Article Text

Abstract
Background The economic impact of multimorbidity in severe or difficult-to-treat asthma has not been comprehensively investigated.
Aims To estimate the incremental healthcare costs of coexisting chronic conditions (comorbidities) in patients with severe asthma, compared with non-severe asthma and no asthma.
Methods Using health administrative data in British Columbia, Canada (1996–2016), we identified, based on the intensity of drug use and occurrence of exacerbations, individuals who experienced severe asthma in an incident year. We also constructed matched cohorts of individuals without an asthma diagnosis and those who had mild/dormant or moderate asthma (non-severe asthma) throughout their follow-up. Health service use records during follow-up were categorised into 16 major disease categories based on the International Classification of Diseases. Incremental costs (in 2016 Canadian Dollars, CAD$1=US$0.75=₤0.56=€0.68) were estimated as the adjusted difference in healthcare costs between individuals with severe asthma compared with those with non-severe asthma and non-asthma.
Results Relative to no asthma, incremental costs of severe asthma were $2779 per person-year (95% CI 2514 to 3045), with 54% ($1508) being attributed to comorbidities. Relative to non-severe asthma, severe asthma was associated with incremental costs of $1922 per person-year (95% CI 1670 to 2174), with 52% ($1003) being attributed to comorbidities. In both cases, the most costly comorbidity was respiratory conditions other than asthma ($468 (17%) and $451 (23%), respectively).
Conclusions Comorbidities accounted for more than half of the incremental medical costs in patients with severe asthma. This highlights the importance of considering the burden of multimorbidity in evidence-informed decision making for patients with severe asthma.
- asthma epidemiology
- Health Economist
- systemic disease and lungs
Statistics from Altmetric.com
Key messages
What is the key question?
Severe asthma is a costly disease; but do patients with severe asthma also incur higher costs for coexisting chronic conditions (comorbidities) compared with patients with non-severe asthma or with the general non-asthma population?
What is the bottom line?
Severe asthma is associated with incremental healthcare costs of $2779CAD (CAD$1=US$0.75=₤0.56=€0.68) per person-year compared with the general population without asthma and $1922 per person-year compared with the non-severe asthma population; over half of these incremental costs were attributable to comorbidities, particularly to respiratory diseases other than asthma and diseases of the nervous and digestive systems. Costs of mental disorders were similar in severe and non-severe asthma.
Why read on?
This study provides up-to-date estimates of the incremental costs of severe asthma and to the best of our knowledge, is the first that quantifies the impact of multimorbidity across 16 major disease categories towards such costs.
Introduction
Among the roughly 358 million people with asthma worldwide,1 an estimated 1%–3% have the severe form of the disease.2 Severe asthma, or difficult-to-treat asthma, generally refers to asthma which is not responsive to high-intensity treatment with inhaled corticosteroids (ICS) and other controller therapies such as long-acting beta agonists.3 Despite its relatively low prevalence, severe asthma contributes disproportionately to its morbidity, mortality and costs,4 accounting for approximately 50% of the total asthma healthcare costs.5
Compared with mild and moderate asthma, patients with severe asthma might have a higher burden of multimorbidity. In this context, and in line with the definition adopted by the UK Medical Research Council,6 multimorbidity refers to the coexistence of two or more chronic conditions (eg, non-communicable disease, mental condition, infectious disease). For instance, the prevalence of dyspeptic disorders, bone loss, osteoporosis, cataract and chronic kidney disease is reported to be 2–5 times higher in those with severe asthma relative to those without severe asthma.7 Multimorbidity increases the healthcare resource utilisation,8 reduces health-related quality of life9 and results in reduced effectiveness of treatments10 in patients with asthma.
