Article Text

Statistics from Altmetric.com
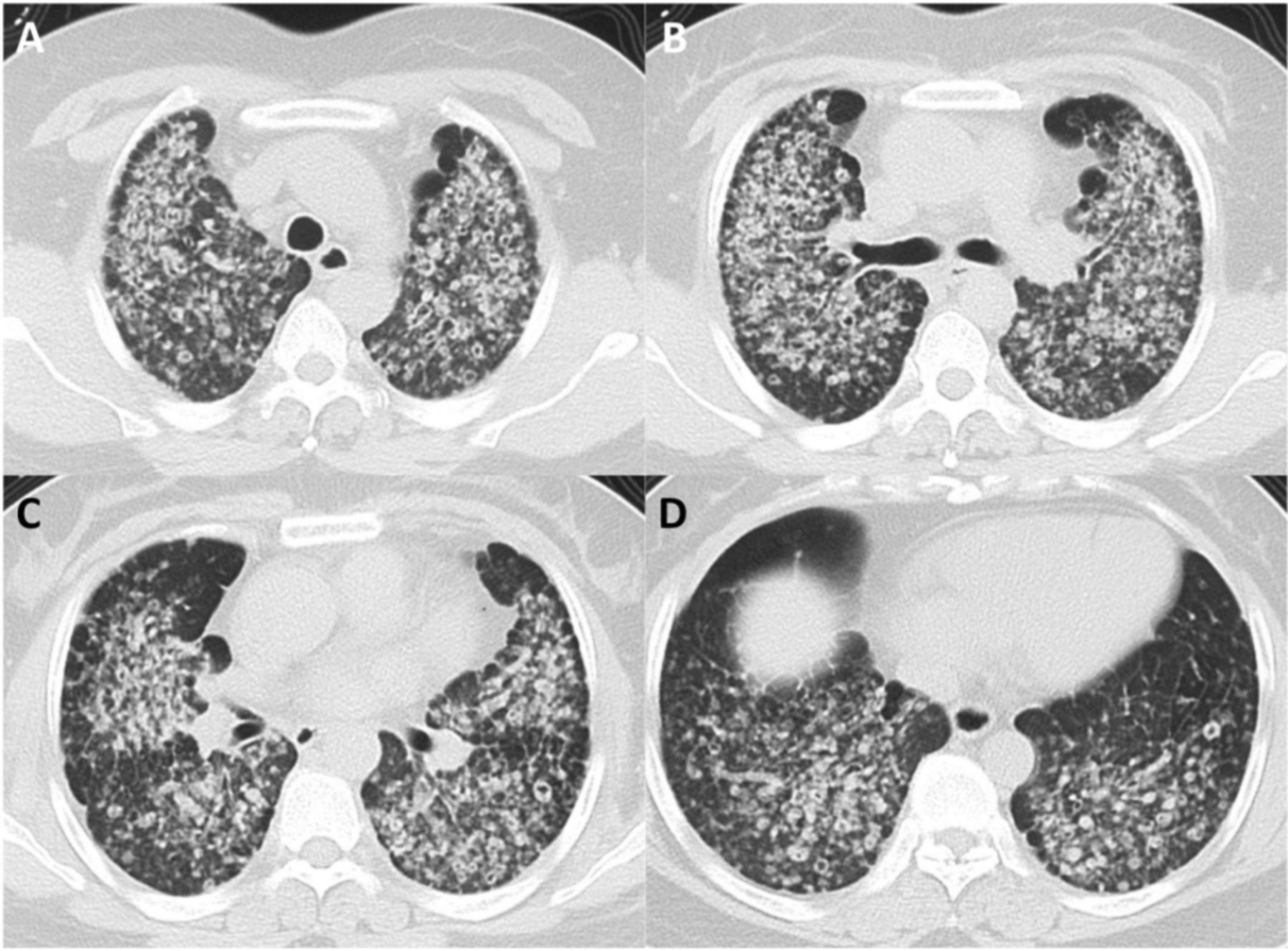
A 49-year-old woman presented to the pulmonary outpatient clinic with a 4-year history of cough and dyspnoea. Physical examination showed bilateral coarse breath sounds. Pulmonary function tests showed mixed ventilatory defects and small airway obstruction. Chest CT (figure 1) revealed diffuse pulmonary nodules smaller than 1 cm with cavitation. Pelvic ultrasonography revealed a uterine leiomyoma measuring 4×3 cm. A video-assisted thoracoscopic surgery wedge biopsy of the left lingular segment was performed. Microscopic examination revealed the nodules were composed of cytologically benign spindle cells without atypia (figure 2A,B). These spindle cells were positive for alpha-smooth muscle actin (figure 2C), oestrogen (figure 2D) and progesterone (figure 2E) receptor, and negative for D2-40, Human Melanoma Black-45 and S-100. In the nodules, there were entrapped tubular and cleft-like spaces lined by epithelial elements of the lung tissue (figure 2B), which were positive for thyroid transcription factor 1 (figure 2F). The clinical and histopathological findings were consistent with benign metastasising leiomyoma from uterine leiomyoma. The patient received 1 year of herbal therapy. Her cough and dyspnoea persisted. Follow-up chest CT and pelvic MRI performed 30 months after the biopsy showed enlargement of the pulmonary nodules and the uterine leiomyoma. Hormonal therapy with tamoxifen was started. The patient was still in follow-up.

(A–D) Chest CT at different levels of the thorax showed diffuse pulmonary nodules ranging from a few millimetres to 1 cm. The majority of the nodules had cavitation.

{kind=link}
{kind=link}
(A) Microphotograph of the biopsy specimen showed tumour nodules (arrowheads) with irregular margins (H&E stain, original magnification ×40). (B) The tumour nodule was composed of benign pink spindle cells with entrapped epithelial elements (arrowheads) of the lung tissue (H&E stain, original magnification ×100). (C–E) The tumour cells were positive for alpha-smooth muscle actin (C, original magnification ×100), oestrogen (D, original magnification ×100) and progesterone receptor (E, original magnification ×100) staining. (F) The entrapped epithelial elements (arrowheads) of lung tissue were positive for thyroid transcription factor 1 staining (original magnification ×100).
Pulmonary benign metastasising leiomyoma is a rare neoplastic process in which leiomyomas of the uterus metastasise to the lung. It usually occurs in women with a history of surgery for benign uterine leiomyoma.1 Radiologically, well-defined solitary or multiple pulmonary nodules ranging in size from a few millimetres to several centimetres are typical findings.1 Rare radiographic findings include cystic lesions, cavitary formation and military pattern.2 3 This case presenting as diffuse cavitary small nodules of the lungs is very unusual. The spindle cell infiltrates of distal airways or alveolar septa may lead to airway narrowing, air trapping and formation of cavity. This case indicates benign metastasising leiomyoma of the lung can present as diffuse micronodularity and macronodularity with some cavitation on CT, which may be mistaken for pulmonary tuberculosis or advanced cystic metastatic carcinoma.3
Footnotes
Patient consent for publication Obtained.
Contributors JZ initiated the idea for case reporting and prepared the final copy of the manuscript. AD took responsibility for reviewing the CT, chest radiograph and MRI. YC supervised and reviewed the final manuscript. YW and JC took responsibility for reviewing the histopathology. All authors have read and approved the final manuscript.
Competing interests None declared.
Ethics approval Ethics Committee of The Second Affiliated Hospital of Jiaxing University.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves