Article Text

Statistics from Altmetric.com
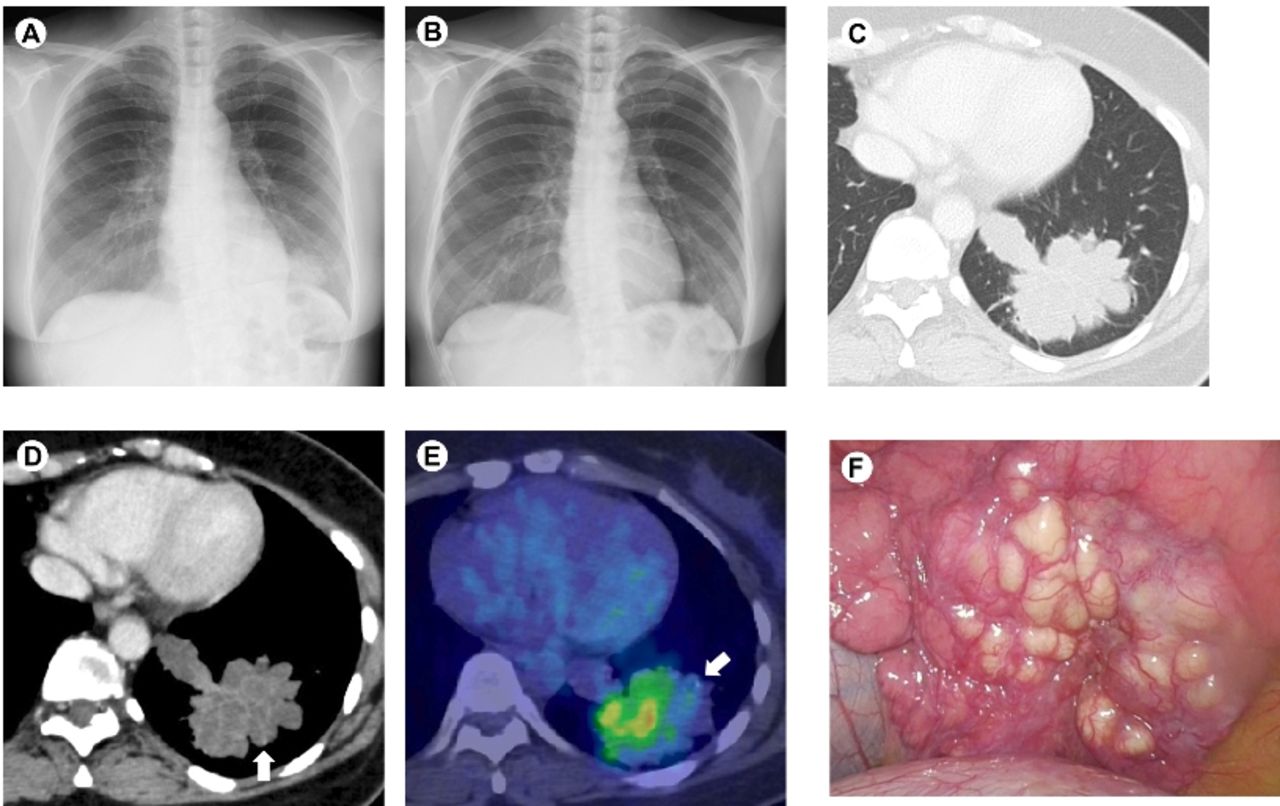
A 43-year-old asymptomatic woman with no history of smoking was referred to our hospital because of decreased radiolucency in the left lower lung field (figure 1A), which was found by chest X-ray performed as part of a routine investigation during a medical check-up. No abnormal shadow was recognised by chest X-ray performed two years previously (figure 1B). Initial laboratory data included a white blood cell count of 4710/μl (neutrophils, 48.6%) and a C-reactive protein level of 0.03 mg/dL. Chest enhanced CT revealed a solitary lobulated low attenuation mass with septal enhancement, approximately 6 cm in diameter, across the left lateral and posterior basal segments (figure 1C-D). The internal structure appeared multilocular and was filled with fluid. A small part of the margin of the mass was accompanied by stippled calcification (figure 1D-E). Bronchoscopic examination was performed on suspicion of pulmonary mucinous cystadenocarcinoma (PMCAC). However, the forceps could not reach the mass. Bronchial lavage bacterial culture, acid-fast bacillus smear (Ziehl-Neelsen stain) and PCR tests for Mycobacterium tuberculosis, Mycobacterium avium and Mycobacterium intracellulare were all negative. The maximum standardized uptake value measured by positron emission tomography of the mass, which showed heterogeneous 18F-fluorodeoxyglucose (FDG) uptake, was 5.2 suggesting a non-benign process (figure 1E). Primary lung cancer without metastasis was diagnosed and the patient agreed to undergo video-assisted thoracoscopic lobectomy. Many rounded pale yellow nodules were observed on the diaphragmatic surface of the left lung (figure 1F). A large amount of pus was discharged from the divided face of the resected mass. Histologically, no neoplastic cells were present in the mass. The bronchial lumens expanded cystically and the insides were full of purulent exudate. Many granulomas with indistinct boundaries were observed around the bronchi and some granulomas were accompanied by small central necrosis (figure 2A-D). Distinct necrotising granulomas were observed in resected lymph nodes (figure 2E). These findings were suggestive of an infectious aetiology including mycobacterial diseases. Later, acid-fast bacillus culture of the pus became positive and the isolate was identified as Mycobacterium kansasii by DNA-DNA hybridisation. Adjunctive antimicrobial therapy with isoniazid, rifampin and ethambutol scheduled for one year was initiated and no evidence of recurrence was detected for eight months after the operation.

