Article Text

Abstract
Introduction Adult spirometry following community-acquired childhood pneumonia has variably been reported as showing obstructive or non-obstructive deficits. We analysed associations between doctor-diagnosed childhood pneumonia/pleurisy and more comprehensive lung function in a middle-aged general population cohort born in 1961.
Methods Data were from the prospective population-based Tasmanian Longitudinal Health Study cohort. Analysed lung function was from ages 7 years (prebronchodilator spirometry only, n=7097), 45 years (postbronchodilator spirometry, carbon monoxide transfer factor and static lung volumes, n=1220) and 53 years (postbronchodilator spirometry and transfer factor, n=2485). Parent-recalled histories of doctor-diagnosed childhood pneumonia and/or pleurisy were recorded at age 7. Multivariable linear and logistic regression were used.
Results At age 7, compared with no episodes, childhood pneumonia/pleurisy-ever was associated with reduced FEV1:FVC for only those with current asthma (beta-coefficient or change in z-score=−0.20 SD, 95% CI −0.38 to –0.02, p=0.028, p interaction=0.036). At age 45, for all participants, childhood pneumonia/pleurisy-ever was associated with a restrictive pattern: OR 3.02 (1.5 to 6.0), p=0.002 for spirometric restriction (FVC less than the lower limit of normal plus FEV1:FVC greater than the lower limit of normal); total lung capacity z-score −0.26 SD (95% CI −0.38 to –0.13), p<0.001; functional residual capacity −0.16 SD (−0.34 to –0.08), p=0.001; and residual volume −0.18 SD (−0.31 to –0.05), p=0.008. Reduced lung volumes were accompanied by increased carbon monoxide transfer coefficient at both time points (z-score +0.29 SD (0.11 to 0.49), p=0.001 and +0.17 SD (0.04 to 0.29), p=0.008, respectively).
Discussion For this community-based population, doctor-diagnosed childhood pneumonia and/or pleurisy were associated with obstructed lung function at age 7 for children who had current asthma symptoms, but with evidence of ‘smaller lungs’ when in middle age.
- clinical epidemiology
- respiratory infection
Statistics from Altmetric.com
Key messages
What is the key question?
What is the relationship between childhood pneumonia and comprehensive lung function measures in a general population-based cohort currently in middle age?
What is the bottom line?
Doctor-diagnosed childhood pneumonia and/or pleurisy were associated with obstructed prebronchodilator spirometry at age 7 for children who had current asthma symptoms, but with reduced static lung volumes when in middle age.
Why read on?
For the first time, this prospective study has used static lung volume and carbon monoxide transfer factor measurements to complement spirometric data from childhood to middle age, to further understanding of childhood pneumonia and/or pleurisy and their association with lung physiology across the life course.
Introduction
In the preantibiotic era, bacterial pneumonia was frequently associated with lung abscesses, empyema, septicaemia and/or death.1 While widespread access to antibiotics and immunisation has reduced these adverse outcomes predominantly in developed countries, the global health burden from pneumonia and lower respiratory tract illnesses still remains high,2 with respiratory viruses commonly identified as pathogens.3 4 Thus, information on the long-term consequences of childhood pneumonia in the antibiotic era has ongoing importance.
Whether childhood pneumonia predisposes to reduced adult lung function and/or COPD is controversial.5 6 Of the five prospective population-based studies that have examined the association between childhood pneumonia and postbronchodilator (BD) spirometry in adults,3 7–10 two have observed airflow obstruction,3 7 while three have found spirometric restriction (reductions in both post-BD FEV1 and FVC with a preserved forced expiratory ratio (FEV1:FVC)).8–10 These conflicting physiological patterns were not clearly related to the preantibiotic7–9 versus antibiotic era,3 10 nor to older (55–75 years) versus younger adults (<40 years). However, the magnitude of spirometric deficits attributed to early childhood pneumonia was greatest in preantibiotic cohorts (FEV1: 0.65 L7 and FVC: 0.67 L9). The most recent birth cohort study examined radiologically confirmed childhood pneumonia and lower respiratory tract infections (LRTI) separately and reported pneumonia-related airflow obstruction with greater FEV1 deficits up to age 22 years and LRTI-related reductions in FVC at age 26.3 Using group-based trajectory modelling, our research group has previously reported associations between doctor-diagnosed childhood pneumonia/pleurisy and lower pre-BD FEV1 trajectories across the life course, and shown how obstructed airway function in middle age was related to a combination of childhood pneumonia, asthma and bronchitis.11 12 Notably, none of these previous analyses reported on static lung volumes in relation to either obstruction or restriction, nor on carbon monoxide transfer factor (TLco) to assess lung parenchymal function.
