE)’s Respiratory and Vaccine Preventable Bacteria Reference Unit in Colindale, London for pneumococcal serotyping using a validated multiplex immunoassay (Bio-plex24.) The Bio-plex24 assay targets the detection of pneumococcal serotypes 1, 2, 3, 4, 5, 6A, 6B, 7F, 8, 9N, 9V, 10A, 11A, 12F, 14, 15B, 17F, 18C, 19A, 19F, 20, 22F, 23F, 33F and the pneumococcal cell-wall polysaccharide.12 Samples from September 2014 to August 2015 were tested using the original protocol as published by Eletu et al, with a clinical sensitivity of 96.2% and specificity 89.9%.12 The assay was then updated to include minor protocol modifications and alternative monoclonal clones for serotypes 7F, 18C, 19F, 20 and 22F; this updated assay (validated using 2037 urine samples from patients with CAP or suspected pneumococcal disease, with a calculated clinical sensitivity of 94.3% and specificity of 93.6%—manuscript in preparation) was used for the remainder of the study period. Sixteen of the human monoclonal antibodies within the Bio-plex24 assay exhibited some cross-reactivity with specific non-targeted pneumococcal serotypes. A ‘checkerboard’ system for interpretation of results allowed serotype identification for five of these serotypes. In the remaining 11, based on probabilistic grounds, the designated serotype for analysis was determined according to the predominant serotype observed in national IPD data for the corresponding time period (online supplementary appendix 2).4
Supplemental material
During sample testing between September 2014 and August 2015 (first batch tested), the monoclonal antibodies targeting serotypes 7F, 20 and 22F were found to cross-react with an unknown substance in some urine samples. Therefore, in reporting results for samples from that study year, we excluded all results for serotype 7F and applied a higher diagnostic threshold for serotypes 20 and 22F, with results excluded if these criteria were not satisfied.12 Samples from the four other study years were tested with an improved Bio-plex24 assay, outlined above, eliminating the non-specific cross-reactivity.
Up to September 2017, bacteraemic isolates of Streptococcus pneumoniae were identified by standard phenotypic methods and serotyped by slide agglutination tests with latex antisera (ImmuLex Pneumotest Kit) or standard factor sera (SSI Diagnostica, Denmark). From October 2017, confirmation of pneumococcal isolate identification and serotype prediction was performed by bio-informatical methods following DNA extraction and whole genome sequencing,14 with the exception of serotypes within serogroup 24 which were identified by conventional methods using antisera.15
Patients were considered to have pneumococcal CAP if any of the following criteria were met: a) positive pneumococcal UAD or b) a positive blood culture for S. pneumoniae or c) pneumococcal serotype or cell wall polysaccharide detection by the Bio-plex24 assay.
Statistical analysis
Serotypes were classified according to the serotype content of vaccines: PCV7 serotypes (serotypes 4, 6B, 9V, 14, 18C, 19F and 23F), PCV13non7 serotypes (serotypes 1, 3, 5, 6A/C, 7F/A and 19A), PPV23non13 serotypes (serotypes 2, 8, 9N, 10A, 11A, 12F, 15B, 17F, 20, 22F and 33F) and non-vaccine-type (NVT) serotypes (comprising a) any non-PCV13, non-PPV23 serotype and b) ‘untyped’ pneumococcal disease; Binax UAD positive without subsequent serotype identification, or Bio-plex24 positive for cell wall polysaccharide only). Definations of variables used in the analyses are available in (online supplementary appendix 1).
Annual incidence rates were derived from mid-year estimates from the Office for National Statistics for the Greater Nottingham area, including local population data stratified by age group (16–49, 50–64, 65–74, 75–84, ≥85 years). Trends between 2013 and 2018 comparing overall incidence of CAP, pneumococcal CAP and CAP according to serotype categories were examined. Additionally, serotype trends were compared with corresponding national IPD surveillance data.4 Poisson regression models together with 95% CIs were used to assess year-to-year variation and linear trends in serotype distribution.
