Article Text

Statistics from Altmetric.com
TL (junior doctor), RW (respiratory specialist trainee) and SM (respiratory consultant)
A 69-year-old man was initially referred to urology outpatient clinic for investigation of frank haematuria. His medical history included transurethral resection of prostate in 2008, autoimmune hepatitis, hyperlipidaemia and hypertension. He was an active smoker with a 52 pack-year history and drinks 12 units of alcohol per week. He worked as a librarian with no history of chemical or asbestos exposure. His regular prescription included azathioprine and ursodeoxycholic acid, amlodipine, alfuzosin and finasteride. He underwent a cystoscopy which was normal. Subsequently, a CT urogram was performed which demonstrated a 48 mm mass within the left adrenal gland, suspected of malignancy; however, no primary site had been identified. A subsequent CT of the thorax and abdomen displayed a 6.5 cm diameter mass within the base of the right upper lobe on the background of emphysema, with precarinal and right hilar lymph nodes, and multiple nodules in the middle lobe and left lower lobe (figure 1A). A large left adrenal mass was again identified. On further questioning, the patient described symptoms of breathlessness and lethargy but denied any chest pain or cough. There was no history of sputum production or haemoptysis. He did, however, report loss of appetite and had lost 3 kg of weight over the previous 4 weeks.
{kind=link}
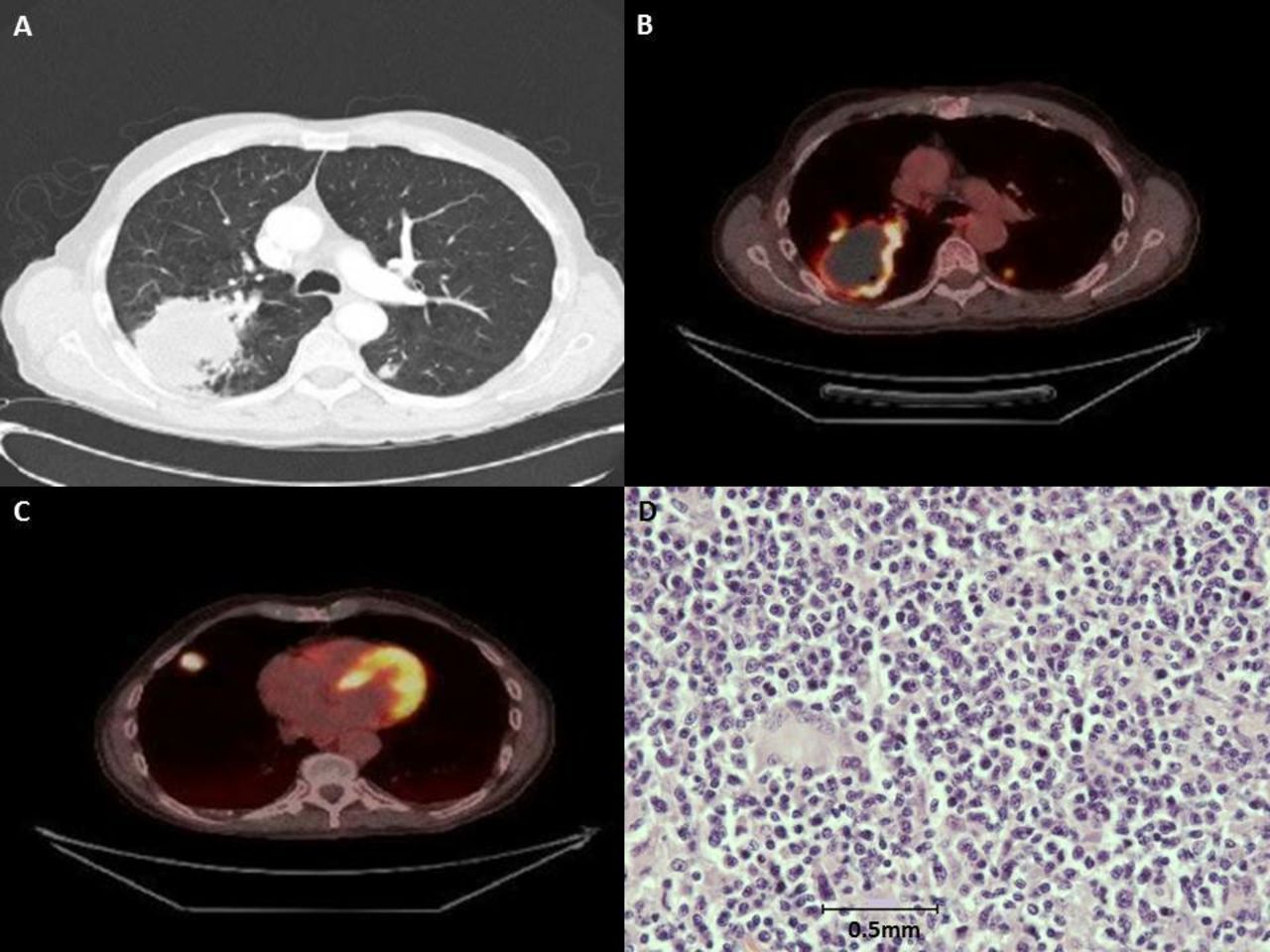
(A) Initial CT thorax demonstrating a 6.5 cm diameter mass within the base of the right upper lobe, small precarinal and right hilar nodes and evidence of multiple intrapulmonary nodules; (B) PET CT demonstrating large necrotic mass at right upper lobe; (C) FDG avid intrapulmonary metastasis; (D) histopathological features of lymphomatoid granulomatosis under high power microscopy (40× objective, NIKON eclipse 80i).