Quantifying the lung function influence of childhood pneumonia across the life course is clinically important given the evolving link between early life respiratory factors and predisposition to COPD.6 12 Using data from the whole-of-community cohort born in 1961 in Tasmania, Australia, we aimed to investigate the lung function consequences of doctor-diagnosed childhood pneumonia/pleurisy using serial spirometry spanning childhood and middle age, and for the first time post-BD TLco and static lung volumes.
Materials and methods
Study design and population
Our study sample included those participants of the Tasmanian Longitudinal Health Study cohort (TAHS 1968–2015) who took part in three clinical studies at the mean ages of 7, 45 and 53 years. Details have been published elsewhere.13–18 Briefly, this population-based cohort born in 1961 (n=8583) and studied with spirometry in 1968 (aged 6–7 years) was retraced (n=7312)16 and resurveyed by questionnaire. Of 5729 respondents, those who had participated in a 1974 and/or 1992 clinical follow-up visit and/or had adult respiratory symptoms were invited to undertake spirometry (pre-BD and post-BD), TLco and static lung volumes between 2006 and 2008. Of 2373 invitees, 58.5% (n=1389) attended.
Of the full original cohort, 6127 were traced and invited to participate in the subsequent 2012 clinical study, with 3609 (58.9%) completing the questionnaire and 2689 (43.9%) undergoing spirometry and TLco measurements. Of those tested, 897 had lung function measurements from the previous laboratory study (figure 1).

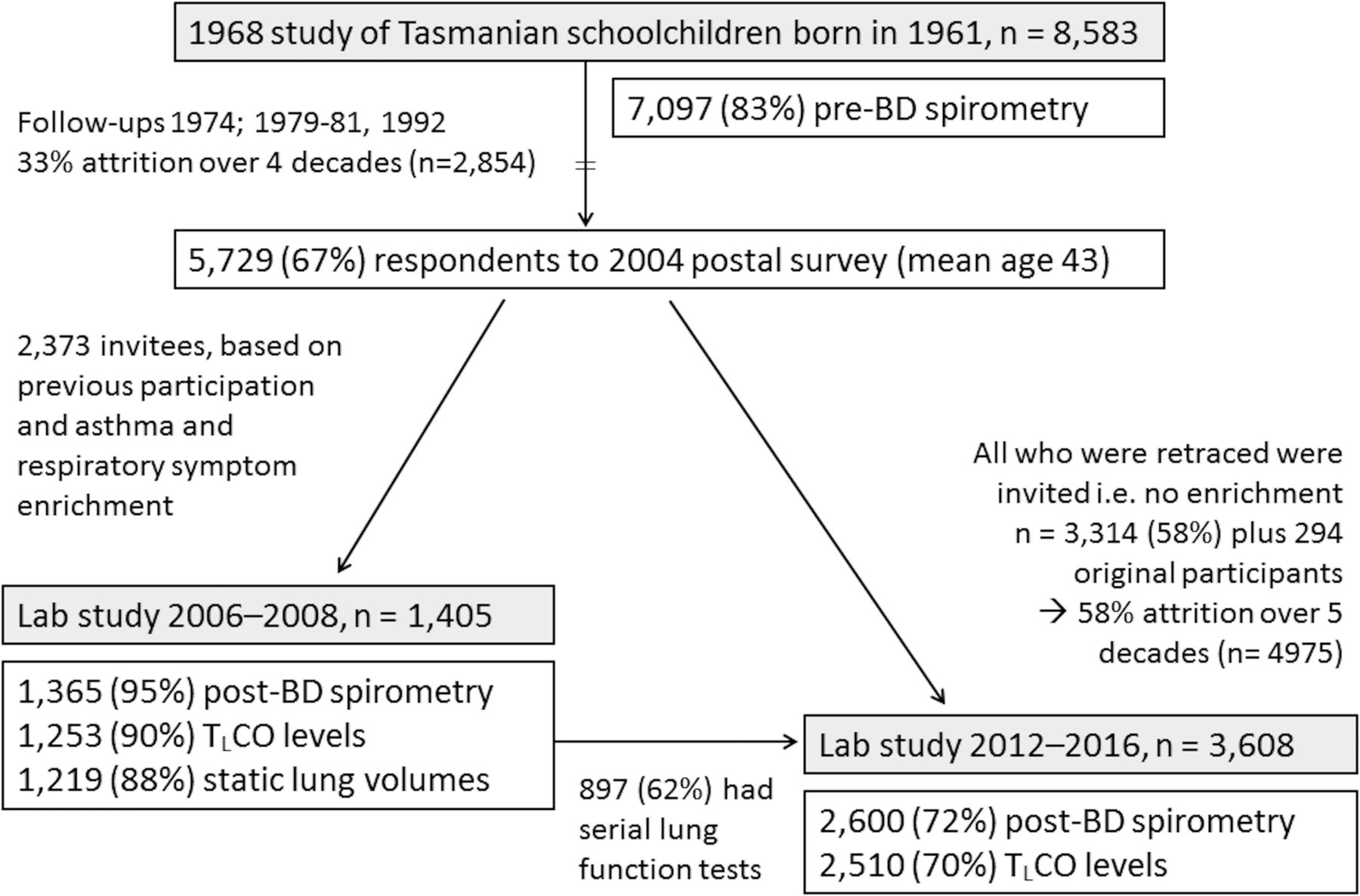{kind=link}
TAHS participants of the present analysis (1968–2016). BD, bronchodilator; TASH, Tasmanian Longitudinal Health Study; TLco, carbon monoxide transfer factor.
Data collection methods
