Article Text

Statistics from Altmetric.com
Description
A 24-year-old woman presented with an 8-year history of chest tightness and shortness of breath during intense exercise. Physical examination showed decreased expansion of the right rib cage and respiratory sounds in the right lung were quiet. A routine examination was unremarkable. There were no systemic symptoms, including fever, skin rash and arthralgia. The erythrocyte sedimentation rate and high sensitivity C-reactive protein levels were normal. Autoantibodies, including antinuclear antibodies, antiextractable nuclear antigen antibodies and antineutrophil cytoplasmic antibodies, were negative.
Chest high-resolution CT showed a low right lung volume, markedly thickened interlobular septae (mainly in the right lower lung) and some ground-glass opacity, showing a wedge-shaped area of consolidation (figure 1A). Bronchoscopy showed submucosal varices of the right bronchial tree, with markedly increased surface secretions and mucosal hypertrophy (figure 2). Echocardiography showed normal inner atrial and ventricular diameters. Additionally, ostia of the right superior pulmonary vein were unclear, and pulmonary arterial systolic pressure was normal. CT pulmonary angiography (axial image, figure 1B; coronal maximum intensity projection image, figure 1C) showed a thin right pulmonary artery (PA), with fewer and thinner branches than normal. Right pulmonary venous drainage was not visible. There were multiple, slender, tortuous collateral veins with reflux into the superior vena cava in the right hilum. Selective right PA angiography showed reversed contrast medium flow to the left PA and a decreased diameter of the right PA compared with the left PA (figure 3A). The right pulmonary vein was not visible during the venous phase (figure 3B).

Findings of chest CT and CT angiography. (A) Chest CT shows diffuse thickening of interlobular septae and ground-glass opacity (black arrows) and a small right hemithorax. (B) CT angiography images (axial) showed a smaller right pulmonary artery (black arrows) compared with the left pulmonary artery (white arrow). (C) Coronal maximum intensity projection image shows the left pulmonary artery (bold white arrow) and left pulmonary vein (bold black arrow), while the right pulmonary artery and its branches were slim (thin white arrows) and the right pulmonary vein was absent (thin black arrows).

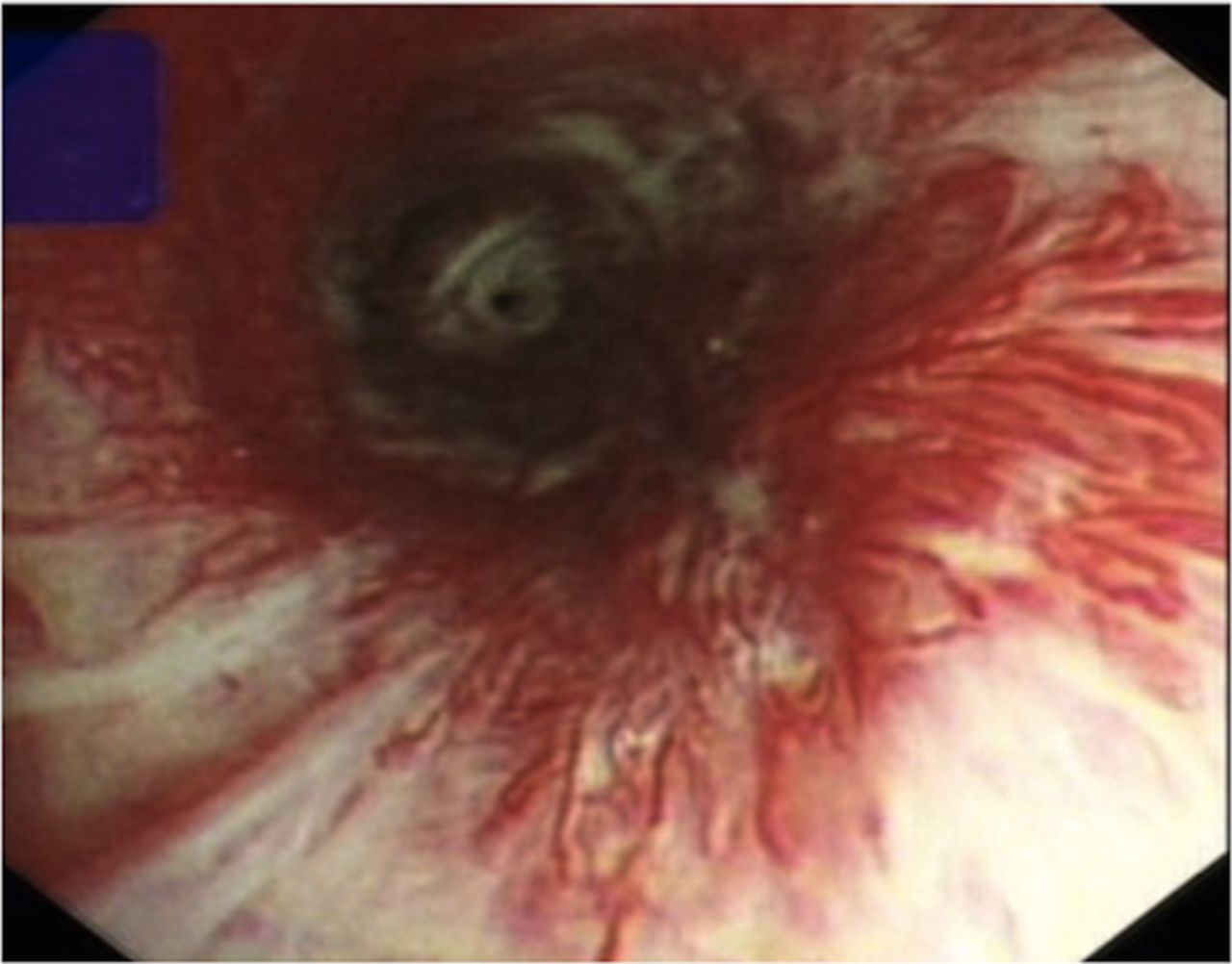
Bronchoscopy shows varices of the right bronchial tree and bronchial mucosal hyperaemia.

