Article Text

Abstract
Here, we report that increasing treatment with inhaled corticosteroids (ICS) in patients with not well-controlled asthma from a medium to a high dose results in a profound reduction of blood eosinophils (median fall in blood eosinophil concentrations from 560 to 320 cells/µL). Therefore, ‘normal values’ of blood eosinophils in patients with asthma need to be considered in view of the individual ICS doses of the patients. In addition, increases in the dose of ICS may result in blood eosinophil concentrations which would formally preclude treatment with biologics targeting the interleukin-5 pathway.
- asthma
- eosinophil biology
Statistics from Altmetric.com
To the editor
Although enhanced blood eosinophil concentrations have been recognised as a feature of asthma since the beginning of the 20th century,1 there has been renewed interest in this parameter over the last years.2 Higher blood eosinophil concentrations were found to correlate with asthma severity3 and the occurrence of asthma exacerbations,4 whereas treatment with biologics that lead to a specific reduction of blood eosinophils are associated with a reduction in asthma exacerbations.5 6 Although it is well established that long-term treatment with inhaled corticosteroids (ICS) and even temporary increases of the ICS dose reduce asthma exacerbations,7 8 the impact of ICS treatment on blood eosinophils is still poorly understood.
Currently, decisions for treatment with biologics targeting the interleukin-5 (IL-5) pathway are made on the basis of blood eosinophil concentrations. It is, therefore, of utmost importance to understand the impact of changes in baseline asthma medications, especially ICS, on blood eosinophils. In 1993, Evans and colleagues demonstrated that treatment with a high dose of ICS (1600 µg budesonide per day for 14 days) in 10 patients with mild asthma not previously treated with ICS resulted in a mean fall in blood eosinophil concentrations from 370 to 160 cells/µL (reduction by 57%).9 However, the effect of an increase of the maintenance dose of ICS on blood eosinophils in patients with moderate to severe asthma is unknown.
Here, we report, for the first time, that the recommendation to optimise the dose of ICS prior to an evaluation of treatment with biologics in patients with not well-controlled asthma has a profound influence on blood eosinophils. Eleven consecutive patients (median age 54 years; 5 women, 6 men; 6 never-smokers, 5 ex-smokers) who presented as part of their routine clinical care to the outpatient severe asthma clinic of the department of pneumology (University of Rostock, Germany) with not well-controlled asthma despite long-term treatment with ICS in combination with a long-acting beta-agonist were examined (table 1). All patients had been treated with a stable dose of ICS for at least 6 months prior to their initial consultation at our severe asthma clinic. Of these 11 patients, 7 patients also inhaled a long-acting muscarinic antagonist. None of the patients was taking systemic corticosteroids, other systemic immunosuppressive drugs or biologics.
Lung function und blood eosinophils of each patient before and after the increase in the daily ICS dose
Baseline lung function, blood eosinophil concentrations (cells/µL blood) and blood eosinophil percentages (% of all blood leucocytes) were assessed before the daily dose of ICS was at least doubled (from a median dose of 1000 µg beclometasone equivalent per day to a median dose of 2000 µg beclometasone equivalent per day). The patients were reassessed after a median follow-up period of 84 days (table 1). A decrease in blood eosinophil concentrations was observed in all patients following the increase of the dose of ICS (figure 1), with a median fall in blood eosinophil concentrations from 560 to 320 cells/µL (reduction by 49%) (figure 1) and a median fall in blood eosinophil percentages from 8.7% to 4.8% (reduction by 46%) (table 1).