There is evidence from multiple countries including the UK, USA and Canada, on healthcare costs attributed to severe asthma in the general asthma populations.11–13 These figures provide important insights for further research on strategies to reduce the disease burden and important parameters to estimate the cost-effectiveness of health technologies in this patient population. To the best of our knowledge, however, the economic implications of multimorbidity in patients with severe asthma are seldom considered in such analyses. Understanding the systemic healthcare burden of severe asthma and its economic impact can enhance our understanding of this disease and our capacity to assess the merits of investment towards research and care in severe asthma.
Our primary objective in this study was to estimate incremental healthcare costs (hereafter referred to as ‘incremental costs’ for brevity) in individuals with severe asthma as compared with patients with non-severe asthma, as well as with the general non-asthma population. Our secondary objective was to examine the distribution and costs of multimorbidity across 16 major disease categories towards determining the overall incremental costs of severe asthma.
Methods
Data sources
Healthcare resource use data from January 1996 to December 2016 of residents of British Columbia (BC), a Canadian province of 4.4 million (as of 2016, 13% of Canada’s population),14 were obtained through the provincial health administrative databases (covering >98% of legal residents). These databases provide linked, individual-level information on demographics, vital statistics and healthcare encounters of all BC residents15–19 (Details are provided in online appendix 1). Previous analyses have showed a very low prevalence of missing data, under-reporting and misclassification in these databases.20 21 For example, in the current study cohort, only 5% of cost data was missing in the pharmacy dispensation database while the outpatient services database did not have any missing cost data. All inferences, opinions and conclusions drawn in this study are those of the authors and do not reflect the opinions or policies of the Data Steward(s). Ethics approval was obtained from the University of British Columbia Human Ethics Board (H17-00938).
Supplemental material
Study design and sample
This was a retrospective matched cohort study. First, we identified individuals who satisfied a validated case definition of asthma (sensitivity=0.632, specificity=0.997).22 According to this algorithm, asthma was defined as the occurrence of one or more asthma-related inpatient admissions or two or more asthma-related outpatient physician visits (on different dates) or three or more filled asthma-related medications (on different dates) during any 12 month period. Asthma-related inpatient and outpatient encounters were defined as those in which asthma was the most responsible diagnosis (International Classification of Diseases codes, ninth edition (ICD-9): 493.xx or tenth revision (ICD-10): J45.xx, J46.xx). For asthma-related medications, we used a prespecified list (see online appendix 2 for the list of medications). For each patient identified, we defined the date of the first asthma diagnosis as the index date, marking the start of follow-up. To study the evolution of multimorbidity costs over time, we included only new patients who had been in the databases for at least 3 years prior to their first asthma diagnosis. To further reduce the risk of including patients with COPD who might have received the same medications as those with severe asthma, we limited our sample to patients aged between 5 and 55 years at the time of asthma diagnosis and excluded patients who incurred any COPD-specific hospitalisation or three or more COPD-specific physician visits in the first 2 years following the index date for asthma (COPD codes: ICD-9: 491.x, 492.x, 493.2x, 496.x; ICD-10: J43.x, J44.x). Once the patients were included, we followed them over time regardless of age.
Of note, although we removed individuals with a COPD diagnosis in the first 2 years after the index date, COPD is considered a legitimate comorbid condition of asthma.23 As such, beyond the first 2 years, we still considered COPD-related healthcare use in cost calculations.
Second, we divided the asthma cohort into two groups according to disease severity: the severe asthma group experienced an incident year of severe asthma (without having asthma before) and the ‘non-severe asthma’ group experienced only mild and/or moderate asthma throughout the study period. Severity was calculated for each complete 12-month interval from the index date based on a validated algorithm,24 defining severe asthma as the use of high doses of ICS in beclomethasone-chlorofluorocarbon equivalent (average daily dose of at least 1000 µg/day) or reliever medications (more than 10 doses of short-acting β2 agonists per week) while still experiencing moderate-to-severe exacerbations (online appendix 3 provides the details of severity classification). Specifically using Canadian administrative health data, this severity algorithm was based on the Canadian Asthma Consensus Guidelines and was validated against well-established indicators of asthma severity such as pulmonary function measurements.25 The definition of severity in the Canadian guideline is concordant with the definition proposed by the joint European Respiratory Society/American Thoracic Society Task Force on severe asthma26 and has been used in multiple peer-reviewed publications.27 28
As the basis for comparison, we created a third group from a random sample of BC residents who did not satisfy the asthma case definition during the same study period (‘no asthma’). We excluded non-asthmatic subjects with less than 3 years of coverage in the database to match a similar inclusion criterion imposed on the asthma groups. For each included subject in this group, we assigned an index date corresponding to the data of a randomly chosen healthcare encounter which occurred after being in the data for 3 years. Similar to the asthma cohorts, we excluded patients with COPD from the non-asthma cohort.
