Article Text

Abstract
Background Early-life respiratory tract infections could affect airway obstruction and increase asthma risk in later life. However, results from previous studies are inconsistent.
Objective We examined the associations of early-life respiratory tract infections with lung function and asthma in school-aged children.
Methods This study among 5197 children born between April 2002 and January 2006 was embedded in a population-based prospective cohort study. Information on physician-attended upper and lower respiratory tract infections until age 6 years (categorised into ≤ 3 and >3–6 years) was obtained by annual questionnaires. Spirometry measures and physician-diagnosed asthma were assessed at age 10 years.
Results Upper respiratory tract infections were not associated with adverse respiratory outcomes. Compared with children without lower respiratory tract infections ≤3 years, children with lower respiratory tract infections ≤3 years had a lower FEV1, FVC, FEV1:FVC and forced expiratory flow at 75% of FVC (FEF75) (Z-score (95% CI): ranging from −0.22 (−0.31 to –0.12) to −0.12 (−0.21 to −0.03)) and an increased risk of asthma (OR (95% CI): 1.79 (1.19 to 2.59)). Children with lower respiratory tract infections >3–6 years had an increased risk of asthma (3.53 (2.37 to 5.17)) only. Results were not mediated by antibiotic or paracetamol use and not modified by inhalant allergic sensitisation. Cross-lagged modelling showed that results were not bidirectional and independent of preschool wheezing patterns.
Conclusion Early-life lower respiratory tract infections ≤3 years are most consistently associated with lower lung function and increased risk of asthma in school-aged children.
- respiratory infection
- asthma
- clinical epidemiology
Statistics from Altmetric.com
Key messages
What is the key question?
Are early-life respiratory tract infections associated with lower lung function and an increased risk of asthma in school-aged children?
What is the bottom line?
When taking bidirectional associations into account, early-life lower respiratory tract infections are associated with lower lung function and an increased risk of asthma, while upper respiratory tract infections are not.
Why read on?
This large prospective cohort study shows, by using cross-lagged modelling, that early-life lower respiratory tract infections might have a direct effect on lung development and the risk of asthma.
Introduction
It has been hypothesised that respiratory tract infections in early life influence the risk of lower lung function1–4 and asthma5–10 in later childhood and adulthood. Respiratory tract infections could lead to higher airway sensitisation leading to airway obstruction and hyperreactivity11 and, subsequently, asthma. Respiratory tract infections might lead to persistent respiratory morbidity since both the immune and respiratory systems are under development in early life. In observational studies, findings on the association of respiratory tract infections with lung function or asthma have been inconclusive.1–10 Differences in results might be explained by power issues, ascertainment of respiratory tract infections, use of different lung function measurements, definitions of asthma, age of the outcome and use of covariates. Most studies that examined associations of respiratory tract infections with asthma focused on children at high risk for atopy,5–7 9 10 which leads to limited external validity. Additionally, child’s antibiotic12–17 and paracetamol17–19 use are suggested to be associated with increased risks of childhood asthma, and their effect on the associations of respiratory tract infections with lung function and asthma is unclear. Antibiotic or paracetamol use might have an effect on the risk of lower lung function and asthma, by influencing the microbiome or glutathione levels, respectively. However, any found association could also be the result of confounding by indication or reverse causality. Additionally, parents might change smoking behaviour as a result of respiratory infections, which could subsequently influence the risk of asthma. Therefore, second-hand smoke exposure might act as a mediator in this association. Associations of respiratory tract infections with asthma seem different between subgroups of children with or without allergic sensitisation, which suggests a modifying effect of allergy.6 7 Last, it is unclear whether early respiratory tract infections lead to lower lung function and asthma or that lower lung function and asthma, represented by wheezing at preschool age, lead to vulnerability for respiratory tract infections.
Therefore, we examined in a population-based prospective cohort study the association of early-life respiratory tract infections with lung function and asthma in school-aged children, taking bidirectional associations and preschool wheezing into account. Next, we examined if these associations are explained by children’s paracetamol and antibiotic use or modified by current inhalant allergic sensitisation status and if findings were specific for respiratory tract infections. This study adds to the current literature by examining the association of respiratory tract infections with lung function and asthma on a population-based level, using detailed and longitudinally measured information on both upper and lower respiratory tract infections and respiratory outcomes measures, applying a unique approach to identify bidirectional associations, and taking the effect of infections in general into account. With this, we aim to provide new evidence for a possible direct effect of respiratory tract infections on lung function and development.
