Article Text

Abstract
Objective To assess the effectiveness and cost-effectiveness of primary care (PC) and sleep unit (SU) models for the management of subjects with suspected obstructive sleep apnoea (OSA).
Methods Multicentre, open-label, two-arm, parallel-group, non-inferiority randomised controlled trial. A total of 302 subjects with suspected OSA and/or resistant hypertension were consecutively enrolled, 149 were treated at 11 PC units and 153 patients at a SU. The primary outcomes were a 6-month change in the Epworth Sleepiness Scale (ESS) score and Health Utilities Index (HUI). The non-inferiority margin for the ESS score was −2.0.
Results A total of 80.2% and 70.6% of the PC and SU patients were diagnosed with OSA, respectively, and 59.3% and 60.4% of those were treated with CPAP in PC and SU units, respectively. The Apnoea–Hypopnoea Index was similar between the groups (PC vs SU (median (IQR); 23.1 (26.8) events/h vs 21.8 (35.2) events/h), and the baseline ESS score was higher in the PC than in the SU group (10.3 (6.6) vs 9 (7.2)). After 6 months, the ESS score of the PC group decreased from a mean of 10.1 to 7.6 (−2.49; 95% CI −3.3 to −1.69), and that of the SU group decreased from 8.85 to 5.73 (−3.11; 95% CI −3.94 to 2.28). The adjusted difference between groups for the mean change in the ESS score was −1.25 (one-sided 95% CI −1.88; p=0.025), supporting the non-inferiority of PC management. We did not observe differences in the HUI between groups. The cost analysis showed a median savings of €558.14/patient for the PC setting compared with the SU setting.
Conclusions Among patients with suspected OSA, the PC model did not result in a worse ESS score or HUI than the specialist model and generated savings in terms of management cost. Therefore, the PC model was more cost-efficient than the SU model.
Trial registration Results; >>NCT02234765, Clinical Trials.gov.
- sleep apnoea
Statistics from Altmetric.com
Key messages
What is the key question?
Is the comprehensive management of obstructive sleep apnoea (OSA) followed by primary care as effective as conventional OSA management in a specialised sleep unit?
What is the bottom line?
The high prevalence of OSA, its chronic character and its consequences make the exclusive management of this pathology by sleep unit unfeasible. Similar to other chronic and prevalent diseases, the comprehensive care and management of OSA should involve other clinical settings.
Why read on?
The comprehensive management of OSA in a primary care setting is a cost-efficient and feasible alternative to the standard management performed in the specialised sleep units.
Introduction
Obstructive sleep apnoea (OSA) is a common disease that affects more than 10% of the adult population and becomes more prevalent with age.1 It is caused by the intermittent collapse of the upper airway during sleep, which leads to transient asphyxia. OSA is an important public health issue and has been shown to be associated with the onset or worsening of hypertension,2 3 cardiovascular diseases,4 stroke5 and a reduced quality of life6; it also has a causative role in work7 and traffic accidents.8 Notably, OSA should be suspected in patients with resistant hypertension (more than 70% of patients have OSA), in whom its treatment with CPAP has an effect on blood pressure control.9
Only approximately 10% of individuals with OSA are diagnosed and treated. This shortfall has direct consequences on public health because of the high financial costs of untreated OSA.10 A steady demand for specialised sleep units (SUs) for sleep service provision and growing waiting lists for sleep physician consultations has been observed. The high prevalence of this disease, its chronic character and its consequences make the exclusive management of this pathology using a SU unfeasible. Similar to other chronic and prevalent diseases, the comprehensive care and management of OSA should involve other clinical settings. A new model for managing sleep apnoea in primary care (PC) settings has recently been proposed as a realistic alternative.11 12 Previous studies performed exclusively in patients with a high pre-test probability of having OSA have revealed that the model of management in a PC unit is feasible and exhibits comparable effectiveness with the specialist SU model.11 13 Nevertheless, the comprehensive cost-effective management of all patients with suspected OSA in PC settings has implications for the diagnostic methods used, treatment decisions and patient follow-up procedures, and has yet to be explored.
In this randomised controlled trial, we aim to compare the clinical efficacy and within-trial costs of the comprehensive management of patients with suspected OSA in a PC setting with specialised SUs. We hypothesised that the comprehensive management of OSA in a PC setting is a cost-effective alternative to the standard care and management that are exclusively performed in a specialised SU.