Details of lung function testing have been described15 and summarised in online supplementary data, methods E1. The measurements of lung function were standardised across testing sites and followed the 2005 American Thoracic Society/European Respiratory Society standards for technically acceptable lung function testing based on repeatability criteria for spirometry, TLco and static lung volumes.19–21 For this analysis, lung function data at a mean age of 7, 45 and 53 were converted to z-scores (ie, SD units) using established standard reference values22 23 and equations.24
Supplemental material
Clinical definitions
Childhood pneumonia and/or pleurisy was defined by a parent’s affirmative response to the 1968 survey question ‘Have you ever been told by a doctor that he/she had pneumonia or pleurisy’, followed by the prespecified options of ‘No, never’, ‘Yes, once or twice’, and ‘Yes, more than twice’. These categories correspond to childhood pneumonia/pleurisy-never, infrequent childhood pneumonia/pleurisy, and recurrent childhood pneumonia/pleurisy in the main text, respectively. Childhood pneumonia/pleurisy-ever combines the latter two categories (≥1 episode). Other relevant definitions are included in online supplementary methods E2.
Postbronchodilator airflow obstruction (post-BD AO) was defined by FEV1:FVC <5th percentile of predicted values following 200 µg of salbutamol administered via spacer (z-score <–1.645 SD).22 Spirometric restriction was defined by post-BD FVC <5th percentile of predicted values in the absence of post-BD AO.
Statistical analysis
All analyses were carried out using Stata V.14. Univariable trends of continuous/categorical lung function data were examined across ordered categories using the non-parametric trend test (‘nptrend’)25 and ordinal logistic regression, respectively. Multivariable linear/logistic regression was used to examine associations with continuous/categorical lung function outcomes using two different classifications: (1) childhood pneumonia/pleurisy as a binary exposure (ever or never); and (2) a multilevel exposure consisting of never (0), infrequent (1–2) and recurrent (>2 episodes). The regression coefficients represent the associations between exposures and lung function values expressed as z-scores (SD units) (online supplementary methods E3).