Clinical risk factors for pneumococcal disease were defined in accordance with PHE’s ‘Immunisation against Infectious Diseases’ (The Green Book).3 For analyses of groups at risk of pneumococcal disease, patients with multiple serotypes that crossed vaccine groups were excluded (eg, one or more positive serotype in both PCV13-serotype and PPV23-serotype disease groups). Baseline characteristics and comorbid risk factors for PCV13-serotype and PPV23-serotype disease were compared using Pearson’s χ2 or Fisher’s exact tests for categorical variables, and the Mann-Whitney U test for non-parametric continuous variables. Likelihood ratio tests were used to determine the best model fit for continuous variables. Multivariate logistical regression was used to compare the independent association between comorbid disease and a) PCV13-serotype and b) PPV23-serotype disease. Purposeful selection of variables for inclusion in the multivariate analysis was conducted based on clinical risk factors outlined in PHE’s ‘Immunisation against Infectious Diseases’ (The Green Book),3 in conjunction with evidence from previous studies of risk factors for pneumococcal and/or vaccine serotype disease, and considering biological plausibility, and were specified a priori.16 Secondary analyses were conducted examining the risk of PCV13-serotype and PPV23-serotype disease in:
the pneumococcal clinical risk group (defined as adults 16–64 years with ≥1 clinical risk factor for pneumococcal disease or age ≥65 years),
specific clinical risk groups: (1) aged 16–64 years without clinical risk factors, (2) aged 16–64 years with ≥1 clinical risk factor, (3) aged ≥65 years without clinical risk factors and (4) aged ≥65 years with ≥1 clinical risk factor,
individuals with increasing numbers of clinical risk factors.
Sensitivity analyses were conducted to investigate the impact of a) the method used for serotype designation and b) serotype 3 disease. Statistical analyses were conducted using Stata/IC V.15 (StataCorp, 2017).
Results
Study population
During the 5-year study period, of 3595 eligible patients, 158 (4.4%) patients had an alternative diagnosis and study consent was not obtained for 503 (14.6%). Patients without consent were older (median age 82.2 years, IQR 70.2–88.9 years vs 71.3 years, IQR 55.8–81.2 years, p<0.001), more often resident in care home facilities (35.0% vs 4.0%, p<0.001), more likely to have chronic kidney disease (12.8% vs 8.3%, p=0.001), cerebrovascular disease (21.2% vs 7.7%, p<0.001) and cognitive impairment (33.6% vs 3.7%, p<0.001), and less likely to have chronic respiratory disease (19.5% vs 27.9%, p<0.001) compared with the study cohort patients.
Baseline characteristics
The study cohort consisted of 2934 adults hospitalised with CAP between 2013 and 2018 (table 1); median age 71.3 years (IQR 55.8–81.2 years), 1515 (51.7%) male, and pneumonia severity low, moderate and high in 1377 (46.9%), 880 (30.0%) and 677 (23.1%) patients, respectively. Admission to intensive care occurred in 225 (7.7%) cases and overall 30-day case mortality rate was 7.5% (n=219).
Baseline characteristics, disease severity and outcomes of community-acquired pneumonia (CAP) cohort and pneumococcal CAP cohort
In 538 of 2934 patients, a urine sample was not available for pneumococcal testing. S. pneumoniae was identified in 1075 (36.6%) patients; Binax-NOW test was positive in 505 (47.0%) of 1075, Bio-plex24 in 973 (90.5%) and blood cultures in 111 (10.3%). One or more serotype was determined in 843 (78.4%) of 1075 patients with pneumococcal CAP; 2 serotypes were identified in 102 patients and ≥3 serotypes in 15 patients.
Trends in pneumococcal CAP
The overall annual incidence of CAP over the study period was 120.4 (95% CI 116.4 to 124.5) per 100 000 population. Annual incidence rates are presented in table 2. Incidence increased significantly over the 5-year period (annual incidence rate ratio (IRR) 1.12, 95% CI 1.09 to 1.14, p<0.001) (table 3). Adults aged ≥85 years demonstrated the greatest relative increase (115%) between 2013 and 2018 (annual IRR 1.24, 95% CI 1.17 to 1.31, p<0.001).
Incidence rates of community-acquired pneumonia (CAP), pneumococcal CAP and CAP due to vaccine and non-vaccine groups by study year
Linear trends and variation in CAP due to serotype groups, and non-vaccine serotype CAP
The overall annual incidence of pneumococcal CAP was 37.7 (95% CI 35.3 to 39.8) per 100 000 population. Pneumococcal CAP incidence rates increased over 5 years particularly in older age groups; for adults aged 65–74 years, 75–84 years and ≥85 years, annual IRR was 1.12 (95% CI 1.02 to 1·22, p=0·014), 1·20 (95% CI 1.09 to 1.32, p<0·001) and 1·15 (95% CI 1·03 to 1.28, p=0.014), respectively (table 3).