Methods
Design
This study was embedded in the Generation R Study, a population-based prospective cohort study from early fetal life onwards in Rotterdam, The Netherlands. Women with a delivery date between April 2002 and January 2006 living in Rotterdam were eligible for participation in the study, as described previously.20 Written informed consent was obtained from parents or legal representatives of all participants. A total of 5197 children were included for the current analyses (see online supplementary figure S1).
Supplementary file 1
Early-life respiratory tract infections
Information on parental reported physician-attended upper and lower respiratory tract infections was obtained by questionnaires at the ages of 6 months and 1, 2, 3, 4 and 6 years. Response rates ranged from 71% to 80%. Questions about physician-attended upper respiratory tract infections included ear and throat infections, false croup and whooping cough, and questions about lower respiratory tract infections included bronchitis, bronchiolitis and pneumonia in the past 6 or 12 months (no or yes, not physician attended; yes, physician attended). We combined each individual respiratory tract infection into groups of upper and lower respiratory tract infections. For the cross-lagged analyses, respiratory tract infections were first analysed per year and to improve readability subsequently combined into early (≤3 years: at least one infection in this period vs no infections or late infections only) and late (3–6 years: at least one infection in this period vs no infections or early infections only) upper and lower respiratory tract infections. The cut-off point of 3 years was chosen to obtain sufficient power, based on end of highest velocity of maturation of lungs and the immune system until this age,21–23 and for consistency with categorisation of wheezing patterns.
School-age lung function and asthma
At age 10 years, FEV1, FVC, FEV1:FVC and forced expiratory flow after expiring 75% of FVC (FEF75) were measured by spirometry (MasterScreen-Pneumo, Jaeger Toennies (Viasys) CareFusion Netherlands). All curves were scored by two trained researchers according to the European Respiratory Society/American Thoracic Society guidelines24 and when necessary discussed with a senior researcher. Reproducible curves were converted into sex-adjusted, age-adjusted, height-adjusted and ethnicity-adjusted Z-scores.25 Current asthma was defined as (1) ever diagnosis of physician-diagnosed asthma with (2) either wheezing or any asthma medication use in the past 12 months. Questions on asthma and wheezing were adapted from the International Study on Asthma and Allergy in Childhood (ISAAC), and information on medication use was obtained at the research centre. Wheezing was reported by annual parental questionnaires from birth to age 4 years and at age 6 years. We combined preschool wheezing patterns into early (≤3 years) and late (>3–6 years) wheezing, similar to groups of respiratory tract infections.
Covariates
Information on maternal characteristics included educational level, body mass index at intake, parity, smoking during pregnancy, psychiatric symptoms, pet keeping and history of asthma and atopy and was obtained from multiple questionnaires during pregnancy. Mode of delivery and child’s sex, gestational age at birth and birth weight were obtained from midwife and hospital records at birth. Information on country of birth, breastfeeding, day care attendance, environmental tobacco smoke exposure and antibiotic and paracetamol use was obtained by multiple questionnaires at age 6 months to 2 years. Ethnicity was based on country of birth of both parents. Inhalant allergic sensitisation at the age of 10 years was measured by skin prick test using the ‘scanned area method’.26
Other infections
Information on infections other than respiratory tract infections were collected by similar questionnaires as respiratory tract infections and included physician-diagnosed gastroenteritis and urinary tract infection (no or yes, not physician attended; yes physician attended). Similarly to respiratory tract infections, other infections were combined into early (≤3 years) and late (3–6 years) infections.
