Article Text

Abstract
Cardiovascular and skeletal muscle manifestations constitute important comorbidities in COPD, with systemic inflammation proposed as a common mechanistic link. Fibrinogen has prognostic role in COPD. We aimed to determine whether aortic stiffness and quadriceps weakness are linked in COPD, and whether they are associated with the systemic inflammatory mediator—fibrinogen. Aortic pulse wave velocity (aPWV), quadriceps maximal volitional contraction (QMVC) force and fibrinogen were measured in 729 patients with stable, Global Initiative for Chronic Obstructive Lung Disease (GOLD) stages II–IV COPD. The cardiovascular and muscular manifestations exist independently (P=0.22, χ2). Fibrinogen was not associated with aPWV or QMVC (P=0.628 and P=0.621, respectively), making inflammation, as measured by plasma fibrinogen, an unlikely common aetiological factor.
- copd pathology
Statistics from Altmetric.com
Introduction
Cardiovascular disease and locomotor muscle dysfunction are two important comorbidities in COPD, occurring in up to 50%1 2 of patients, and relating to both increased healthcare utilisation and mortality, thus representing potential therapeutic targets. Both share common risk factors, including smoking, exacerbations and physical inactivity, but systemic inflammation has been also proposed as a mechanistic link between them. If so, novel anti-inflammatory therapies might simultaneously target both manifestations. Fibrinogen is the only inflammatory biomarker with regulatory approval as a drug development tool in COPD, but hitherto the value of fibrinogen in predicting these phenotypes has not been examined.
In the ‘Evaluating the Role of Inflammation in Chronic Airways disease’ (ERICA) study, we investigated whether cardiovascular and skeletal muscle manifestations overlap in COPD and whether these manifestations are associated with plasma fibrinogen. ERICA is unique among multicentre studies in objectively quantifying these non-pulmonary manifestations of COPD.
Methods
Methods have been described previously.3 ERICA is a prospective, observational study that recruited subjects from hospital and community settings, and was registered with the UK Clinical Research Network Study Portfolio (http://public.ukcrn.org.uk/Search/StudyDetail.aspx?StudyID=11101). Participants provided written consent to participate.
Subjects were aged 40–90 years with Global Initiative for Chronic Obstructive Lung Disease (GOLD) stages II–IV COPD judged by postbronchodilator spirometry. Relevant exclusion criteria were alpha-1-antitrypsin deficiency or significant coexisting pulmonary disease; subjects were clinically stable for >4 weeks. Comorbid disease was not an exclusion criterion.
Subjects underwent multiple phenotypic assessments, including aortic pulse wave velocity (aPWV), quadriceps maximal volitional contraction (QMVC) force, 6 min walk distance (6MWD) and fibrinogen.
APWV of >10 m/s was chosen as a surrogate measure of cardiovascular disease.4 Quadriceps weakness was defined according to the gender-specific Seymour equation.2 The ‘Cardiovascular’ group contained subjects with elevated aPWV alone, ‘Muscle’ contained subjects with skeletal muscle weakness only, ‘Both’ contained subjects with both manifestations and ‘Neither’ had subjects with neither manifestation.
Multiple linear regression analyses were conducted to estimate the dependence of QMVC and aPWV on fibrinogen, with adjustment for known or expected confounders. Non-normally distributed variables were log-transformed prior to analysis.
Χ2 testing was carried out to test whether QMVC and aPWV were independently associated.
Analyses were performed using R V.3.0.0 for Microsoft Windows with RStudio V.0.98.953.
Results
Seven hundred and forty-six people were screened; 729 met the inclusion criteria and 617 subjects had both aPWV and QMVC measurements. Table 1 describes the baseline demographics for the whole cohort and phenotypic groups. The population had a mean age of 67 years, 61% were male, with a mean FEV1 of 52.2% predicted, mean aPWV of 10.3 m/s and mean QMVC of 30.6 kg (68.2% predicted).