All study participants were followed from the index date to date of death, loss-to-follow-up (ie, end of registration with the healthcare system) or 31 December 2016, whichever came first.
Matching
Using a pragmatic common-referent pair matching approach,29 we first estimated the propensity scores by fitting two separate logistic regression models that predicted the probability of an individual having severe asthma (common referent group) relative to having non-severe asthma or no asthma, adjusted for the index year, age, sex, area of residence (ie, urban versus rural) and neighbourhood household income quintiles (all observed in the index year). Next, we matched each patient with severe asthma to a patient with non-severe asthma and an individual without asthma, with respect to age (±5 years), sex, index year (±2 years) and propensity score (±0.2). The histogram of propensity scores across three matched cohorts is provided in online appendix figure 1. The remaining imbalances in these covariates across the three groups, as well as pre-existing comorbidity status in the 12 month prior to the diagnosis of asthma (Charlson comorbidity index, number of hospitalisations, physician visits and dispensations of medications), were additionally adjusted for in the regression analysis model.
Outcome variables
The primary outcome was incremental costs of severe asthma, defined as the difference in mean total healthcare costs between severe asthma and non-asthma and between severe and non-severe asthma groups. A secondary outcome was condition-attributable incremental costs, defined as additional costs that were attributable to either asthma or identifiable comorbid conditions. Of note, in line with the definition set forth by the UK Medical Research Council,6 comorbidity was defined as the coexisting condition, rather than the secondary diagnosis of asthma. All costs were adjusted to 2016 Canadian dollars using historical inflation rates from the Consumer Price Index of BC,30 in which CAD$1=US$0.75=₤0.56=€0.68.31 Total costs were summed from three components: hospitalisations, outpatient services and filled prescriptions. We used case mix methodology to calculate hospitalisation costs, which involved multiplying the resource intensity weight for each inpatient admission with the average costs of hospitalisation in BC for the same fiscal year, as described previously.32 Costs of outpatient services and prescription medications were directly available in the data. Of note, most emergency department encounters (78%) were already captured by fee-for-service payments to healthcare practitioners within the outpatient encounter database (eg, billing codes with emergency visits/consultation and 1-day onsite hospital visits), and the rest were captured within hospitalisation costs.33
Based on the most responsible diagnosis code recorded on the billing claim of each healthcare encounter, we separated multimorbidity-attributable costs to either asthma or to one of the 16 major disease categories of comorbidities. These categories were defined according to the highest level classification (the first letter) in the ICD-10 codes. As for the healthcare encounters that were associated with the presence of symptoms (ICD-10 code range R00-R69), we assigned their costs to the corresponding ICD-10 comorbid areas based on the Diagnosis-Related Groups (part of the ICD system). ICD-9 codes, being used in the entire outpatient databases and up to 2002 in the inpatient databases, were converted to ICD-10 codes using validated cross-walk algorithm.34 Medication records were assigned into corresponding comorbidity categories by mapping the American Hospital Formulary Service (AHFS) major categories (available in the data) to ICD-10 categories35 (online appendix 4). Inpatient, outpatient or medication records that could not be assigned to any multimorbidity category (eg, injury, poisoning, burns and other external causes, lab tests, miscellaneous drugs) or when they had undefined ICD or AHFS codes, were grouped into an ‘unattributable costs’ category.