Models were adjusted for known confounding of the pneumonia–lung function relationship, namely categorical variables of maternal/paternal smoking, socioeconomic status (paternal occupation, rurality of primary school) and history of breast/bottle feeding.26 27 Where applicable, models were adjusted for sampling weights, being the inverse of the probability of being included in the sample. Childhood lung function measured at the time of the original survey and current childhood asthma were considered potential intermediaries and/or mediators.2 3 28 29 This approach was supported for the latter by performing causal mediation analysis,30 31 which estimated the per cent of the total effect mediated by current childhood asthma to be 72.5% and 55.6% for FEV1/:FVC as continuous and categorical variables at age 7, respectively (online supplementary data, table E4). Thus pneumonia–childhood asthma interactions were investigated, also to provide estimates for participants without symptomatic asthma at age 7. Biologically plausible sex-related differences and effect modification by smoking status (never vs ever-smokers) were also examined. These analyses were performed using childhood pneumonia/pleurisy-ever as a binary variable, and stratified results were reported if a statistical interaction was identified.
Missing exposure/confounding data ranged between 0% and 6% per variable (online supplementary data, tables E1 and E2), so complete case analysis was performed. A conventional cut-off of p<0.05 was used to determine statistical significance for the main associations and p<0.10 for interactions.
Results
Demographic and clinical features
Clinical characteristics and lung function data have been published.15 At age 7, 14.2% (n=1172) of participants had had childhood pneumonia/pleurisy-ever, more commonly for males than females (15.3% (95% CI 14.2 to 16.4) vs 13.1% (95% CI 12.0 to 14.1), respectively, p=0.004). This baseline prevalence was similar when the population was restudied at two time points in middle age, after taking sampling weights into account (13.4%–14.4%; table 1).
Demographic characteristics of TAHS participants, stratified by history of childhood pneumonia/pleurisy
Other than an increased prevalence of current asthma and chronic bronchitis with symptom enrichment at age 45, there were no other appreciable differences in baseline characteristics when compared with the original survey at age 7 and subsequent follow-ups (online supplementary tables E1 and E2). Specifically, after accounting for sampling weights, the percentage with doctor-diagnosed childhood pneumonia/pleurisy (13.6%–16.0%) and z-score distributions of childhood lung function (0.00–0.12 SD) were similar between those participating and not participating in each of the three follow-ups (online supplementary table E3).
Spirometry at age 7
At age 7, pre-BD FEV1 and FEV1:FVC levels were reduced (p trend ≤0.01), and the odds for airflow obstruction increased across ordered childhood pneumonia/pleurisy categories (p trend=0.008; table 2). In multivariable models, across all participants, childhood pneumonia/pleurisy-ever was associated with reduced FEV1:FVC when analysed as a continuous variable (z-score –0.09 SD (–0.16 to –0.02), p=0.012; table 3). However, when the analysis was stratified by current childhood asthma status, the association for childhood pneumonia/pleurisy-ever compared with no history was seen in children who had current childhood asthma (z-score –0.20 (95% CI –0.02 to –0.38), p=0.028) but not those without (–0.003 (–0.1 to +0.1), p=0.94, p interaction=0.036; online supplementary data, table E5).
Number of participants and baseline lung function of TAHS laboratory study participants, stratified by childhood history of pneumonia/pleurisy
Multivariable associations between doctor-diagnosed childhood pneumonia-pleurisy, FEV1 and measures of airflow obstruction from childhood to middle age
For the smaller subgroup with recurrent episodes, childhood pneumonia/pleurisy was associated with reduced FEV1 (z-score –0.25 SD (95% CI –0.5 to –0.04), p=0.021; table 3) and an increased odds for airflow obstruction in childhood (OR 2.71 (1.3 to 5.7), p=0.009; table 3) compared with no history. Infrequent, recurrent and childhood pneumonia/pleurisy-ever were associated with reduced FEV1:FVC (p<0.05), especially for males (z-score –0.14 (–0.2 to –0.05), p=0.003, p interaction=0.104; online supplementary table E6).