Baseline demographics
Of 617 subjects, 194 (31.4%) were classified as ‘Neither’, 137 (22.2%) as ‘Muscle’, 154 (30.0%) as ‘Cardiovascular’ and 132 (21.4%) as ‘Both’ (supplementary eFigure 1). Overall, 269 out of 617 (43.6%) subjects had muscle weakness and 286 out of 617 (46.4%) had elevated aPWV. Χ2 test confirmed that cardiovascular and skeletal muscle manifestations were independent (test statistic 1.49; P = 0.22).
Supplementary file 1
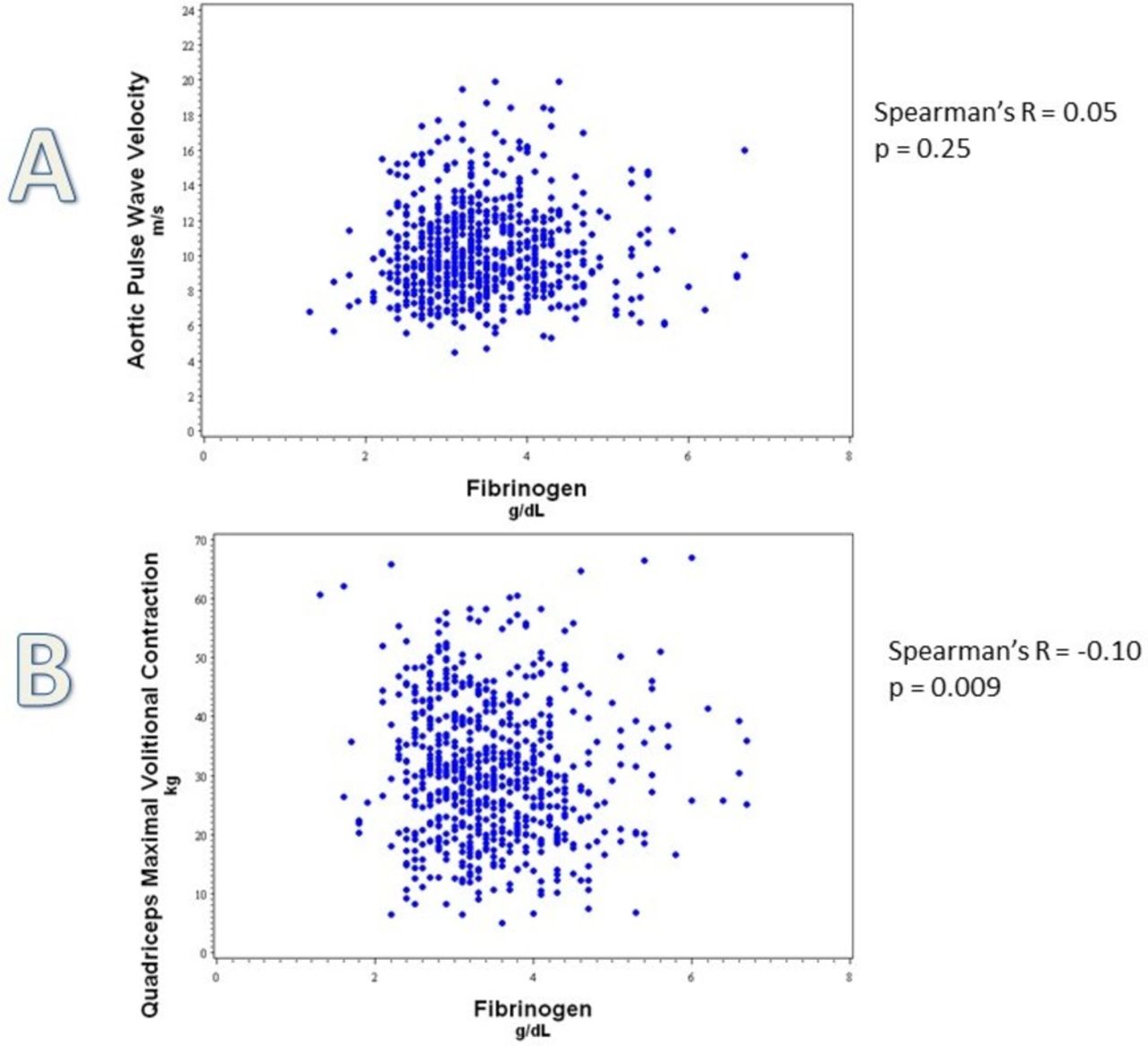
Fibrinogen was not siginificantly associated with either APWV or QMVC (P =0.628 and P =0.621) (figure 1, supplementary eTable 2 and eTable 3).

