Article Text

Statistics from Altmetric.com
A 47-year-old woman with a history of chronic cough presented with dyspnoea. She had no history of smoking, tuberculosis and cardiovascular disease. Physical examination revealed wheezing in both lungs. We started maintenance and reliever therapy for suggested bronchial asthma. However, symptoms did not improve, and she was hospitalised repeatedly. Chest X-ray showed a right-sided aortic arch. In the pulmonary function test, a fixed obstruction pattern was observed, and a bronchodilator response was not seen (figure 1A). On bronchoscopy, functional obstruction with extrinsic compression at the level of the lower trachea was shown (figure 1B,C). Chest CT and CT aortography showed a right-sided aortic arch and a left subclavian artery (LSA) with a Kommerell’s diverticulum. The LSA originated from a left innominate artery, connected with the diverticulum and formed a vascular ring (figure 2A–D) that caused fixed extrinsic compression on the lower trachea.
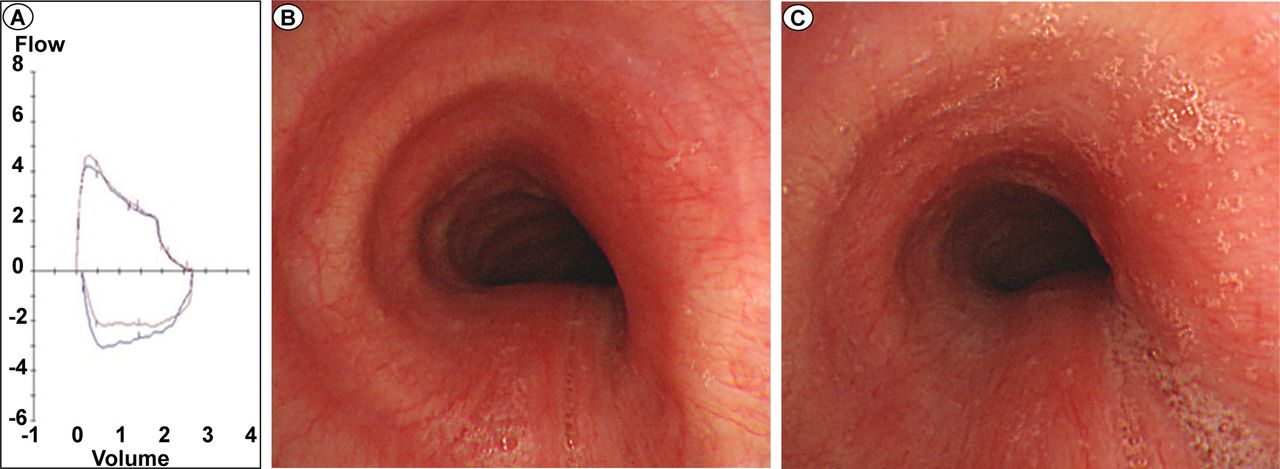
(A) Pulmonary function test shows a fixed obstruction pattern. (B) Functional obstruction on lower trachea during full inspiration on bronchoscopy imaging (60%–70% obstruction). (C) Functional obstruction on lower trachea during full expiration on bronchoscopy imaging (70%–80% obstruction).

{kind=link}
{kind=link}
(A,B) CT scan shows a vascular ring formed by connecting Kommerell’s diverticulum and a left subclavian artery. (C,D) three dimensional reconstruction image by CT aortography shows a left innominate artery from the ascending aorta and connection between Kommerell’s diverticulum and left subclavian artery.
Kommerell’s diverticulum with a right-sided aortic arch is a rare congenital aortic arch abnormality that is mainly found in infancy.1 2 The main symptoms are dysphagia, recurrent airway infection and dyspnoea.3 Sometimes, dyspnoea is accompanied by wheezing, which makes it difficult to differentiate from asthma.4 When the aortic arch appears on the chest X-ray, it is often overlooked. Although not common, clinicians need to consider that dyspnoea can be caused by aortic arch abnormality.
Footnotes
JC and JJS contributed equally.
Contributors Study concept and design: JC and JJS. Acquisition, analysis or interpretation of data, critical revision of the manuscript for important intellectual content and study supervision: all authors. Drafting of the manuscript : JC and JJS.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.