SM and JH (consultant chest radiologist)
With the symptoms of breathlessness and unintentional weight loss, in combination with a significant smoking history and suspicious radiological findings, metastatic bronchogenic carcinoma with a left adrenal metastasis was the most likely diagnosis. Spirometry was performed and demonstrated forced expiratory volume in one second (FEV1) of 2.44 L (85% predicted), forced vital capacity (FVC) of 5.07 L (137% predicted) with FEV1/FVC ratio of 48% and carbon monoxide transfer coefficient (KCO) of 50.6%, indicative of obstructive airway disease with decreased diffusion capacity, most likely secondary to chronic smoking.
A CT-guided biopsy of lung lesion was performed as the next step to establish histological diagnosis, which demonstrated necrotic tissues only. A subsequent endobronchial ultrasound-guided transbronchial needle aspiration of lymph nodes showed granulomatous inflammation with small foci of caseous necrosis. An alcohol and acid-fast bacilli culture from sputum sample was also performed to rule out possibility of mycobacterium tuberculosis infection and this was negative. Due to the ongoing suspicion of cancer, a Positron Emission Tomography (PET) CT scan was performed to evaluate other sites of metastatic disease from which further biopsies may be obtained. This demonstrated a metabolically active necrotic right upper lobe mass with further intrapulmonary metastases (figure 1B and C). Bilateral adrenal metastases were identified. Furthermore, there was a 2 cm lesion in the right supraclavicular fossa and multiple ill-defined subcutaneous lesions. An endoscopic ultrasound-guided biopsy of the adrenal lesions was performed, and this demonstrated no evidence of malignancy. The fine needle aspiration (FNA) and core biopsy of the supraclavicular lesion also demonstrated granulomatous inflammation with no malignant cells seen. To pursue further histological evidence, an FNA of the subcutaneous lesions was performed. This revealed scanty inflammatory cells and was non-diagnostic.
Although all histological findings had been inconclusive at this stage, the most important differential diagnosis remained to be bronchogenic carcinoma and was provisionally staged as T4N3M1b based on radiological findings. Given the patient had a WHO performance status of one and the pulmonary function test was satisfactory, a wedge resection of the upper lobe mass by video-assisted thoracoscopic surgery was performed.
During the follow-up clinic postsurgery, a repeat CT scan of thorax showed regression of the lung lesions. The patient was asymptomatic and his symptoms of weight loss had been resolved. Connective tissue disease screening, rheumatoid factors, total IgE, hepatitis screening, HIV serology and serum Epstein-Barr Virus (EBV) PCR were performed and these were negative.
LP and RT (consultant pathologists)
The initial analysis of the wedge resection showed only granulomatous inflammation (figure 1D). Extended histological analysis was carried out at a specialist centre, and the tissue sample was identified as lymphomatoid granulomatosis (LYG), though EBV was not identified in the samples analysed.