Radiological findings (A–E) and intraoperative photography (F). (A) Chest X-ray on admission shows decreased radiolucency in the left lower lung field. (B) Chest X-ray performed two years previously shows no abnormal shadow. (C: CT, D: enhanced CT, E: positron emission tomography/CT) A solitary lobulated low attenuation mass with septal enhancement was observed across the left lateral and posterior basal segments. The internal structure appeared multilocular and filled with fluid. A small part of the margin of the mass was accompanied by stippled calcification (arrows). The mass indicated heterogeneous 18F-fluorodeoxyglucose uptake. (F) Many rounded pale yellow nodules on the diaphragmatic surface of the left lung.

{kind=link}
{kind=link}
Histology of a resected specimen (A-D: mass, E: lymph node, A: loupe image, B: low-power field, C-D: high-power field, E: medium-power field). The bronchial lumens expanded cystically and the insides were full of purulent exudate (A–B). Many granulomas with indistinct boundaries were observed around the bronchi (B–D). (D) Granuloma accompanied by small central necrosis. (E) Distinct necrotising granulomas.
Being asymptomatic, the multilocular cystic low attenuation lesion with septal enhancement, peripheral stippled calcifications and heterogeneous FDG uptake observed in the patient were all characteristic findings of PMCAC.1 In addition, various pathophysiologies leading to mucoid impactions, such as allergic bronchopulmonary aspergillosis, bronchogenic carcinoma and carcinoid tumour, were also considered, although the typical ‘finger-in-glove’ sign was not observed.2 However, the contents were not mucus, but pus, and the septae in the mass consisted of walls of cystically dilated bronchi and surrounding granulomatous inflammation. It was not clear whether the M. kansasii infection newly caused bronchiectasis or was secondary to existing bronchiectasis in this case, but the relatively rapid expansion of the lesion within two years suggested that M. kansasii infection was directly involved in bronchodilation. In some patients with pulmonary disease caused by non-tuberculous mycobacteria (NTM), especially in adult non-smoking women, cylindrical bronchiectasis progresses later than nodular lesions. Takahashi et al previously identified bronchiectasis in 27.6% of patients with M. kansasii pulmonary disease.3 However, prominent cystic bronchiectasis due to NTM including M. kansasii infection was not reported. We need to consider that the radiological manifestations of pulmonary NTM diseases are protean and NTM infection should be considered as a differential diagnosis of a solitary lobulated mass.
Footnotes
Contributors Conception and design: NK, TS. Collection and interpretation of data: NK, TS, KN, HH, FO. Drafting of the manuscript: NK, TS. Approval of the final version of the manuscript: NK, TS, KN, HH, FO.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There are no additional unpublished data.
Linked Articles
- Airwaves