Statistical analysis
The unit of observation was each 12 month period following the index date. To avoid biased estimates of incremental costs due to temporary absence of individuals from the Province, periods with fewer than 300 days of registration were removed unless death occurred within the period.
Descriptive analyses were performed on the distribution of matching variables and additional selected confounders at baseline and the prevalence of comorbidity diagnoses during follow-up period across study cohorts. In the adjusted analyses, we used generalised linear models to estimate the differences in healthcare costs between patients with severe asthma versus non-asthma matches and between severe asthma versus non-severe asthma patients. The exposure variable was the cohort membership (no asthma, non-severe asthma, severe asthma). Estimates were reported as averaged incremental costs per person-year. To account for the potential residual imbalances in matching, we further adjusted the model for age, sex, rural residence and neighbourhood household income, all measured at the index year. To control for the effect of pre-existing conditions (prior to asthma incidence), we further adjusted for the number of all-cause hospitalisations, physician visits, medication dispensations and Charlson Comorbidity Index, all observed in the 12 months before the index date. Normal distribution and identity link were used in the estimation. The assumption of the normality of the mean is justified in this context given its robustness with large sample sizes,36 and was used in previous asthma cost studies.37 38 Generalised estimating equations, with an independent working correlation matrix and a robust sandwich estimator, were applied to obtain robust inference for the clustered time series data (given the clustering of observation units within individuals). Separate regression analyses were performed for the all-cause and condition-attributable costs and by cost components. All analyses were performed using SAS 9.3 (SAS Institute, Cary, North Carolina, USA).
Results