Neither recurrent nor ever childhood pneumonia/pleurisy was associated with reduced FVC analysed as either a continuous or categorical variable (p>0.146; table 4). Effect modification of these relationships by childhood asthma was not seen (p interaction >0.43; online supplementary table E5).
Multivariable associations between doctor-diagnosed childhood pneumonia-pleurisy, FEV1 and measures of spirometric restriction from childhood to middle age
Spirometry in middle age
At both ages 45 and 53, the odds for spirometric restriction increased across ordered childhood pneumonia/pleurisy categories (p trend <0.009; table 2), with some evidence for decreasing post-BD FEV1:FVC at age 53 only (p=0.059).
At age 45, although childhood pneumonia/pleurisy-ever was not associated with post-BD FEV1, recurrent episodes corresponded to reductions in FEV1 equivalent to 0.46 SD (95% CI 0.01 to 0.9, p=0.045) compared with no history (table 3). There was a 3.02-fold increase in the odds for adult spirometric restriction for childhood pneumonia/pleurisy-ever compared with no history (95% CI 1.5 to 6.0, p=0.002; table 4).
Effect modification of the pneumonia-spirometry relationship by childhood asthma was seen. Specifically, the odds of having airflow obstruction were reduced for childhood pneumonia/pleurisy-ever compared with no history, but for only those without childhood asthma (OR 0.31 (95% CI 0.1 to 0.9), p=0.028 vs 1.64 (0.8 to 3.5), p=0.20 with asthma, p interaction=0.020; online supplementary table E5). This was complemented by higher post-BD FEV1:FVC levels for those without current childhood asthma (z-score +0.27 SD (95% CI +0.1 to +0.5), p=0.004 vs –0.04 (–0.3 to +0.3), p=0.78 with asthma, p interaction=0.079; online supplementary table E5). The odds for spirometric restriction were statistically greater for females than males at the 45-year follow-up (p interaction=0.042; online supplementary table E6), without modification by adult smoking status (online supplementary table E7).
At age 53, childhood pneumonia/pleurisy-ever was associated with similar reductions in post-BD FEV1 and FVC analysed as continuous variables (z-scores –0.16 SD (95% CI –0.28 to –0.04), p=0.009 and –0.11 SD (–0.22 to –0.001), p=0.047, respectively). There was modest evidence for an association between recurrent childhood pneumonia/pleurisy and spirometric restriction (OR=3.91 (0.86 to 17.7), p=0.076, n=25). Childhood asthma symptoms at age 7, participant sex and adult never/ever-smoking status did not modify any of these pneumonia–spirometry relationships (p interaction >0.20; online supplementary tables E5–E7). However, the estimate for pneumonia-related spirometric restriction was statistically significant only for those who had current childhood asthma at age 7 and not for those without, seen at both time points in middle age (online supplementary table E5).
Static lung volumes at age 45
Total lung capacity (TLC) and functional residual capacity (FRC) were reduced across increasing childhood pneumonia/pleurisy categories (p trend <0.01; table 2). This dose–response relationship with TLC was especially evident for never smokers compared with ever-smokers (p trend=0.006 vs 0.132, respectively).
In multivariable models, childhood pneumonia/pleurisy-ever was associated with reductions in adult TLC compared with no history (z-score –0.24 SD (95% CI –0.37 to –0.12), p<0.001; table 5). This deficit corresponded to an absolute reduction in TLC of 225 mL (95% CI 104 to 346 mL) or 3.97 (2.0 to 5.9) % predicted. The statistically significant reductions in TLC, FRC and RV were greater for never smokers compared with ever-smokers, although estimates were not statistically different between the two groups (p interaction=0.104, 0.146 and 0.120, respectively; online supplementary table E7). The pneumonia–TLC relationship was not modified by the presence of current asthma at age 7 (p interaction=0.63; online supplementary table E5), but was more pronounced for males compared with females (z-score –0.29 SD (–0.5 to –0.1), p=0.002 vs –0.14 SD (–0.30 to +0.01), p=0.075, p interaction=0.193), while FEV1:FVC was reduced for males only (–0.14 SD (–0.24 to –0.05), p=0.003, p interaction=0.104; online supplementary table E6).
