Article Text

Statistics from Altmetric.com
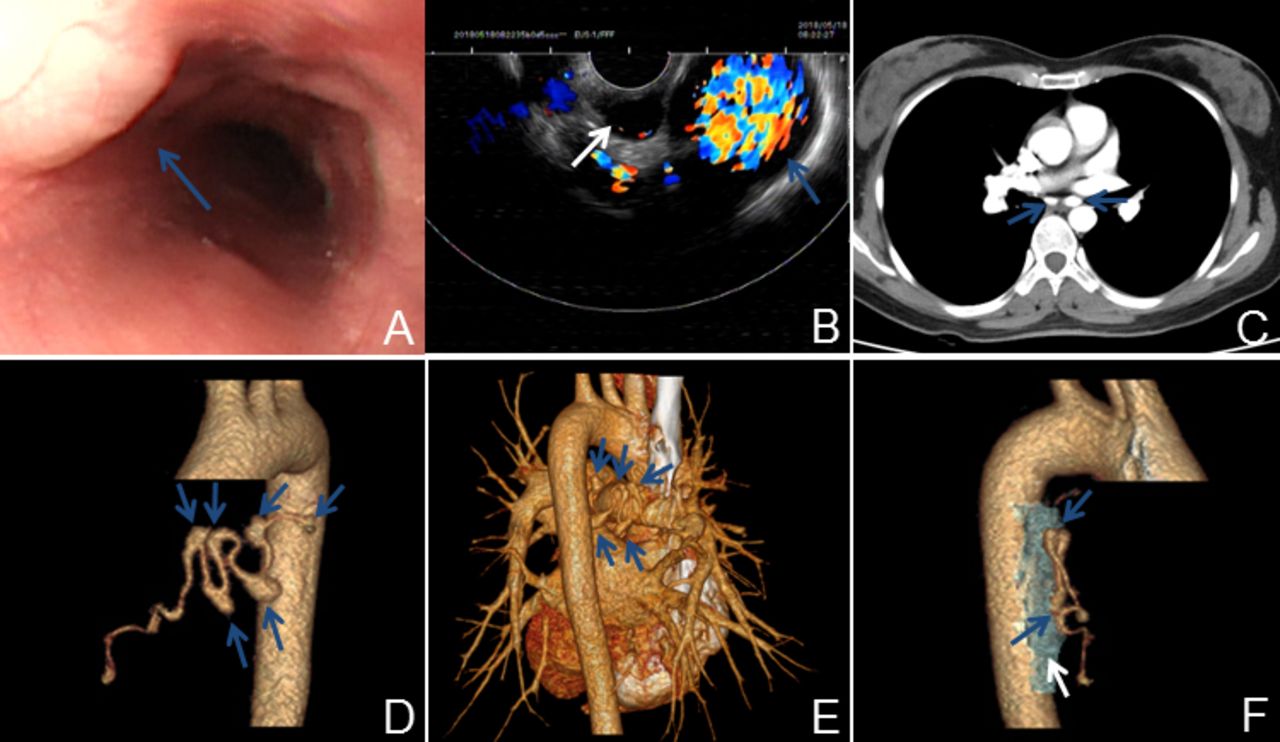
A 41-year-old woman attended hospital with a 2-week history of a post-prandial, left upper abdominal pain. The patient underwent upper gastrointestinal endoscopy, and multiple round oesophageal submucosal lesions (figure 1A) were observed. On ultrasound, these abnormalities were echoless and were identified as outside the oesophageal wall with blood flow detected by colour Doppler flow imaging. Moreover, one of the lesions was connected to the aorta (figure 1B). There were no other abnormalities reported by the patient in terms of medical history and, in particular, there was no history of genetic disease. The rest of the physical examination and laboratory tests did not reveal any clinical anomalies, although the patient reported a 10-day history of cough and dysphagia 2 months previously, at which time a chest CT scan showed no obvious cause.

(A) Upper gastrointestinal endoscopy showing multiple round lesions of oesophageal submucosa lesions (blue arrow). (B) These lesions were echoless with blood flow outside the oesophageal wall (white arrow) by ultrasound and colour Doppler flow imaging; moreover, one of the lesions was connected to the aorta (blue arrow). (C) Contrast-enhanced chest CT scan showing BAAs (blue arrows), which exhibited a similar degree of contrast enhancement with the aorta in the arterial phase and compressed the adjacent oesophagus. (D,E) Three-dimensional volume rendering image clearly showing at least five BAAs and aneurysmal dilations in the right bronchial artery (blue arrows). (F) 3D fusion image of the oesophagus (white arrow) compressed by multiple BAAs (blue arrows). BAA, bronchial artery aneurysm.
A contrast-enhanced chest CT scan and three-dimensional volume rendering image showed at least five aneurysms and aneurysmal dilations with varying sizes in the right bronchial artery (figure 1C–E); some of the aneurysms compressed the adjacent oesophagus (figure 1C, F).
Selective bronchial arteriography confirmed the CT findings and revealed multiple aneurysms and aneurysmal dilations in the right bronchial artery (figure 2A). Transcatheter arterial embolization with Embosphere micropheres [Merit Medical (Beijing) Co.,Ltd., China] and Glubran (GEM S.R.L., Italy) was conducted to occlude the blood flow to the right bronchial artery (figure 2B), which was successful and resulted in no complications. The patient was discharged after 2 days of hospitalisation. After a 10-month follow-up, her condition remained stable, and there were no complications or symptoms in the chest or abdomen.

{kind=link}
{kind=link}
(A) Selective bronchial angiograph confirmed multiple BAAs and aneurysmal dilations (blue arrows) in the right bronchial artery. (B) After transcatheter arterial embolization, the BAAs and aneurysmal dilations were completely occluded. The black area at the edge of the bronchial artery is motion artefacts (white arrow).
Bronchial artery aneurysm (BAA) is a rare but potentially life-threatening vascular abnormality, with an incidence of less than 1%, based on selective bronchial angiography1 ; the incidence of multiple BAAs is even rarer. The aetiology of BAA has not been established and can be congenital or acquired. It has been reported that BAAs are mostly associated with bronchiectasis, atherosclerosis, inflammatory lung disease, hypertension, chronic obstructive pulmonary disease, vasculitis, tuberculosis and trauma.2 3 However, many cases of BAAs have no definite cause.
BAAs can be classified as mediastinal, intrapulmonary or both.1 Patients with BAAs are often asymptomatic, and BAAs are incidentally found during CT angiography. Haemoptysis is the most frequent symptom of intrapulmonary BAAs, while mediastinal BAAs may present with dysphagia, related to the extrinsic compression or rupture into contiguous structures, and BAA rupture is unpredictable and unrelated to the BAA diameter.1 3 Therefore, treatment of every BAA should be initiated as soon as the diagnosis is made. Transcatheter arterial embolization is considered the gold standard of treatment in haemodynamically stable patients because of its safety, selectivity, efficacy and low invasiveness. Surgery should be considered in patients with contraindications to endovascular treatment. In our case, transcatheter arterial embolization was employed to totally occlude the aneurysms and tortuous bronchial arteries.
Footnotes
Contributors C-CL and WC conceived the idea for the article. C-CL drafted the manuscript. WC approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.