Figure 1 displays the flowchart of cohort creation. We initially identified a total of 6620 individuals between 14 and 55 years of age with incident severe asthma, 247 401 with non-severe asthma and 939 280 with no asthma. After matching, the final sample included 6402 individuals within each group. Table 1 presents baseline characteristics of the sample. Within each group, the average age was 37.4 years (SD=13.6) and 54% were women. Both severe and non-severe asthma cohorts had more people living in rural areas compared with the non-asthma cohort (22%, 19% and 11%, respectively). Additionally, patients with severe asthma had a relatively higher comorbidity burden before the index date compared with those with non-severe asthma or without asthma (Charlson Comorbidity Index, 0.30, 0.18 and 0.02, respectively). Imbalance in the baseline distribution of these variables was adjusted for in cost estimations.

Flowchart of cohort creation.
Baseline characteristics of the study cohorts
All-Cause incremental costs, overall and by components
Figure 2 presents adjusted incremental healthcare costs during follow-up. Online appendix table 1 provides further details including numerical values, 95% CI and results by cost components.
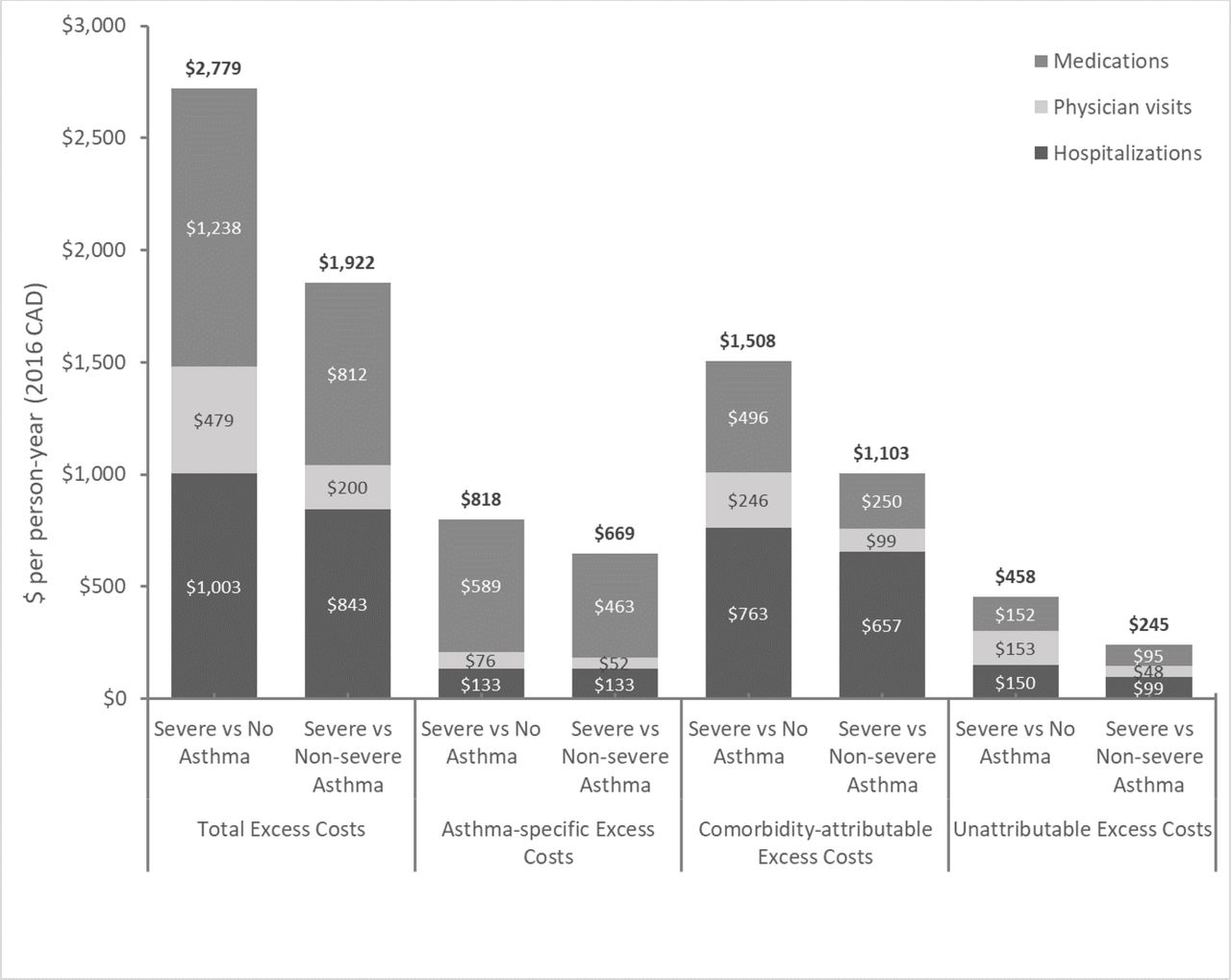
Overall incremental costs per person-year in patients with severe asthma. CAD$1=US$0.75=₤0.56=€0.68.
Relative to individuals without asthma, severe asthma patients incurred approximately three times higher annual healthcare costs ($4125 vs $1345), corresponding to incremental costs of $2779 per person-year (95% CI 2514 to 3045). Asthma-specific costs accounted for $818 (95% CI 763 to 873), corresponding to 29% of incremental costs, while the comorbidity-attributable costs accounted for $1508 (95% CI 1303 to 1714) or 54% of incremental costs; the remaining 16% ($458) could not be attributed to any specific diseases.
On the other hand, compared with patients with non-severe asthma, patients with severe asthma generated twice higher annual healthcare costs ($4125 vs $2202), corresponding to incremental costs of $1922 (95% CI 1670 to 2174) per person-year. Approximately 35% ($669 (95% CI 615 to 723)) and 52% ($1003 (95% CI 800 to 1205)) of the incremental costs were attributable to asthma and comorbidities, respectively, with the remaining 13% ($245) classified as unattributable costs.
Hospitalisations for comorbidities, medications for asthma and medication for comorbidities were the three largest components in the incremental costs of severe asthma, both relative to no asthma ($763 (27% of mean total incremental costs), $589 (21%), $496 (18%), respectively) and to non-severe asthma ($657 (34%), $463 (24%), $250 (13%), respectively).