Statistical analysis
First, we examined associations of respiratory tract infections with lung function measures and asthma using linear and logistic regression models, respectively. Analyses were adjusted for potential confounders, which were selected from literature,8 9 27–29 if they were related to respiratory tract infections and the outcomes of interest or if the effect estimate of the unadjusted analyses changed ≥10% when we additionally adjusted for a confounder. Missing data of covariates were imputed by the multiple imputation method using chained equations to select the most likely value for a missing response. Ten new datasets were created by imputation. Additionally, to take correlations between respiratory tract infections into account, both any and individual upper respiratory tract infections were adjusted for any preceding upper respiratory tract infections and any and individual lower respiratory tract infections for any preceding lower respiratory tract infections. We did not apply multiple testing due to strong correlations between the different infections and lung function measures, since that could potentially lead to false negative findings. Second, we examined if associations were mediated by children’s antibiotic or paracetamol use or environmental tobacco smoke exposure by additionally adjusting for these variables or were modified by inhalant allergic sensitisation by testing their interactive effects. Statistical analyses were performed with the Statistical Package of Social Sciences V.21.0 for Windows (SPSS). Third, we applied a cross-lagged model using Mplus V.7.11 for Windows (Muthén & Muthén). With a cross-lagged model, bidirectional associations between the exposure, respiratory tract infections until age 5 years and the outcome, wheezing until age 5 years and lung function or asthma at age 10 years can be studied within the same model. In this model, logistic or linear regression models are used to study the associations of early respiratory tract infections with early and late wheezing and lung function or asthma, of late respiratory tract infections with late wheezing and lung function or asthma and of early wheezing with late respiratory tract infections, while taking associations over time between respiratory tract infections and wheezing and lung function or asthma into account.30 31 These models enable us to disentangle the direction of the observed associations, such as whether respiratory tract infections influence the risk of lower lung function and asthma or vice versa. Last, sensitivity analyses were performed to examine the associations of gastroenteritis and urinary tract infection with lung function and asthma. These sensitivity analyses could prove insight to whether any associations of respiratory tract infections with lung function and asthma are due to a specific respiratory tract infection effect or due to a general infection status. All measures of association are presented with their 95% CIs.
Results
Subject characteristics