The overall annual incidence for CAP due to PCV7, PCV13non7, PPV23non13 and NVTs was 2·5 (95% CI 1.9 to 3.1), 12.2 (95% CI 11.0 to 13.6), 15.1 (95% CI 13·7 to 16.6) and 11·2 (95% CI 10.0 to 12.5) per 100 000 population, respectively (figure 1). The incidence of PCV13non7-serotype CAP (annual IRR 1·12, 95% CI 1.04 to 1.21, p=0·003) and NVT-serotype CAP (annual IRR 1.19, 95% CI 1.10 to 1.28, p<0·001) increased significantly over 5 years.

Incidence of serotyped pneumococcal CAP by vaccine groups between 2013 and 2018. Incidence per 100 000 adult population. PCV7-serotype CAP: CAP due to serotypes included in PCV7; PCV13non7-serotype CAP: CAP due to serotypes included in PCV13, excluding serotypes also included in PCV7; PPV23non13-serotype CAP: CAP due to serotypes included in PPV23, excluding serotypes also included in PCV13; non-vaccine-serotype CAP: CAP due to a) any non-PCV13, non-PPV23 serotype and B) untyped pneumococcal cases—blood culture or Binax urinary antigen detection positive without subsequent serotype identification, or Bio-plex24 assay positive for cell wall polysaccharide only. CAP, community-acquiredpneumonia; PCV, pneumococcal conjugate vaccine.
Pneumococcal serotypes
A total of 32 different serotypes were identified; 21 were definitively identified by Bio-plex24 or serum agglutination of bacteraemic cases while 11 were designated based on the predominant serotype derived from national IPD surveillance data (figure 2 and online supplementary appendix 2). Of the 11 designated serotypes, 9 matched the target serotypes, 1 was a different vaccine serotype (6A to 6C) and 1 was an NVT (15B to 15A). PCV7 serotypes were identified in 71 (6.6%) of the 1075 patients with pneumococcal CAP; serotype 19F was the most common (n=25, 33.3% of PCV7 serotypes), followed by serotype 14 (n=17, 22.7%) and 23F (n=11, 14.7%). PCV13non7 serotypes were identified in 349 (32.5%) patients, with serotype 3 being responsible for more than half of these cases (n=205, 56·9% of PCV13non7 serotypes).

Variation in absolute serotype numbers, grouped according to vaccine types, by study year among adults with pneumococcal CAP. PCV7-serotype CAP: CAP due to serotypes included in PCV7; PCV13non7-serotype CAP: CAP due to serotypes included in PCV13, excluding serotypes also included in PCV7; PPV23non13-serotype CAP: CAP due to serotypes included in PPV23, excluding serotypes also included in PCV13; non-vaccine-serotype CAP: CAP due to a) any non-PCV13-serotype, non-PPV23-serotype and B) untyped pneumococcal cases—blood culture or Binax urinary antigen detection positive without subsequent serotype identification, or Bio-plex24 assay positive for cell wall polysaccharide only. CAP, community-acquired pneumonia; PCV, pneumococcal conjugate vaccine.
PPV23non13 serotypes were identified in 431 (40.1%) patients; serotype 8 was the most common (n=197, 44.1% of PPV23non7 serotypes) followed by serotypes 12F (n=60, 13.4%), 11A (n=38, 8.5%), 22F (n=36, 8.1%) and 9N (n=35, 7·8%).
An NVT-serotype was identified in 321 (29.9%) patients, with serotype 15A identified in more than a quarter (n=80, 26.9% of NVT serotypes) while no serotype (‘untyped’ pneumococcal disease) was identified in 231 patients.
Compared with national IPD data over the same period,4 proportions of serotype 3 disease were higher for CAP while PPV23non13-serotype disease was higher in IPD (figure 3). The observed increase in serotype 3 pneumonia (annual IRR 1·28, 95% CI 1.24 to 1.32) was of similar magnitude to serotype 3 in IPD (annual IRR 1.23, 95% CI 1.12 to 1.36) (table 4 and figure 4).