Methods
Study design and patients
This study was conducted in the SU of one teaching hospital and 11 PC units in Lleida (Catalonia, Spain). The methodology of the study has been published previously.14 In this multicentre, open-label, two-arm, parallel-group, prospective, non-inferiority randomised controlled trial, patients were consecutively recruited from 11 PC units during visits for suspected OSA (chronic snoring, apnoea and/or excessive daytime sleepiness (EDS)) or resistant hypertension (defined as blood pressure (BP) higher than the therapeutic goals (ie, average systolic BP ≥130 mm Hg, average diastolic BP ≥80 mm Hg or both) despite the concurrent use of at least three antihypertensive agents prescribed at doses that provide optimal benefit, with one of these drugs ideally being a diuretic agent.15 We compared the comprehensive management of patients with suspected OSA in an ambulatory PC-based management system with the management of patients in a specialist SU. Patient enrolment started in June 2014 and was completed in December 2015. The inclusion criteria were as follows: patients older than 18 years who visited a PC unit because of suspected OSA and/or resistant hypertension. Suspected OSA was based on the presence of (1) chronic snoring, (2) partner-objectified apnoea and/or (3) EDS (self-reported in response to the question “Do you have a tendency to fall asleep during the day in situations where it should not happen?”) The exclusion criteria were advanced heart failure (New York Heart Association class III or IV), associated advanced pathology (including any active neoplasm or tumour), a psychiatric disorder, restless legs syndrome, pregnancy, another form of dyssomnia or parasomnia, previous treatment with CPAP and/or pulmonary illness. Demographic and anthropometric data were collected, including sex, age, weight, height, Body Mass Index (BMI) and waist circumference.
Randomisation and masking
Web-based/computer-based randomisation was performed using a secure, automated, password-protected system. Participants were randomly assigned to the PC or SU group. Block randomisation was not applied in this study. Patients were recruited and randomised in the PC settings. After patient recruitment and randomisation in PC, a baseline visit was scheduled to be performed in the assigned setting (PC or SU). Patients randomised to the PC unit were treated in the unit in which they were recruited. An open-label design was required because of the nature of the study and to allow us to reflect real-world clinical practice. Each participating centre had access to their own data, and only the principal investigator (FB) had access to the entire database.
Procedures
Patients were consecutively recruited during medical visits for suspected OSA and/or resistant hypertension. Interested patients provided consent and completed baseline assessments. Patients meeting eligibility criteria were randomised into either a PC management group or a specialist SU management group. All patients received sleep hygiene and hygienic-dietary measures. Follow-up visits were conducted by specialised nurses at the SU or by general practitioners/nurses in the PC setting. All patients were followed up at 6 months. Patients treated with CPAP were followed up at 1, 3 and 6 months and patients with OSA without CPAP treatment at 3 and 6 months. Additionally, a telephone call was made to patients treated with CPAP to reinforce the necessity of adequate CPAP adherence. The patients received education and support for setting up and using the CPAP device, advice on managing CPAP-related adverse effects, encouragement for CPAP compliance and education about lifestyle changes. The follow-up evaluation actions are described in online supplementary etable 1. The patients received education and support for setting up and using the CPAP device, advice on managing CPAP-related adverse effects, encouragement for CPAP compliance and education regarding lifestyle changes.
Supplemental material
One PC physician and one nurse from each of the 11 PC units in the study participated in an education programme (6 hours) that included the theoretical and practical aspects of managing patients with sleep apnoea. Eight of the 11 participating PC centres that participated in a previous study by our group12 had previously received specific training in managing patients with OSA before completing the new education programme. This programme included the theoretical and practical aspects of managing patients with sleep apnoea and comprised specific information about the diagnosis of sleep apnoea and treatment decisions. Additionally, information concerning treatment follow-up, including adherence monitoring, strategies for reinforcing adequate adherence and management of CPAP-related adverse effects, was included in the education programme.
Primary care management
The patients allocated to the PC group were exclusively managed by the PC unit. The PC physicians decided on the type of sleep study (respiratory polygraphy (RP) or full polysomnography (PSG)) and the decision whether to prescribe CPAP treatment. Moreover, patients received education regarding lifestyle and behavioural modifications of benefit in the treatment of OSA. These modifications included dietetic and sleep hygienic measures. The realisation and scoring of sleep studies (PSG or RP) was performed by a certified sleep specialist from a private external company. The decision whether to prescribe CPAP treatment was made exclusively by the PC physician without considering any recommendations by the personnel of the private external company.