Maternal and child characteristics are shown in table 1. The highest prevalence of upper and lower respiratory tract infections was at the age of 2 years (24.0% and 8.5%, figure 1A, B, respectively). At age 10 years, mean FEV1 (SD) was 2.02 L (0.30), FVC 2.33 L (0.36), FEV1:FCV 86.6% (5.7) and FEF75 1.14 L/s (0.35) (table 1). Current asthma was present in 5.5% of the children. Current asthma was defined as ever asthma (9.4%), combined with wheezing (4.4%) or medication use (17.4%) in the past 12 months. Those not included in the analysis had, among others, mothers who were lower educated and had a higher prevalence of smoking during pregnancy. These children were more often born younger and had a lower birth weight and a lower prevalence of breastfeeding (online supplementary table S1).
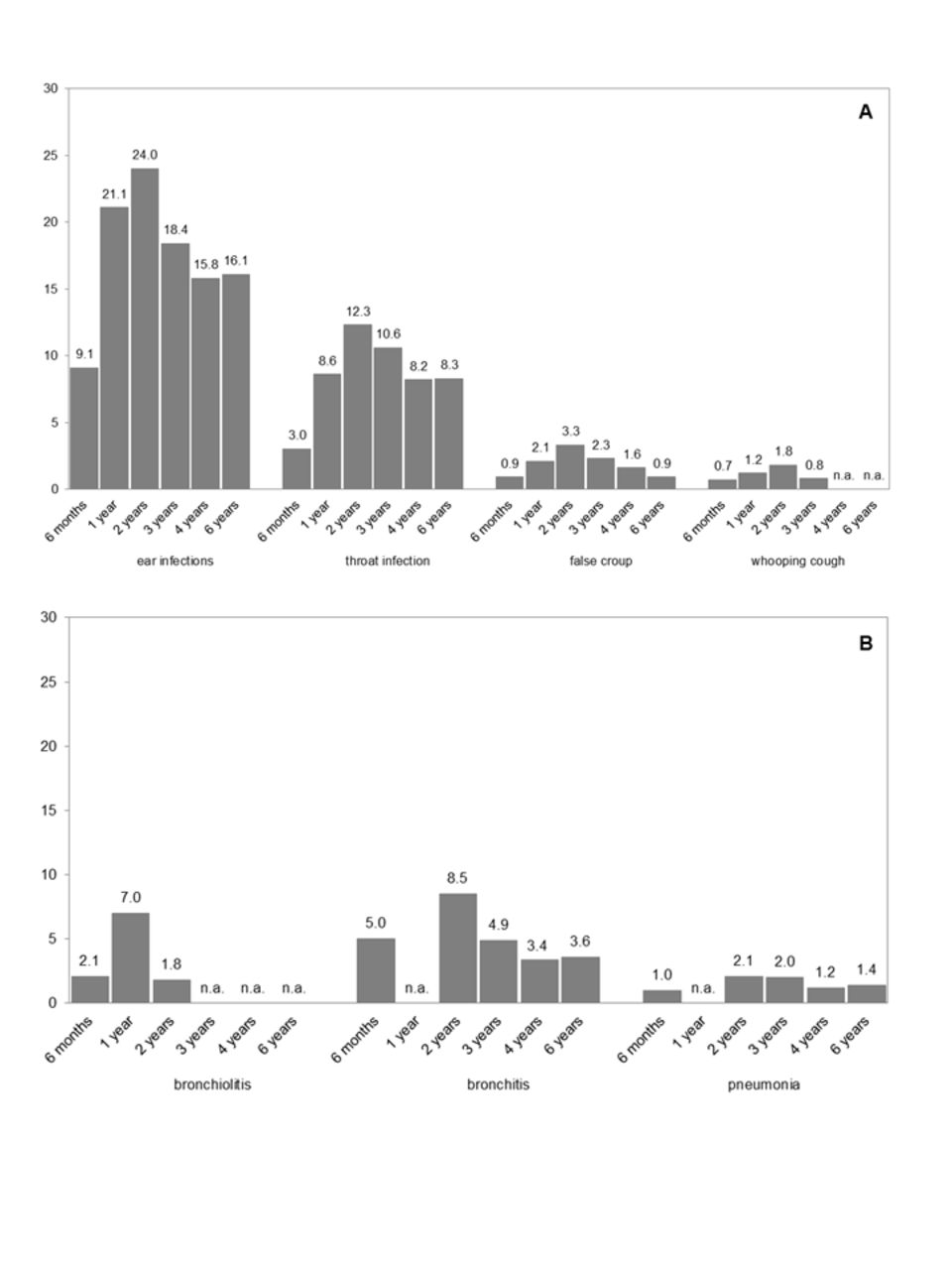
Prevalence of upper (A) and lower (B) respiratory tract infections. Values represent % of specific upper and lower respiratory tract infections per age and were not imputed. Not available: no data on this specific infection at this timepoint (n.a.).
Characteristics of children and their mothers
Respiratory tract infections and lung function or asthma
Results from models on crude and adjusted complete cases associations of upper and lower respiratory tract infections with lung function and asthma are shown in online supplementary tables S2 and S3, respectively. No major differences in the magnitude or direction of the effect estimates were observed between analyses with imputed missing data and complete cases only. Results of imputed datasets using per year analyses showed that upper respiratory tract infections were not consistently associated with lung function measures or asthma (table 2 and online supplementary table S4). Lower respiratory tract infections at ages 6 months and 1, 2, 3 and 6 years were associated with lower FEV1, FVC, FEV1:FVC or FEF75, with Z-score differences (95% CI) ranging from −0.19 (–0.32 to –0.05) to −0.34 (−0.50 to −0.18) (table 2). Lower respiratory tract infections at ages 2–6 years were associated with an increased risk of current asthma at 10 years, with ORs (95% CI) ranging from 4.19 (2.65 to 6.64) to 13.45 (7.22 to 25.05). Associations of individual upper and lower respiratory tract infections with lung function and current asthma are given in online supplementary tables S4 and S5.
Associations of any upper and lower respiratory tract infections with lung function and asthma at age 10 years
After adjustment for antibiotic and paracetamol use and environmental tobacco smoke exposure, the strength and direction of the effect estimates did not materially change (data not shown). We observed no consistent interactive effect of upper and lower respiratory tract infections and inhalant allergic sensitisation for the associations with lung function and asthma, (p values >0.05).
Cross-lagged modelling
Cross-lagged modelling showed no association of upper respiratory tract infections ≤3 years with lung function measures (figure 2A–C) or asthma (figure 2D). Compared with no upper respiratory tract infections >3–6 years, upper respiratory tract infections >3–6 years were associated with a higher FEV1:FVC and FEF75 (0.08 (0.02 to 0.15) and 0.10 (0.04 to 0.17), respectively, but not FEV1. Upper respiratory tract infections >3–6 years were associated with a decreased risk of current asthma (0.69 (0.49, 0.97)) (figure 2D).