Multivariable associations between doctor-diagnosed childhood pneumonia-pleurisy and static lung volumes in middle age
TLco in middle age
Childhood pneumonia/pleurisy-ever was associated with increases in carbon monoxide transfer coefficient (Kco) (ie, TLco per unit of accessible alveolar volume) at ages 45 and 53 years, compared with no history (z-score +0.29 SD (95% CI +0.1 to +0.5), p=0.001 and +0.17 SD (+0.04 to +0.3), p=0.008, respectively; table 6). The main associations between childhood pneumonia/pleurisy-ever and TLco were also in the same direction at both time points, although not statistically significant. No sex-related differences were seen (online supplementary table E6), and there was no clear pattern of effect modification by current childhood asthma and smoking status (online supplementary tables E5 and E7).
Multivariable associations between doctor-diagnosed childhood pneumonia-pleurisy and transfer factor in middle age
Discussion
In our prospective population-based cohort born in 1961, which is the first such study to measure comprehensive lung function in middle age, we found parental report of doctor-diagnosed childhood pneumonia and/or pleurisy was associated with mildly obstructive spirometry in childhood for the subgroup who had current asthma in childhood that was not seen in later life. Childhood pneumonia and/or pleurisy were associated with dose–response trends in TLC and FRC, as well as reductions in TLC, FRC and residual volume, across all middle-aged participants, which were more pronounced for never smokers. Unexpectedly, we found coexistent pneumonia-related increases in the efficiency of alveolar transfer of carbon monoxide (Kco) at the two time points in middle age, without a consistent pattern when stratified by sex, asthma and smoking subgroups. While these results are not straightforward to interpret, these findings would be consistent with childhood pneumonia and/or pleurisy being associated with smaller lungs in middle age, with higher Kco reflecting a more efficient distribution of pulmonary capillary blood flow over a smaller alveolar surface.
Whether early childhood community-acquired pneumonia predisposes to the development of COPD in later life has been subject to a long and ongoing debate.5 Our data support doctor-diagnosed childhood pneumonia and/or pleurisy reducing lung function in an obstructive pattern only in childhood at a general population level; however, we saw this pattern only for children who had recent asthma symptoms and found no association for those without. In the Tucson Children’s Respiratory Study, which followed a cohort of participants born 1980–1984 from birth up to their early 20s, childhood pneumonia was associated with incident asthma and airflow obstruction was the predominant airway pattern seen.3 For this more recent Tucson cohort, pneumonia was confirmed radiologically and the predominance of viral-related pneumonia was confirmed serologically, but unfortunately the results were not stratified for asthma. Hypothetically, this obstructive decrement in childhood might contribute to later COPD development by reducing peak adult lung function.6 32 Nonetheless, we acknowledge that in our TAHS cohort, the average magnitude of lung function deficit was modest. Thus, the contribution of childhood pneumonia-pleurisy itself to the development of COPD may be only clinically important for a vulnerable minority of the general population who have other predisposing factors.