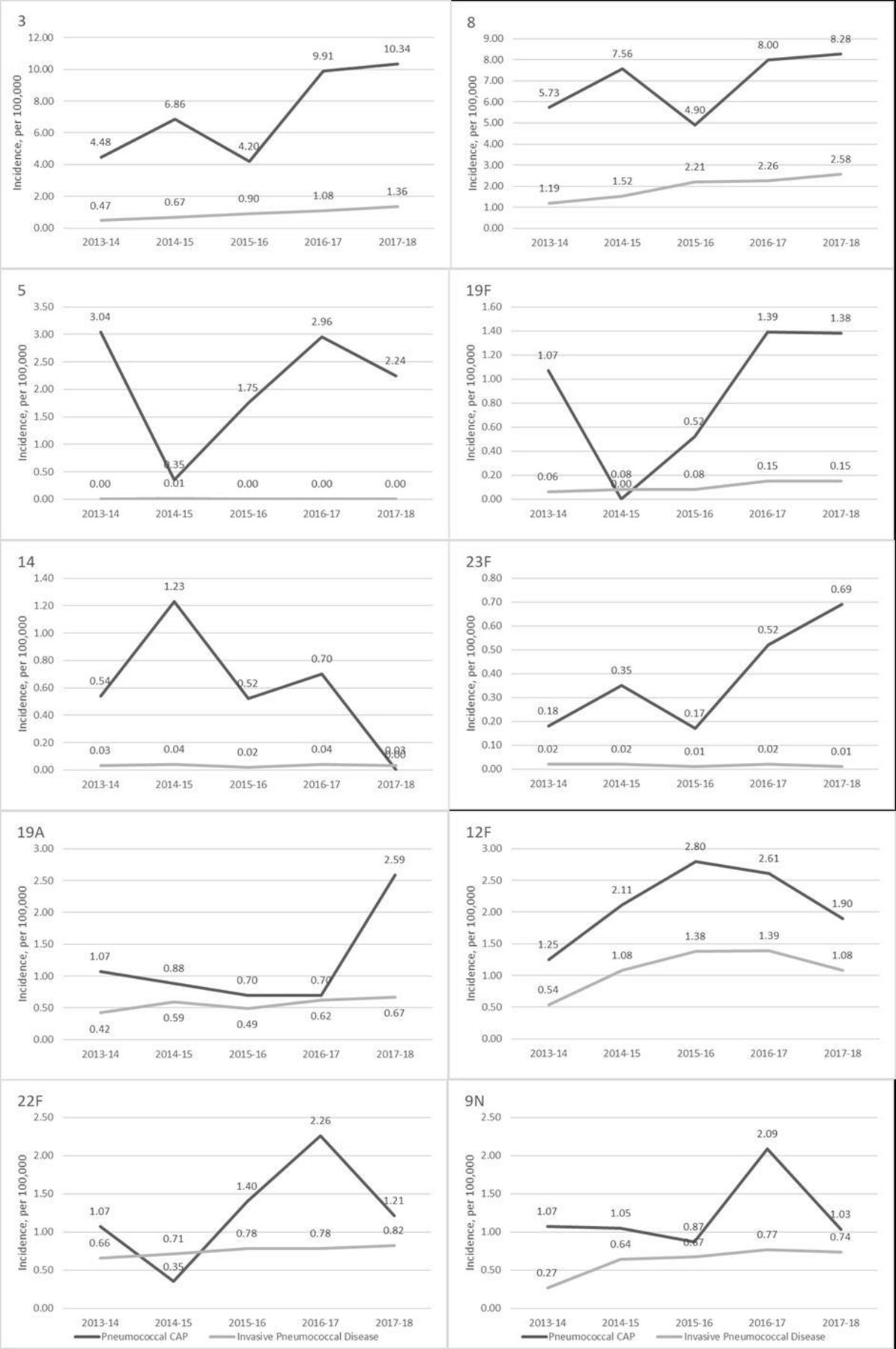
Overall trends in pneumococcal CAP and invasive pneumococcal disease incidence for individual serotypes between 2013 and 2018. Incidence per 100 000 adult population. IPD, invasive pneumococcal disease; CAP, community-acquired pneumonia.