Direction of associations of URTIs with wheezing and FEV1 (A), FEV1:FVC (B) FEF75 (C) and current asthma (D) at age 10 years. Values are ORs or change in Z-scores with their corresponding 95% CI derived from binomial logistic or linear regression models, respectively, using cross-lagged modelling, which takes bidirectional associations into account. Models are adjusted for maternal education, body mass index, parity, smoking during pregnancy, psychiatric symptoms during pregnancy, pet keeping, history of asthma or atopy, mode of delivery and child’s sex, gestational age at birth, birth weight corrected for gestational age at birth, breastfeeding and day care attendance. Arrows indicate the direction of the associations and if they are significant (bold) or non-significant (dashed). For (B-D) only the right lower quadrant of the figure is presented. All other directions and effect estimates of the associations were approximately the same as presented in (A). URTI, upper respiratory tract infection.
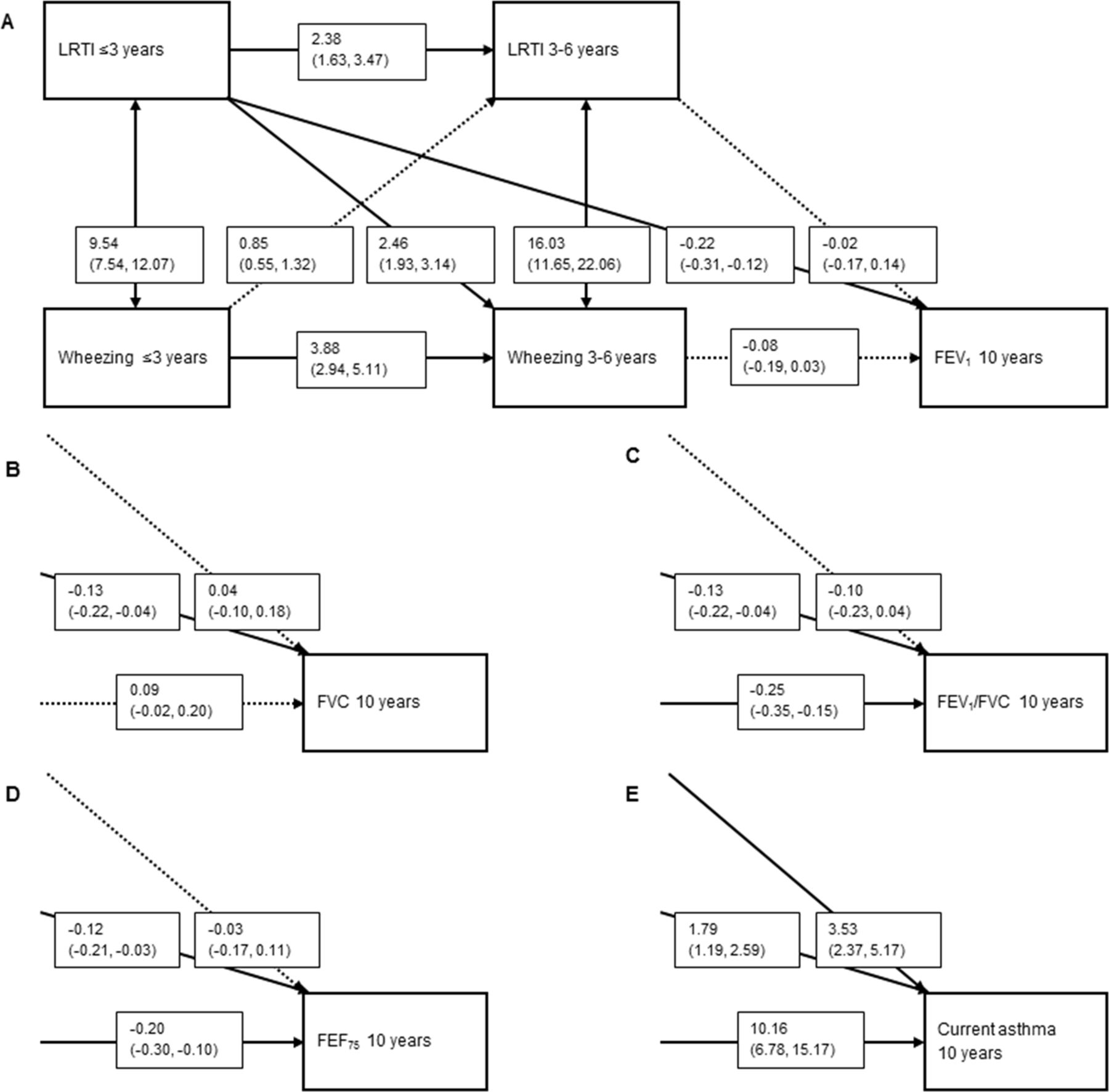
Lower respiratory tract infections ≤3 years were associated with lower FEV1, FVC, FEV1:FVC and FEF75 (range −0.12 (−0.21 to –0.03) to −0.22 (−0.31 to −0.12) (figure 3A–D). Lower respiratory tract infections ≤3 and >3–6 years were also associated with an increased risk of current asthma (1.79 (1.19 to 2.59) and 3.53 (2.37 to 5.17), respectively) (figure 3E). Lower respiratory tract infections >3–6 years were not associated with any lung function measurements. The directions from preschool wheezing patterns to later upper and lower respiratory tract infections were not significant.
{kind=link}
{kind=link}
{kind=link}