{kind=link}
{kind=link}
{kind=link}
Findings of pulmonary angiography. (A) Selective right pulmonary artery angiography shows a thin right pulmonary artery (white arrow) and reversed contrast medium flow to the left side (black arrow). (B) The right pulmonary vein is absent during the pulmonary venous phase (black arrow).
A diagnosis of congenital unilateral pulmonary vein atresia (CUPVA) was made. The patient experienced shortness of breath only after intense exercise and there was no pulmonary infection or recurrent haemoptysis. She was closely monitored, and light-intensity physical activity was permitted.
Unilateral diffuse pulmonary parenchymal lesions are clinically rare. The causes of these lesions include focal chronic inflammatory diseases, such as bronchiectasis and gastro-oesophageal reflux, radiation pneumonitis and mechanical ventilation of a unilateral lung.1 Unilateral diffuse pulmonary parenchymal lesions have also been reported in diseases, such as Sjogren’s syndrome and systemic sclerosis.1 Additional rare causes of unilateral lesions include pulmonary circulatory diseases, such as proximal PA blockage (eg, PA sarcoma), venous thrombosis and unilateral pulmonary vein stenosis due to mediastinal fibrosis. In adult patients with CUPVA, long-term pulmonary circulation abnormalities can cause typical unilateral diffuse lung lesions. However, diffuse thickening of interlobular septae, decreased lung volume and a slender PA on the affected side can differentiate CUPVA from other causes of unilateral diffuse lung disease.
Bronchial varices is a rare bronchoscopic finding, but it is clinically important for establishing the diagnosis of CUPVA.2 Rupture of these dilated bronchial veins can cause mild to massive haemoptysis. Therefore, transbronchial biopsy should be avoided in this situation.
Pulmonary angiography is the gold standard for investigation of CUPVA. CT angiography is also helpful. Magnetic resonance can be useful because it can define anatomic hypoplasia of the right PA and the absence of right pulmonary veins, as well as a lack of any forward flow to the right lung.3
CUPVA should be considered in the differential diagnosis of unilateral diffuse thickening of interlobular septae. The presence of concurrent bronchial varices as visualised by bronchoscopy could strongly suggest diagnosis of this condition.
Footnotes
Contributors HW and JS were involved in designing and drafting of the manuscript. All the authors equally contributed to the collection and interpretation of the data and approval of the final manuscript.
Competing interests None declared.
Patient consent Obtained
Provenance and peer review Not commissioned; externally peer reviewed.