Condition-attributable incremental costs and prevalence of comorbidities
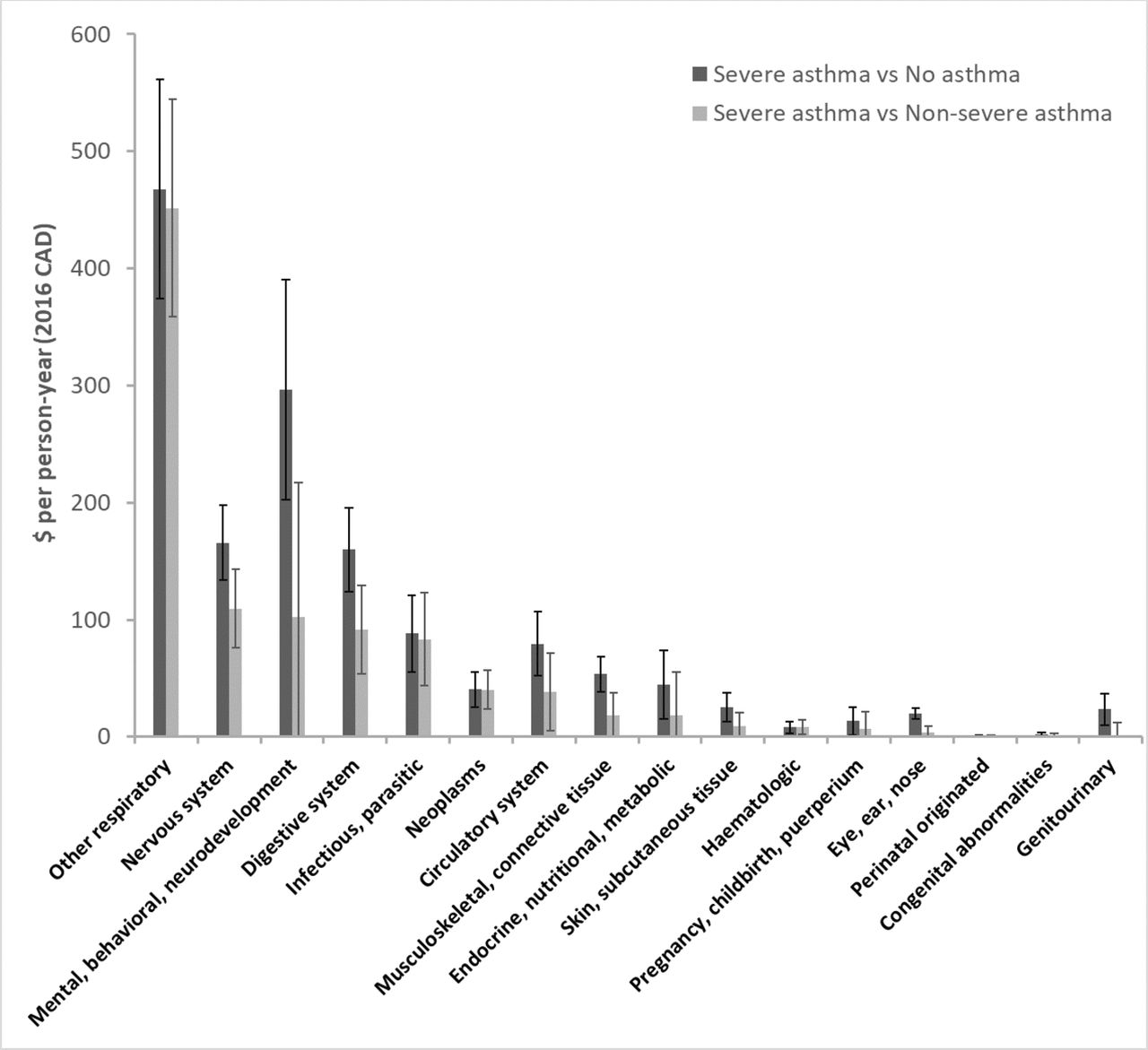
Online appendix table 3 presents the prevalence of comorbidity-related healthcare use across three study cohorts during the follow-up period. Figure 3 displays comorbidity-attributable incremental costs of severe asthma. Online appendix table 2 presents the numerical values and 95% CIs.