Direction of associations of LRTIs with wheezing patterns and FEV1 (A), FVC (B), FEV1:FVC (C), FEF75 (D) and current asthma (E) at age 10 years. Values are ORs or Z-scores with their corresponding 95% CIs derived from binomial logistic or linear regression models, respectively, using cross-lagged modelling, which takes bidirectional associations into account. Models are also adjusted for maternal education, body mass index, parity, smoking during pregnancy, psychiatric symptoms during pregnancy, pet keeping, history of asthma or atopy, mode of delivery and child’s sex, gestational age at birth, birth weight corrected for gestational age at birth, breastfeeding and day care attendance. Arrows indicate the direction of the associations and if they are significant (bold) or non-significant (dashed). For (B–E) only the right lower quadrant of the figure is presented. All other directions and effect estimates of the associations were approximately the same as presented in (A). LRTI, lower respiratory tract infection.
Other infections
Cross-lagged modelling showed that gastroenteritis was not associated with lung function measures (data not shown). Gastroenteritis ≤3 years, but not >3–6 years, was associated with an increased risk of current asthma (1.68 (1.13 to 2.47)) (online supplementary figure S2A). Urinary tract infections ≤3 years were associated with a higher FEV1 (0.18 (0.00 to 0.35), but not with current asthma (online supplementary figure S2B).
Discussion
We observed in large population-based prospective cohort study that lower respiratory tract infections ≤3 years were most strongly and consistently associated with lower lung function and an increased risk of current asthma at school age. These associations were not mediated by use of antibiotics or paracetamol and environmental tobacco smoke exposure and not modified by inhalant allergic sensitisation. Additionally, we observed that these associations were not bidirectional, independent of preschool wheezing patterns, and not due to a general infection status. Upper respiratory tract infections at any age were not associated with lower lung function, and only upper respiratory tract infections at the age of 2 years were associated with an increased risk of asthma.