Incident rate ratios (IRRs) for pneumococcal pneumonia cohort and IPD cohort between 2013 and 2018

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of serotype proportions between pneumococcal pneumonia cohort and national invasive pneumococcal disease cohort between 2013 and 2018. PCV7-serotype: pneumococcal disease due to serotypes included in PCV7; PCV13non7- serotype: pneumococcal disease due to serotypes included in PCV13, excluding serotypes also included in PCV7; PPV23non13-serotype: pneumococcal disease due to serotypes included in PPV23, excluding serotypes also included in PCV13; CAP cohort: non-vaccine-serotype: pneumococcal disease due to a) any non-PCV13-serotype, non-PPV23-serotype and b) untyped pneumococcal cases—blood culture or BINAX urinary antigen detection positive without subsequent serotype identification, or Bio-plex24 assay positive for cell wall polysaccharide only National IPD cohort: non-vaccine-serotype: pneumococcal disease due to any non-PCV13-serotype, non-PPV23-serotype case. CAP, community-acquired pneumonia; IPD, invasive pneumococcal disease; PCV, pneumococcal conjugate vaccine.
Persons with PCV13-serotype pneumonia
Of 983 patients eligible for analysis (single serotype, or multiple serotypes not crossing vaccine serogroup classes), 325 had PCV13-serotype and 658 had non-PCV13-serotype disease (online supplementary table 1). Increasing age (per year increase, adjusted OR (aOR) 1.02, 95% CI 1.01 to 1.03, p<0.001) and chronic kidney disease (aOR 1·71, 95% CI 1·02 to 2.86, p=0.019, respectively) were significantly associated with higher odds of PCV13-serotype disease compared with non-PCV13-serotype disease. Conversely, those living in residential care (aOR 0.28, 95% CI 0.10 to 0.75, p=0.012) or with active malignancy (aOR 0.52, 95% CI 0·31 to 0.90, p=0.019) had significantly lower odds of PCV13-serotype disease. On multivariate analysis, patients in the pneumococcal clinical risk group (aOR 1.73, 95% CI 1.31 to 2.28, p<0·001) and patients aged ≥65 years with ≥1 risk factor (aOR 1.69, 95% CI 1.24 to 2.30, p=0.001) had significantly higher odds of PCV13-serotype while patients aged 16–64 years without risk factors had significantly lower odds of PCV13-serotype disease (aOR 0.59, 95% CI 0.43 to 0.81, p=0.001) (table 5).
Association between clinical risk group and PCV13-serotype disease
Sensitivity analysis excluding all cases with designated serotypes (n=157) did not significantly alter findings. Conversely, none of the described associations remained significant when all serotype 3 cases were excluded.
Persons with PPV23 serotype pneumonia
Of 1048 patients eligible for analysis (single serotype, or multiple serotypes not crossing vaccine serogroup classes), 732 had PPV23-serotype and 316 had non-PPV23-serotype disease (online supplementary table 2). There were no significant associations between risk of PPV23 serotype disease and individual comorbidities identified in the multivariate analysis. On multivariate analysis of clinical risk and PPV23 serotype disease, both the pneumococcal clinical risk group (aOR 0·65, 95% CI 0·48 to 0·88, p=0·006) and patients aged 16–64 years with ≥1 risk factor (aOR 0·51, 95% CI 0·35 to 0·73, p<0·001) had significantly lower odds of PPV23-serotype disease (table 6). Patients aged 16–64 years without risk factors had significantly higher odds of PPV23-serotype disease (aOR 1·54. 95% CI 1·13 to 2·10, p=0·006).
Association between clinical risk group and PPV23-serotype disease
Sensitivity analyses excluding 1) all cases with designated serotypes (n=183) and 2) all cases of serotype 3, from the model did not significantly alter findings (online supplementary data, supplementary tables 3 and 4).
An exploratory analysis to identify persons at risk of PPV23non13-serotype disease found that patients aged 16–64 years without risk factors had significantly higher odds of PPV23non13-serotype disease (aOR 1·94, 95% CI 1·42 to 2·65, p<0·001), while patients aged ≥65 years with ≥1 risk factor (aOR 0·69, 95% CI 0·51 to 0·94, p=0·017) and pneumococcal clinical risk group (aOR 0·52, 95% CI 0·38 to 0·70, p<0·001) had significantly lower odds of PPV23non13-serotype disease compared with non-PPV23non13-serotype disease.