Our observations during middle age most closely resemble findings from the British 1958 Birth Cohort, also born during the antibiotic era, which documented reductions in post-BD FEV1 and FVC with a preserved FEV1:FVC.10 We found this association for participants who had recurrent childhood pneumonia/pleurisy, and this was supported by dose–response trends. Our spirometric findings extend those of the UK cohort by documenting a lack of spirometric restriction in childhood raising the possibility of impaired lung or chest volume growth through later childhood, adolescence and potentially early adulthood. This concept is supported by data from a South African study which documented a temporal relationship between early lower respiratory tract illnesses and impaired lung function at 12 months as measured by multiple breath washout techniques during quiet natural sleep.2 Importantly, this study largely excluded the possibility of preceding low lung function (at 6 weeks) being associated with an increased risk of LRTI during the first year of life, providing some evidence that early life lung function is a likely mediator and unlikely confounder of the pneumonia–adult lung function relationship in our study. However, whether our data could be confounded by pneumonia occurring more commonly in those from more developed countries with lesser premorbid lung function remains possible.33 34 Since we do not have sufficient supporting early data such as birth weight or lung function measurements prior to the pneumonic illness, the observed reductions in adult TLC and FRC might be related to confounding, as being born prematurely or small for dates may increase the risk for both childhood pneumonia and low lung function trajectories. However, the similar analysis of this UK cohort did adjust for birth weight and birth order.10
Even at the age of 7 years, as was the case in the British 1958 Birth Cohort, recent recall by parents could have been subject to some error. While it is quite possible that parents were more likely to recall a history of pneumonia for a child who also had wheezy breathing and/or asthma,35 it is unlikely to explain our predominant finding of spirometric restriction in early middle age. Furthermore, our study specifically asked parents about doctor-diagnosed pneumonia and/or pleurisy, which presumably is more objective and less subject to recall bias than parental report only. Conversely, the potential for unreliable recall by parents (especially for pneumonia occurring 5–6 years earlier) and bias of the presenting symptoms depending on the child’s asthma status might have led to some misclassification of wheezy illness as being pneumonia in children with asthma.
While our results might have been influenced by asthma enrichment when participants were aged 45 as a potential explanation for results at age 53 being less marked despite greater power, it is possible that the participants studied at age 45 may have had more severe pneumonia and/or more frequent pleurisy. Alternatively, the influence from childhood-related insults might lessen during middle age with relatively increasing contributions from accumulating adult factors. Notably, the British 1958 Birth Cohort, which also found restriction, was from an unselected general population. Inhaled corticosteroid therapy for asthma did not become widely available until the early 1970s, so its risk for potentiating pneumonia is unlikely to have been implicated when our cohort was first studied at age 7. However, this pneumonia–asthma association has been documented subsequently.3 29
We acknowledge that our definition of childhood pneumonia-pleurisy almost certainly included some viral pleurisy as well as complicated bacteria-related pleural effusions. This raises the possibility of a degree of extrapulmonary restriction. Although still relevant to populations born in or before the 1960s, more recent management practices limit the generalisability of our results to childhood pneumonia diagnosed in the present day, at least in Westernised countries. Interestingly, a meta-analysis of data published prior to the 1980–1984 cohort study reported a predominance of non-obstructive spirometric patterns after childhood pneumonia, with any obstruction mainly related specifically to adenoviral infection.36
Strengths and limitations
The TAHS is prospective over six decades, and is the first study to quantify the relationship between childhood pneumonia/pleurisy, childhood spirometry and complex lung function in middle age. This was done using z-scores derived from the Global Lung Function Initiative reference values, which effectively minimised anthropometric bias.22 23 While we were able to assess for ‘dose-response’ trends, we were limited in statistical power by relatively small numbers for the subgroup with recurrent childhood pneumonia/pleurisy. While the ‘healthy survivor effect’ might have underestimated our estimates, older preantibiotic cohorts would have been more susceptible to this form of bias.7–9 This analysis has provided supportive evidence for a causal association, especially with the documentation of a temporal and dose–response relationship, as well as consistency of spirometry findings between both TAHS follow-ups in middle age and a similar independent cohort.10 However, as with all observational studies, we are not able to exclude the possibility of an unmeasured confounder having generated these apparent associations.
Regarding our exposure variable, as the TAHS started as a large whole-of-population study in Tasmania in the 1960s (n=8583), it was not feasible to radiologically confirm cases of childhood pneumonia for the entire cohort. Likewise it was not possible to identify causative bacteria or viruses (notably respiratory syncytial and adenovirus) that may predispose to the development of airflow obstruction in later childhood.34 36–38 Further details regarding age of occurrence, severity, hospitalisation and future episodes were also not recorded. Categorisation of age at pneumonia would have been especially useful as previous studies have reported significant associations between pneumonia in the first 1–3 years of life and impairment of adult lung function compared with older children,3 7–9 which might suggest greater pneumonia severity and long-term lung function consequences than for pneumonia occurring in later childhood years.