Comparison with previous studies
Previous prospective cohort studies observed inconclusive associations of respiratory tract infections with lung function or asthma, both in children and in adulthood.1–10 Some studies that used viral sampling found that specific viral triggers, such as respiratory syncytial virus6–9 or rhinovirus,6 9 were associated with a 2.1-fold to 3.9-fold increased risk of wheeze or 2.6-fold to 9.8-fold increased risk of asthma in children aged 5–10 years. However, other studies showed that, not a specific viral trigger, but the number of infections was associated with an increased risk of asthma, current wheeze or bronchial hyper-reactivity at age 7 years.5 10 Two previous studies among children aged 56 and 10 years7 showed that associations of specific lower respiratory tract infections with asthma and wheeze were only present in children who were sensitised before the age of 2 years. Others showed no modifying effect of sensitisation for the associations of respiratory syncytial virus, rhinovirus infections or both with the risk of asthma at age 6 years.9 Some differences could be explained by differences in the size of study groups.4–7 9 Also, most studies examined children at high risk for atopy, which reduces generalisability.4–7 9 10 Most studies were focused on respiratory tract infections in either the first year or the first 3 years of life.4–7 9 10 32 Our findings are consistent with previous findings and now show that results are applicable to a general population, are not mediated by use of antibiotics or paracetamol and environmental tobacco smoke exposure and not modified by inhalant allergic sensitisation. Our sensitivity analysis for non-respiratory tract infections showed an association of gastroenteritis ≤3 years with asthma only. Since urinary tract infections at any age were not associated with any adverse respiratory outcome, the effect of gastroenteritis might be specific, and we speculate that this could be mediated by the intestinal microbiome.33 Another possibility, however, is that infections in general could have an effect on the immune system and thereby influence the risk of asthma.
When we took possible bidirectional associations into account, cross-lagged modelling showed that lower respiratory tract infections ≤3 years were associated with lower lung function and current asthma and lower respiratory tract infections at 3–6 years only with current asthma. By using cross-lagged models, we confirmed the direction of the association of respiratory tract infections with lung function and asthma, and not vice versa. These findings are supported by a randomised clinical trial, which observed that vaccination for respiratory syncytial virus infections led to a reduction of the number of wheezing days in the first year of life, suggesting causality from viral infection to wheeze.34
We observed that lower respiratory tract infections, specifically bronchitis, bronchiolitis and pneumonia, were associated with lower lung function and an increased risk of asthma. Previous studies suggested that childhood respiratory tract infections influence lung function at school age and in adulthood.1–3 35 36 In adults up to 70 years of age, early-life bronchitis3 36 and pneumonia1–3 36 were associated with a lower FEV1, FVC and, in lesser extent, a lower FEV1:FVC. Together with the present finding, these findings suggest that exposure to respiratory tract infections in early life might affect respiratory health during the life course.
Potential mechanisms
Lung development starts in utero and continues during childhood,21 37 similar to the development of the immune system.22 37 38 In early life, the developing respiratory and immune system could be affected by lower respiratory tract infections, leading to persistent adverse adaptations and subsequently lower lung function and an increased risk of asthma. Non-specific immune responses mediated by epithelial cells and phagocytes and adaptive immune responses mediated by T cells could contribute to airway inflammation in response to viral triggers.38 Early airway infections could lead to changes in endothelial cell physiology, such as increased vascular permeability and, hence, bronchial wall oedema.39 40 Because of the immaturity of the respiratory and immune systems at a young age, these processes with potential persistent consequences are more likely to occur when lower respiratory tract infections occur early in life. Our findings are in line with this hypothesis because we observed that mainly lower respiratory tract infections ≤3 years were associated with lower lung function and increased risk of asthma. The effect of upper respiratory tract infections on the lungs seems to be less distinct most probably because upper respiratory tract infections do not affect the lungs directly.
The immune system is also important for the resolution of airway inflammation after infections, and a less-developed immune system could potentially lead to persistent changes of airway physiology and function after infections.39 To date, the immunological pathways responsible for the persistence of structural and functional abnormalities after respiratory tract infections have not yet been identified. The immune response to infections and the risk of developing lower lung function and asthma could both be dependent on common factors, such as the microbiome41 or (epi)genetic factors,39 and need to be examined in future studies.