{kind=link}
{kind=link}
{kind=link}
Comorbidity-attributable incremental costs per person-year in patients with severe asthma. CAD$1=US$0.75=₤0.56=€0.68.
Compared with individuals without asthma, patients with severe asthma incurred significant incremental costs for comorbidities across most disease categories. The highest incremental costs were found in other respiratory conditions ($468, 17% of mean total costs), mental/behavioural disorders ($296, 11%) and diseases of the nervous ($166, 6%) and digestive ($160, 6%) systems (figure 3). These conditions were much more frequently diagnosed in severe asthma compared with no asthma (respiratory: 88% vs 49%, mental: 63% vs 29%, nervous system: 51% vs 31%, digestive: 53% vs 31%, online supplementary file 1).
Compared with patients with non-severe asthma, patients with severe asthma incurred highest incremental costs for other respiratory conditions ($451, 23%), diseases of the nervous system ($110, 6%), diseases of the digestive system ($92, 5%) and infectious and parasitic diseases ($83, 4%). Nonetheless, these conditions were only slightly more prevalent in severe asthma compared with non-severe asthma, suggesting greater disease severity (respiratory: 88% vs 79%, nervous system: 51% vs 49%, digestive: 53% vs 48%, infectious:50% vs 44%, online appendix table 3).
Of note, the costs of other respiratory diseases, infectious diseases and neoplasms did not significantly differ between patients with non-severe asthma and those without asthma (online appendix table 2).
Discussion
This study identified 6402 patients whose healthcare resource uses in the first year of asthma diagnosis were compatible with severe asthma, comprising 1% of the asthma population in British Columbia. On average, patients with severe asthma incurred incremental healthcare costs of $2779 per year compared with non-asthma controls and $1922 per year compared with patients with non-severe asthma. Importantly, roughly 1/3rd of the incremental costs were attributable to asthma itself whereas over 50% were attributable to comorbidities, a share mainly driven by comorbidity-related hospitalisations. Compared with both non-asthma controls and patients with non-severe asthma, patients with severe asthma incurred the highest comorbidity-attributable incremental costs for respiratory diseases other than asthma, diseases of the nervous system and diseases of the digestive system. While patients with severe asthma also incurred very high incremental costs of mental disorders compared with non-asthma individuals, such costs did not significantly differ from patients with non-severe asthma. Overall, the findings of this study can provide insights into the scale of overall burden of severe asthma (incremental costs roughly 3 times of asthma-attributable costs), the share of comorbidity-attributable incremental costs (1.5–2 times of asthma-attributable costs) and comorbid conditions that are the most costly.
These results were generally consistent with the findings of Voorham and colleagues, who in an asthma cohort with a comparable sample size from the UK general practice, which showed a 1.5–2.5-fold increase in the costs from pneumonia, peptic ulcer, cardiovascular diseases and other comorbidities in ‘severe asthmatics’ who received systemic corticosteroids compared with patients with asthma who were not treated systemic corticosteroids.39 We extend the findings of this UK study, which evaluated only a selected number of discrete comorbid conditions, by performing analyses on all major comorbid conditions and their associated costs across all disease categories. While estimating asthma-attributable costs was not an objective of our study, these costs could be calculated from our analyses to be compared with previously reported values. Our estimates of annual asthma-attributable costs in severe asthma ($818) were lower than the analogous costs in the recent UK11 and US40 studies (£861/$1538 and US$3030/$2273); however, those studies were focused on the most severe and uncontrolled cases with high eosinophil counts; also, more expensive healthcare systems such as that of the US tend to generate higher costs. Interestingly, the costly comorbidities in severe asthma were generally the same as those identified in our previous study in the general asthma population.41 Our previous work found significantly elevated comorbidity costs across nearly all disease categories in patients with asthma compared with the general non-asthma population.41 The present study further shows that most costly comorbidities in asthma are predominantly driven by a subset of patients with severe asthma, whereas non-severe patients do not significantly differ from the general population on the costs of such comorbidities.