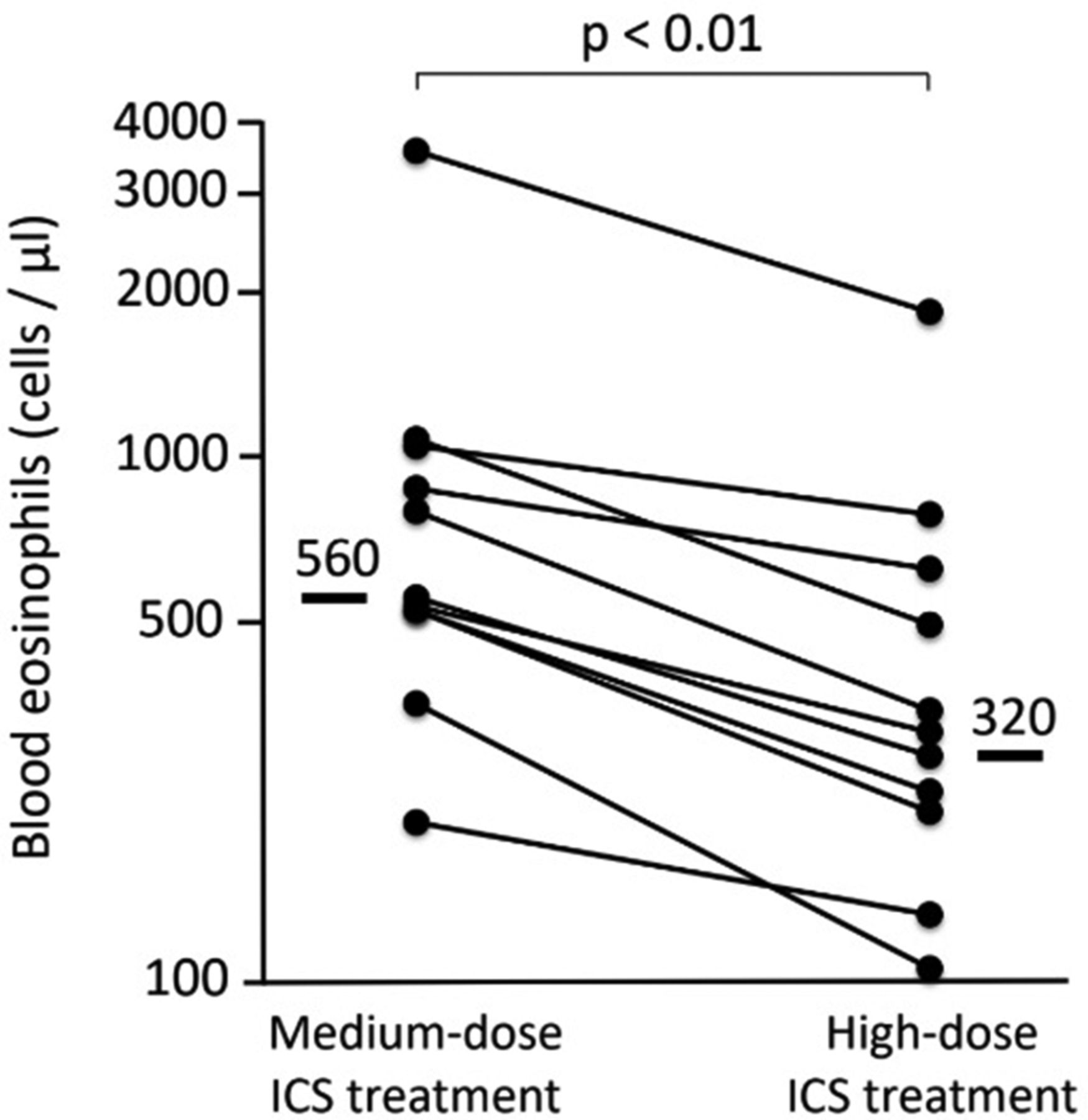
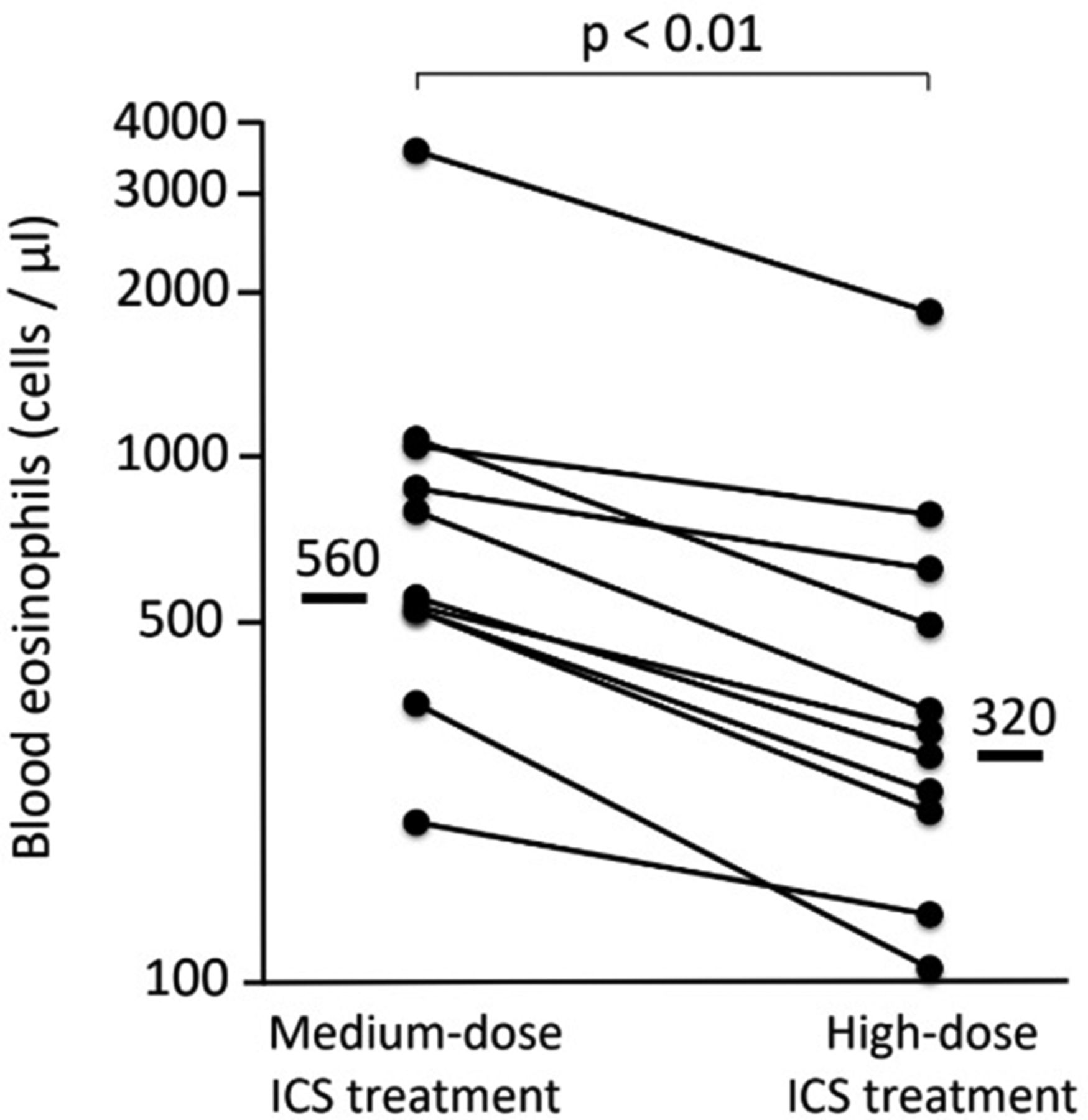{kind=link}
Concentrations of blood eosinophils (cells/µL, logarithmic scale) are shown for each patient (n=11, each dot represents one patient) before (‘medium-dose inhaled corticosteroids (ICS) treatment’) and after (‘high-dose ICS treatment’) the increase of the ICS dose. Median values are shown as bars and numbers. The statistical difference (p value) between the time points was analysed using the Wilcoxon signed-rank test for related samples. Following the increase of the ICS dose, asthma control improved in 10 out of 11 patients, 4 patients achieved complete asthma control.
These data suggest that increasing ICS from a moderate to a high dose results in a profound and consistent reduction of blood eosinophils in asthma (by nearly 50%). It might be conceivable that the observed effect was due to the increase of the ICS dose and due to a better adherence (following the visit of a specialised outpatient service). In either case (increased dose and/or better adherence to ICS inhalation), the effect on eosinophil counts would be due to an increase in the daily dose of ICS. This further strengthens our postulate that ICS have a substantial impact on blood eosinophil concentrations (even when changed from a medium to a high dose). The individual blood eosinophil concentration at baseline was not a criterion for study inclusion (there was no selection of patients with high blood eosinophil levels). Therefore, a regression of eosinophil counts to the mean after the follow-up period was unlikely.
It is well established that systemic corticosteroids and biologics targeting the IL-5 pathway have a strong impact on blood eosinophil concentrations.6 Our observation that also changes in ICS doses profoundly impact on blood eosinophils has two important clinical implications. On one hand, our data support the concept that the dose of ICS in patients with eosinophilic asthma and recurrent exacerbations should be increased to a high dose before considering a treatment with biologics or systemic corticosteroids. On the other hand, our data suggest that the parameter ‘blood eosinophils’ in asthma is influenced substantially by the current dose of ICS of the individual patient. Therefore, ‘normal values’ of blood eosinophil concentrations in asthma4 need to be considered in view of the individual dose of ICS of each patient. In addition, an increase in the dose of ICS can result in blood eosinophil concentrations which are formally too low to meet the thresholds required for biologics targeting the IL-5 pathway, suggesting that blood eosinophils should be monitored prior to any increase in the ICS dose.
Footnotes
Contributors All authors planned and conducted this clinical study. ML, PS: analysed the data. All authors were involved in the writing and correction of the manuscript.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.