While this analysis using multiple lung function outcomes is subject to multiple statistical testing, our interpretation has been based on the overall pattern of results rather than on individual p values. Finally, as participants were essentially of European descent and born in 1961, this may limit the generalisability, especially for infants and children who are now immunised against the most common respiratory bacterial pathogens, pneumococcus and Haemophilus influenzae type b.
Conclusions
By exploring comprehensively measured lung function in middle age via a prospective cohort study design, our analyses support an association between parental report of doctor-diagnosed childhood pneumonia and/or pleurisy and mild airflow obstruction in childhood for those who had active asthma as children, but with ‘smaller lungs’ for all participants in middle age. This adds weight to literature which supports early life pneumonia and/or pleurisy as contributing to a predominantly restrictive lung process in later life. Although the lung function deficits are small in magnitude at a population level, the lung function impairment from recurrent episodes in vulnerable populations might be clinically important if combined with other risk factors for worsening lung function in later life.12 39 At the same time, reassurance is appropriate for the vast majority of middle-aged individuals who had doctor-diagnosed pneumonia and/or pleurisy in childhood.
Acknowledgments
We acknowledge the TAHS study participants and previous investigators, Drs Heather Gibson, Bryan Gandevia, Harold Silverstone and Norelle Lickiss. We thank Professors Mark Jenkins and John Hopper (Centre for Epidemiology and Biostatistics, Victoria) and Dr Iain Feather (Gold Coast Hospital, Queensland), who are investigators of TAHS but not coauthors of this manuscript, for their assistance with obtaining funds and data collection. We also acknowledge all the study site coordinators and respiratory scientists who collected data in the lung function laboratories of Tasmania, Victoria, Queensland and New South Wales; the research interviewers and data entry operators; and the organisational roles of Ms Cathryn Wharton and Dr Desiree Mészáros. Furthermore, we thank the late Stephen Morrison (University of Queensland) for his assistance with obtaining funds/data collection, and the late Professor Philip Quanjer from the Global Lung function Initiative for converting the spirometric data and providing expert opinion. Finally we thank the Archives Office of Tasmania for providing data from the 1968 and 1974 TAHS questionnaires and copies of the school medical records.
References
Footnotes
EHW and SCD are joint senior authors.
EHW and SCD contributed equally.
Presented at Part of this work was presented by oral presentation at the regional Thoracic Society of Australia and New Zealand (TSANZ) and thematic poster at the American Thoracic Society Conference, San Diego, 2014.
Funding This study was supported by the National Health and Medical Research Council (NHMRC) of Australia (research grants 299901 and 1021275); the University of Melbourne; Clifford Craig Foundation; the Victorian, Queensland and Tasmanian Asthma Foundations; Royal Hobart Hospital; Helen MacPherson Smith Trust; GlaxoSmithKline; and John L Hopper. JLP, CL, AL, EHW and SD are funded through the NHMRC of Australia. JLP was also in part supported by Lung Foundation Australia (LFA). ABC is funded by an NHMRC Practitioner Fellowship (APP1154302) and Children’s Hospital Foundation (Queensland, grant 50286). The funding agencies had no direct role in the conduct of the study, the collection, management, statistical analysis and interpretation of the data, preparation, or approval of the manuscript.
Competing interests CFM has directed speaker fees to her institution from Menarini and AstraZeneca. MJA has received investigator-initiated grants for unrelated research from Pfizer and Boehringer Ingelheim, and an unrelated consultancy from Sanofi. BRT has received speaker fees from Mundipharma Australia and AstraZeneca. ABC has received other fees from GlaxoSmithKline. JLP has received a travel grant from Boehringer Ingelheim.
Patient consent for publication Not required.
Ethics approval This study was approved by separate human ethics review committees at all participating institutions, principally The University of Melbourne (040375) and the University of Tasmania (H0012710). Written informed consent was obtained from all participants.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be obtained from a third party and are not publicly available.