One aspect for the high burden of comorbidity in severe asthma is the elevated prevalence of comorbid conditions. Systemic inflammation, more prevalent in severe asthma compared with non-severe asthma,42 43 can result in several other comorbid conditions related to chronic inflammation.44 45 Also, it has been noted that severe asthma often predisposes patients to fixed airflow obstruction, possibly through airway remodelling.46 In addition to higher prevalence for some conditions, our findings suggest that several comorbidities may be more severe in severe asthma than non-severe asthma, such as diseases of the nervous system which was almost equally prevalent in patients with severe and non-severe asthma. On the other hand, comorbidities may contribute to the burden of severe asthma. For instance, rhinosinusitis and viral infection can either worsen asthma symptoms44 or trigger exacerbations.45 Multimorbidity medications are found to be associated with a poor asthma prognosis.47 Finally, the burden of being diagnosed with a lifelong condition can be responsible for the high burden of mental health. Of note, and consistent with earlier findings,48 we found that the high costs of mental disorders in patients with asthma did not differ substantially between severe and non-severe asthma.
This study has some limitations. Our definition of asthma severity was based on a validated algorithm specifically constructed for health administrative data24; however, in the absence of objective measures of lung function and symptoms, such an algorithm can only approximate the clinical definition. For example, it is possible to misclassify patients into severe asthma when they were non-severe but filled more prescriptions than needed. This is relevant because administrative data only capture information on prescription dispensations rather than actual consumption. However, such a misclassification risk is mitigated because severity classification was also based on markers of exacerbation. Second, the definition of severe asthma guaranteed higher asthma-attributable costs in the first year of follow-up compared with the other groups, but this did not apply to subsequent years and not to comorbidity costs which were the primary focus of this work. On the other hand, misclassification can also occur when disease-attributable costs are concerned, because diagnostic codes might not be always correctly assigned. In addition, mapping prescription drugs to disease categories demands certain degree of subjectivity. Fourth, potential confounders such as smoking and physical activity were not recorded in health administrative data. Last but not least, these results did not provide information about the proportion of variance in costs that was explained by severe asthma and different comorbidities. This was difficult due to the complex interactions between diseases, between disease and treatment and between treatments.
In conclusion, over half of the difference in all-cause healthcare costs between severe and non-severe asthma is due to comorbidities, with one-third specifically due to comorbidity-related hospitalisations. Interestingly, while the incremental costs are lower, the similar ratios apply when severe asthma is compared with non-asthma. The presence of multimorbidity leads to a complex interplay between diseases and treatments.6 Our findings provide direct evidence to support the importance of considering comorbidity costs to the cost-effectiveness evaluation of interventions for severe asthma. Beyond health economics, these findings suggest the importance of taking a holistic approach towards managing patients with severe asthma.
References
Footnotes
Contributors WC and AS had full access to all of the data in the study and took responsibility for the content of the manuscript, including the integrity of the data and the accuracy of the data analysis. WC, AS, JMF and MS conceived and designed the study. AS and HT prepared the data. AS and WC analysed the data. WC wrote the first draft of the manuscript. WC, AS, JMF, DS, HT and MS contributed to the interpretation of the data. JMF and DS contributed to the clinical inputs. All authors were involved in the revision of the manuscript for important intellectual content and approved the final version to be published.
Funding This study was funded by The Legacy Program – Vancouver Coastal Health Research Institute.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be obtained from a third party and are not publicly available.
Linked Articles
- Airwaves