{kind=link}
Relationship between fibrinogen and aPWV and QMVC. Scatterplot demonstrating relationship between (A) fibrinogen (g/L) and arterial stiffness, as measured by aPWV (m/s) in 651 subjects with COPD, with Spearman’s correlation of 0.05 and P=0.25; and (B) fibrinogen (g/L) and quadriceps weakness, as measured by QMVC (kg) in 684 subjects with COPD, with Spearman’s correlation −0.10 and P=0.009. aPWV, aortic pulse wave velocity; QMVC, quadriceps maximal volitional contraction.
Age, gender, supine heart rate, supine mean arterial pressure and diabetes were significantly associated with aPWV (online supplementary eTable 2). Smoking history, FEV1, previous self-reported myocardial infarction, antihypertensive therapy and cholesterol-lowering therapy were not significantly associated.
QMVC was significantly and independently associated with age, gender, fat-free mass and FEV1 (online supplementary eTable 3). Smoking history and height were not significant associations.
Discussion
Cardiovascular and skeletal muscle manifestations are more prevalent in COPD than previously reported, but do not coexist more frequently than is expected by chance and therefore likely require different therapeutic approaches. Furthermore, fibrinogen was not associated with quadriceps strength or aortic stiffness, suggesting that it is unlikely to be useful in clinical trials addressing cardiovascular or skeletal muscle manifestations in COPD. Our findings do not support the concept that anti-inflammatory therapy aiming to reduce fibrinogen is likely to reduce aortic stiffness or improve quadriceps strength in COPD.
Our estimate of cardiovascular comorbidity agrees with previous estimates. Associations with aPWV in our patients were similar to those previously observed in healthy subjects.4 Interestingly fibrinogen was not associated with arterial stiffness, despite prior reports of association of aPWV with interleukin-6 and C reactive protein (CRP); moreover, we failed to find associations between white cell count, CRP and aPWV or QMVC (online supplementary eTables 4–13). Furthermore, we did not find an association between FEV1 and aPWV, in contrast to smaller studies,5 suggesting that aPWV is not linked to the severity of airflow limitation in people diagnosed with COPD.
In our cohort, the prevalence of quadriceps weakness (43.6%) is higher than previously reported.2 In COPD, muscle weakness precedes the development of whole body cachexia, with relative upper limb sparing6; therefore, measures other than QMVC (eg, hand grip strength or bioimpedance) are likely to underestimate the prevalence of muscle dysfunction.
This study is one of the few to have examined the coexistence of cardiac and muscle manifestations. Using different methodologies prior studies found lower prevalences; Vanfleteren et al 7 reported 10% of patients in their cardiovascular cluster had muscle wasting while 7% of patients with cachexia had a history of myocardial infarction. Siebeling et al 8 estimate the coexistence of cardiovascular and muscular comorbidities at 2%–3%. Of our cohort, 21.4% exhibited both elevated aPWV and quadriceps weakness; χ2 testing confirmed that there is not an independent, overlap syndrome.
Our study supports recent data that refute the link between low-grade systemic inflammation and cardiovascular or muscle manifestations in COPD.7 9 Persistent systemic inflammation is present in 16% of patients with COPD10; given that we report prevalence of both aPWV and QMVC is much higher than 16%, inflammation seems an improbable key aetiological factor. The cross-sectional nature of our data means that a temporal link between PWV and QMVC or systemic inflammation cannot be assessed at this stage, although follow-up of the cohort is ongoing. Additionally, it is important to note that our study allowed the cross-sectional assessments to be carried out over either a single visit or two visits within a 3-month period; therefore, we acknowledge that in some patients inflammatory markers were measured on a separate day to aPWV and QMVC. A further limitation is that 112 patients of the entire data set did not have the three key measures assessed here. These patients were similar in most respects to the cohort analysed here but had a lower FEV1 and 6MWD (data not shown).