Strengths and limitations
This study was embedded in a population-based, prospective cohort study with a large number of participants, and detailed and longitudinally measured information on both upper and lower respiratory tract infections and respiratory outcomes measures. Furthermore, we applied a unique method to identify bidirectional associations using cross-lagged modelling. Since the study was not limited to a high-risk population, the findings are applicable to the general population. However, some limitations apply to our study. First, selection bias towards a more affluent and healthy population might have been present. Also, we used multiple imputation to reduce potential bias due to missing data in covariates. By using this method, we assumed that data in covariates were missing at random. However, it might be possible that some data were missing not at random, which may have led to bias.42 Second, information on respiratory tract infections was parental-based information, collected with questionnaires, which might have led to recall or misclassification bias. If so, we expect this possible misclassification to be random because information on infections was collected before the outcome was known and would most probably have led to an underestimation of our observed effect estimates. Our study lacked viral or bacteriological sampling at the time of symptoms of respiratory tract infections, although it is suggested that not the specific microbial trigger but respiratory tract infections in general are important for the risk of asthma.5 Third, information on asthma and wheezing was obtained by questionnaires. Although these questionnaires were adapted from ISAAC,43 which was validated in various age groups and is considered as a reliable measure in epidemiological studies, misclassification due to self-report might still have been present. Prevalences of early and late wheezing in our study slightly differ from previous birth cohort studies44 due to the definition used for optimal cross-lagged modelling. Fourth, we did not have lung function measurements before the occurrence of respiratory tract infections. Therefore, we cannot distinguish whether the lower lung function is a result of the respiratory tract infections only or whether it was already present before the infections occurred.45 It has been suggested, however, that lower respiratory tract infections impair lung function independent of lung function at younger age.46 We partly addressed this issue by our statistical effort using cross-lagged modelling. Fifth, inhalant allergic sensitisation was measured at the age of 10 years. Early measurements or longitudinal patterns of allergic sensitisation might be needed to better examine the intermediating role of allergy. Last, even though we corrected for numerous confounders, residual confounding due to unmeasured confounders, for example, genetic susceptibility47 or maternal infections during pregnancy,48 could have affected our results.
In conclusion, our results suggest that lower respiratory tract infections ≤3 years are most strongly and consistently associated with lower lung function and increased risk of asthma at school age, while lower respiratory tract infections at 3–6 years were associated with asthma only. Upper respiratory tract infections were not associated with lower lung function or an increased risk of asthma, except at the age of 2 years with asthma. Cross-lagged modelling showed that observed associations were not bidirectional, independent of wheezing in early life and most likely not due to infections in general. Therefore, our findings support the hypothesis that early-life respiratory tract infections might have a direct effect on lung development and the risk of asthma. Further studies are needed to explore the possible underlying immunological and pathophysiological pathways.
Acknowledgments
The Generation R Study is conducted by the Erasmus Medical Centre in close collaboration with the School of Law and the Faculty of Social Sciences at the Erasmus University, Rotterdam, the Municipal Health Service, Rotterdam area and the Stichting Trombosedienst and Artsenlaboratorium Rijnmond (Star-MDC), Rotterdam. We gratefully acknowledge the contribution of children and their parents, general practitioners, hospitals, midwives and pharmacies in Rotterdam.
References
Footnotes
Contributors ERvM, HTdD and LD contributed to the conception and design, acquisition of data and analyses and interpretation of the data, drafted the article, revised it critically for important intellectual content and gave final approval of the version to be published. NJE, PWJ, HAM, IR, JCdJ and VJ contributed to the conception and design and acquisition of data, revised the drafted manuscript critically for important intellectual content and gave final approval of the version to be published.
Funding The Generation R Study is made possible by financial support from the Erasmus Medical Centre, Rotterdam, the Erasmus University Rotterdam, the Netherlands Organization for Health Research and Development and the Ministry of Health, Welfare and Sport. PWJ received a grant from the Dutch Diabetes Foundation (grant no. 2013.81.1664). VJ received grants from the Netherlands Organization for Health Research and Development (VIDI o16.136.3610) and the European Research Council (ERC-2014-CoG-648916). LD received funding from the Lung Foundation Netherlands (no. 3.2.12.089; 2012). The project received funding from the European Union’s Horizon 2020 research and innovation programme (LIFECYCLE project, grant agreement no. 733206; 2016) and from cofunded ERA-Net on Biomarkers for Nutrition and Health (ERA HDHL), Horizon 2020 (grant agreement no. 696295; 2017), ZonMW The Netherlands (no. 529051014; 2017), Science Foundation Ireland (no. SFI/16/ERA-HDHL/3360) and the European Union (ALPHABET project). The researchers are independent from the funders. The study sponsors had no role in the study design, data analysis, interpretation of data or writing of this report.
Competing interests None declared.
Ethics approval Medical ethical committee of the Erasmus MC, University Medical Centre Rotterdam, Rotterdam, The Netherlands (MEC-2012-165).
Provenance and peer review Not commissioned; externally peer reviewed.