LYG is a rare lymphoproliferative disorder, often associated with the EBV. It is an angio-destructive disease that almost always affects the lungs1 and manifests respiratory symptoms at presentation in most patients, but a minority of patients could be asymptomatic.2 Constitutional symptoms such as fatigue, weight loss and fever are common.2 Extra pulmonary sites of invasion have also been recognised including the skin, however, adrenal metastasis and lymph nodes involvement are relatively rare.1 2
Diagnosis of LYG is often perplexing due to non-specific radiological findings and subsequent histopathological challenges, as demonstrated in this case. Open-lung biopsy is the diagnostic method of choice as it is most likely to yield positive results, while endobronchial samples are rarely positive.3 The presence of EBV, although not mandatory, supports the diagnosis of LYG, therefore efforts were made to analyse multiple samples. It has been suggested that grade I LYG (no large atypical cells with little necrosis; EBV-positive cells are rare) may signify inadequate sampling and EBV may be demonstrated through other tissue samples from elsewhere within the lesion.1
LYG classically involves a triad of polymorphic infiltrate, angiitis and granulomatosis.4 Histologically, one finds nodular replacement of the lung parenchyma, predominantly with lymphocytes, which may become necrotic.4 Microscopic diagnosis can be challenging given its similarities to high grade non-Hodgkin’s lymphoma. Both the presence of mixed mononuclear infiltrate with large and small lymphocytes (CD20+ and CD3+, respectively) and nodular replacement of parenchyma are necessary for diagnosis.4 Other diseases that could mimic LYG include granulomatous polyangiitis and lymphomas.
Given LYG is a lymphoproliferative disorder; this patient should be referred to haematology team for further management and follow-up.
JH and SM
The radiological features of LYG are non-specific and may mimic bronchogenic carcinoma or lung abscesses. However, other radiological presentations are also possible such as pulmonary cystic lesions, pleural masses or interstitial processes. CT scans often demonstrate multiple bilateral lung nodules with predominant basal and peribronchovascular distribution. This can progress rapidly and cavitate, as we have observed in this case.
IT (haematology consultant) and SM
LYG is a rare disease that has a 2:1 male to female predominance with the median age of 48 years old.2 It is noted that this patient had a medical history of autoimmune hepatitis for which he was on azathioprine. In fact, the prevalence of LYG in those who have pre-existing autoimmune disorder are higher,2 as in those who are immunosuppressed or post-transplant.
To date, it remains uncertain whether LYG represents as a distinct disease entity or a part of spectrum of EBV-associated B-cell lymphoproliferative disease. The WHO classification scheme classifies LYG as B-cell proliferation of uncertain malignant potential. The treatment of LYG and prognosis is largely depending on the grade of disease, which are determined by the type and number of EBV-encoded small RNA (EBER)-positive atypical large B-cells and the degree of necrosis found in biopsies. The three tiers grading system are currently in use5
Grade I
No large atypical cells with little necrosis; only a few or absent in EBER-positive atypical large B-cells (<5 per high-power field (hpf)); usually follows an indolent clinical course.
Grade II
Occasional large atypical cells and moderate necrosis; typically has 5–20 EBER-positive atypical large B-cells per hpf; may have a clinical indolent course.
Grade III
Predominant population of large atypical cells (may be confluent) with extensive necrosis. This is considered equivalent to diffuse large B-cell lymphoma due to its aggressive clinical behaviour and similarities in treatment strategies.
This patient had grade I–II disease and a repeat CT scan demonstrated regression of previous lesions. On reviewing this patient in haematology clinic, he was completely asymptomatic, and weight loss had entirely resolved. After the discussion in haematology multi-disciplinary team (MDT), it was felt that chemotherapy was not indicated at the current stage. However, as low grade LYG has the potential to progress into malignant lymphoma,5 close surveillance by imaging should be performed to monitor disease progression.
SM and JH
This patient presented with incidental findings of multiple nodules on lungs, adrenal glands and the skin that were highly suggestive of primary bronchogenic carcinoma. Although LYG is rare, its prevalence is higher in those who are immunosuppressed and with pre-existing autoimmune diseases. In the context of failure in obtaining histological diagnosis after multiple attempts, LYG or other rare systemic inflammatory diseases should be considered. Although pulmonary involvement is almost always present in LYG, lymph nodes and adrenal involvements, as seen in this case, are relatively rare. These sites of fluorodeoxyglucose-avid lesions on PET CT scan mimicked metastatic bronchogenic carcinoma and this highlights the diagnostic challenges in LYG. In this case, it took 6 months from the initial identification of adrenal mass to the confirmation of the LYG diagnosis, and the case was discussed in six lung cancer MDT meetings. As pulmonary involvement is almost always present in LYG and as it mimics several respiratory diseases, respiratory physicians and chest radiologists should always have low index of suspicion of LYG as the diagnosis in high-risk patients, particularly when histological diagnosis remains unclear after multiple attempts.
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.