In conclusion, cardiovascular and skeletal muscle manifestations are prevalent in COPD, with muscle weakness being more common than previously thought. These extrapulmonary manifestations are distinct and need to be addressed individually. Neither aortic stiffness nor quadriceps weakness relates to plasma fibrinogen, suggesting that this is not a useful biomarker for trials addressing these manifestations and that inflammation is an unlikely aetiological factor.
Acknowledgments
The authors would like to thank the subjects who participated in the study, as well as the study teams at all five participating centres, especially Jessica Middlemiss (Cambridge Clinical Trials Unit) and Cayley Smith (Muscle Lab, Royal Brompton Hospital), who were instrumental in helping to set up the study.
Footnotes
RT-S, IBW and MIP contributed equally.
Contributors MIP, DM, JRF, CMM, CEB, JRC, WM, JF, NSG, MF, JRC, DAL, PMAC, BEM, RT-S and IBW all made substantial contributions to the conception and design of the work. MIP, DM, JRF, MA, CMM, CEB, JRC, WM, JF, MM, SN, NSG, MF and IBW made substantial contributions to the acquisition and analysis of data for the work. All authors contributed to the interpretation of the data, drafting and revision of the manuscript, and final approval of the version submitted for publication. All authors take accountability for all aspects of the work.
Funding This study was funded by a grant from Innovate UK. GlaxoSmithKline, a consortium partner, made contributions in kind towards study management. The UK Clinical Research Network contributed towards the study at all participating sites. Subjects from the Wales Heart Research Institute, Cardiff, were simultaneously recruited to the ARCADE study (ClinicalTrials.gov Identifier NCT01656421), which was funded by GSK. IBW, JRC and CMM have received funding support from the National Institute for Health Research (NIHR) Cambridge Comprehensive Biomedical Research Centre. Part of the work was undertaken at the NIHR Respiratory Biomedical Research Unit at the Royal Brompton and Harefield NHS Foundation Trust and Imperial College London, which part-funded DM and MIP’s salary.
Competing interests MIP has received payment to his institution or himself for advice on skeletal muscle weakness in COPD from GSK, Novartis, AZ, Pfizer, Lilly and Astellas. DM is an employee and shareholder of GSK. JRF, CMM, MM, SN and NSG have no conflict of interest to report. CEB reports grants from Innovate UK (formerly Technology Strategy Board (TSB) UK) during the conduct of the study; advisory board fees from GSK paid to their institution, grants from GSK and grants from MRC/ABPI outside the submitted work. JRC reports grants from TSB/MRC, during the conduct of the study; personal fees from GSK, outside the submitted work. WM received research support from GlaxoSmithKline and Pfizer, and was on advisory committees of Almirall, GlaxoSmithKline, Novartis and Pfizer; he was a speaker for AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Janssen and Novartis. JF received speaker fees from GSK. MF acknowledges receipt of an imaging fellowship award from GSK. JRC is employed full-time by Cambridge University Hospitals National Health Service Foundation Trust and is obligated to spend 50% of his time on GSK clinical trial research, representing a significant relationship; however, he receives no other benefits or compensations from GSK. DAL reports grants and personal fees from GSK, and personal fees from Grifols, outside the submitted work. PMAC has advised Boehringer Ingelheim, GSK, AstraZeneca and Takeda on the design and conduct of clinical trials, and has spoken at meetings sponsored by these companies and by Novartis; he has no stock holdings in any pharmaceutical company or connection with the tobacco industry. BEM and RT-S are shareholders and employees of GSK. IBW reports grants from TSB and GSK during the conduct of the study, and grants from GSK outside the submitted work.
Patient consent Obtained.
Ethics approval The Cambridge South Research Ethics Committee (reference 11/EE/0357) approved the study.
Provenance and peer review Not commissioned; internally peer reviewed.