Discussion
The key study findings are 1) the annual incidence of adult pneumococcal CAP has increased from 32·2 per 100 000 population in 2013 to 48·2 per 100 000 population in 2018, concurrent with increases in the incidence of overall CAP, 2) this increase is predominantly due to increases in PCV13non7-serotype and NVT-serotype pneumonia, 3) serotype 3 accounts for more than half of PCV13non7-serotype pneumonia, 4) PCV13-serotype pneumonia is 73% more likely in patients in pneumococcal clinical risk group, while 5) PPV23-serotype pneumonia is 54% more likely in younger patients who are not in the pneumococcal clinical risk group.
The epidemiology of adult pneumococcal pneumonia in Europe appears to be diverging from that seen in the USA. We found evidence of pneumococcal infection in more than a third of adults hospitalised with CAP, consistent with other recent reports from Europe.17 18 In contrast, in the USA, S. pneumoniae has been recently implicated in only 8%–12% of hospitalised cases of CAP.19 20 During 2008–13, we had observed early indications of a decline in CAP due to PCV13 serotypes in adults following PCV7 substitution with PCV13 in the childhood immunisation programme. However, our latest findings in a previously untested and unreported cohort of patients from Nottingham indicate that PCV13 serotypes continue to account for a large proportion (40·6%) of adult CAP, with serotype 3 alone comprising 47·1% of PCV13 serotype cases. Pneumococcal carriage studies21 22 and national surveillance of IPD5 have also observed a limited direct and indirect effect of PCV13 vaccination on serotype 3. These results are consistent with data indicating the serotype 3 antigen within PCV13 may provide suboptimal direct and indirect protection.23 Notwithstanding serotype 3, there appears to be a persistence of PCV13 serotypes causing CAP. Serotypes 3, 5 and 6A were relatively more common in CAP compared with IPD, possibly indicating a predilection for pneumonia (rather than IPD) with these serotypes, as also observed by others.24 25
We identified multiple serotypes in 10.9% of patients with pneumococcal pneumonia. This is higher than the proportion with multiple serotypes identified in IPD cohorts. The relevance and implications of this finding warrants further investigation.
Based on data from 2008 to 2013, we previously reported that PCV13-serotype CAP was less common in adults in the pneumococcal clinical risk group compared with adults aged 16–64 years without clinical risk factors.26 Those data reflected the situation within the first few years after introduction of the childhood PCV13 immunisation programme. Since then, the burden of PCV13-serotype CAP has shifted and adults in pneumococcal clinical risk group are at increased risk of infection. This association is dominated by serotype three which may reflect the invasiveness potential of this serotype, its penchant for pneumonia (compared with IPD) and its persistent carriage among children and adults. The influence of the recently emerged Clade II lineage (of serotype 3) in relation to clinical disease presentation is unclear.27 28
A large proportion of pneumococcal CAP was due to PPV23non13-serotype pneumonia (40·2%) with no significant change in incidence during 2013–18. Serotype 8 was the most common, similar to national IPD trends.4 Although carriage of serotype 8 in children is rare, colonisation in young adults has been observed and may represent the reservoir from which adult pneumococcal infections arise.29 In England and Wales, uptake of PPV23 vaccination in older adults and pneumococcal clinical risk groups has remained stable (~70%) over the study period.30 The lack of significant change in the incidence of PPV23non13-serotype pneumonia suggests the replacing serotypes in pneumococcal pneumonia are predominantly NVT serotypes not covered by either PCV13 nor PPV23 vaccines. This is consistent with the observed increase in incidence of NVT-serotype pneumococcal pneumonia both in this study, and in other cohorts.4 8
We found the odds of PPV23-serotype CAP was higher in patients outside the pneumococcal clinical risk group, specifically in patients aged 16–64 years without risk factors (aOR 1·54), but lower in patients in the pneumococcal clinical risk group (aOR 0·61). These associations were amplified when the analyses were restricted to patients with PPV23non13-serotype pneumonia (aOR 2·39 and 0·42) and could reflect individual direct protection offered by PPV in ‘at-risk’ adults.31
Strengths and limitations
This large prospective population-based cohort study describes trends in pneumococcal serotypes implicated in adult pneumococcal pneumonia over the last 5 years, during which PCV13 replaced PCV7 in the national childhood immunisation programme. Unlike laboratory-based studies, our study population is not over-represented by patients with chronic lung disease or those requiring invasive respiratory procedures.25 Use of the novel Bio-plex24 assay enabled identification of PCV13 and PPV23 serotypes in patients presenting with non-invasive disease, which is the vast majority of adults with CAP, compared with previous studies which have been unable to identify PPV23-non13-serotype disease from non-invasive samples and have classified these cases as non-vaccine-type infection only.
We observed an increased incidence in all-cause CAP and pneumococcal CAP over a 5-year period which we have interpreted as representing a true increase in disease burden. We cannot exclude the possibility that some of this increase may have been due to healthcare system changes resulting in a shift from primary to secondary care management for CAP. However, the lack of any substantial change over time in the distribution of low versus high severity pneumonia on admission suggests this is unlikely to be a major factor.
One limitation of this study relates to cross-reactivity of the Bio-plex24 assay. Non-specific cross-reactivity for serotypes 7F, 18C, 20 and 22F was noted during testing of samples from September 2014 to August 2015. We chose to report results conservatively, accepting some under-representation of serotypes 7F, 18C, 19F, 20 and 22F for that year. Following modifications to the assay, this non-specific cross-reactivity did not affect results for the other 4 years. For 11 serotypes displaying cross-reactivity with other serotypes not targeted by the Bio-plex24 assay, we designated cases to a single serotype based on the predominant serotype derived from national IPD data. A consequence of this methodology is the potential under-representation of less frequent serotypes. In sensitivity analyses investigating the influence of the method of serotype designation on results, no major differences were detected (online supplementary data available on request). Any overall under-representation of NVT serotypes arising from serotype designation would mean that our reported finding of an increased incidence of NVT-serotype CAP is conservative.
Second, all untyped pneumococcal isolates were considered NVT serotypes, potentially leading to an over-representation of NVT-serotype CAP. The impact of this on the overall findings is likely to be small given the high sensitivities of the serotyping methods used.
Additionally, as this study was performed in one geographical area, the serotype trends observed may have been due to local/regional epidemiological changes and our findings may not be applicable to other populations. Nevertheless, the main findings are consistent with trends observed from national IPD data.
Implications
We report an increase in pneumococcal CAP, predominantly due to increases in NVT serotypes and serotype 3. Pneumococcal vaccines targeting emerging serotypes are needed.
Acknowledgments
The authors would like to thank Tim Harrison, Elizabeth Thomas, Pamela Sandu and Sally-Ann Nguyen from the Respiratory and Vaccine Preventable Bacteria Reference Unit, Public Health England (RVPBRU), Colindale for their support; Robert Cave, Matthew Bonsall, Kimberley Coultas, Kerry Hannon, Laura Kirby, Laura Lloyd, Leia-Marie Thacker and colleagues from Department of Clinical Microbiology, Nottingham University Hospitals, for processing the urine specimens using the BinaxNOW assay; the clinicians and staff of Nottingham University Hospitals NHS Trust; the Nottingham Pneumonia Patient and Public Involvement group for their ongoing input to respiratory infection research and all participants who gave their consent for this study.
References
Footnotes
Contributors HJP, CS and WSL were responsible for study conception and design. HJP, PD, CR, TB, DA, HL, VB, RCE-P, CS and SE were responsible for data acquisition. HJP, TMM and CT were responsible for the statistical analysis. HJP and WSL drafted the initial versions of the Article. All authors contributed to data interpretation and read, commented on and approved the final version of the article.
Funding This study is independent research supported by the Nottingham National Institute for Health Research Biomedical Research Centre (NIHR BRC) and arising from an unrestricted investigator-initiated research grant from Pfizer. The study concept was developed and agreed by the authors with no input from the funding bodies; Pfizer had no part in the design or execution of the study, the analysis and interpretation of the results, the writing of this manuscript or the decision to submit for publication. The data are the sole responsibility of the authors and the sponsor for the study was Nottingham University Hospitals NHS Trust.
Disclaimer The views expressed in this publication are those of the authors and not necessarily those of the NHS, the NIHR or PHE.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Study procedures were approved by the Nottingham Research Ethics Committee (REC reference 08/H0403/80).
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves
- Editorial