The follow-up protocol was similar to a protocol performed in a previous study by our group.12 The patients participated in the follow-up sessions in person at 1, 3 and 6 months. Additionally, as necessary, the patients had the option of telephone consultations with the PC physician or nurse who conducted the follow-up visits. CPAP compliance was measured from the internal clocks of the devices.
Specialist sleep unit management
The patients allocated to the SU group were referred to the SU through PC. The diagnostic method was RP or PSG, according to the criteria and standard protocol of the SU. The patients met the SU physician or nurse in person to review their progress and receive education and support for the CPAP set-up, advice about managing CPAP-related adverse effects, encouragement to comply with the CPAP recommendations and to ensure adherence to its use, and be educated about lifestyle changes. The follow-up of the patients in the SU was equal to the follow-up in PC management.
Sleep study and CPAP treatment
Sleep study characteristics and CPAP treatment description are detailed in the online supplementary appendix.
Endpoints
Primary outcomes
The primary outcomes were the Epworth Sleepiness Scale (ESS) score and Health Utilities Index (HUI) at 6 months after the start of the chosen treatment. Changes in effectiveness (ESS scores and HUI) were analysed to assess the cost-effectiveness, which was based on both the ESS score and HUI calculated using the EuroQoL five-dimensions questionnaire (EQ-5D).16 The ESS score was assessed at baseline and at each follow-up visit. The EQ-5D was assessed at baseline and at 6 months. The ESS score is based on a validated questionnaire17 that assesses daytime sleepiness, which ranges from 0 (no daytime sleepiness) to 24 (high level of daytime sleepiness) points and was recorded at baseline and at the 6-month follow-up visit.
Secondary outcomes
The following variables were assessed at the 6-month follow-up: CPAP compliance (measured using the number of hours of CPAP use per day according to the internal clock of the CPAP device), patient satisfaction (measured using a visual analogue scale ranging from 0 to 100), BMI and BP.
Statistical analysis
The sample size was determined to allow assessments of the non-inferiority of the ESS score in PC settings compared with that in SU settings. A non-inferiority margin of −2 was specified based on clinically relevant differences,18 variability in ESS scores19–21 and consensus among researchers.22 Based on the power computations, a minimum of 280 patients (140 in each treatment group) were required to achieve an 80% statistical power. These estimations considered a type 1 error of 5%, a SD of 5.9 (moderately greater than previously reported values from similar studies23) and a loss to follow-up of less than 30%.
Non-inferiority of the PC treatment was assessed using a lineal model adjusted for the baseline ESS score. The Epworth value at 6 months was imputed to the dropout patients. The imputation assumes that all dropouts in the hospital arm improved the established clinical relevance (2 points of ESS) while all dropouts in the primary care arm did not improve. We decided this imputation due to non-inferiority contrast.24 25 Statistical significance was assessed using a one-sided p value and 95% CI. The cost-effectiveness analysis was performed using the total costs for each arm (unit cost; see online supplementary appendix etable 6) based on treatment effectiveness (ESS score and HUI). A probabilistic sensitivity analysis was performed using the bootstrap method, which was represented in a cost-effectiveness plan. In the cost-effectiveness analysis, the patients who did not perform the baseline visit were excluded and the baseline imbalance of the ESS effectiveness measure was considered by applying the methodology proposed by Schilling et al.26 Additionally, we performed a univariate sensitivity analysis in which unit costs were individually varied over a specified range while the remaining values were maintained at their baseline values. Thus, we obtained an assessment of the impact of the change on the results of the analysis. Each parameter ranges between 0.80 and 1.20 times its baseline value. The unit costs were based on the Catalan Institute of Health tables (CVE-DOGC-A-13051031-2013; http://portaldogc.gencat.cat/utilsEADOP/PDF/6326/1287494.pdf). The supplementary material details the methods used for the cost-effectiveness analysis.
Differences in the secondary outcomes between the PC and SU groups at 6 months were assessed using ordinary least-squares linear models adjusted for the baseline values. A two-sided p value and 95% CI were used.
The intention-to-treat (ITT) sample included all randomised patients. For the per-protocol (PP) sample, patients who completed the follow-up were included. The non-inferiority analysis was performed on both the ITT and PP samples. The results obtained from both analyses were compared. HUI and the secondary outcome measures were analysed in the ITT sample after the multiple imputation of missing data. The multiple imputation procedure consisted of chained equations, for which 20 complete databases were obtained. The multiple imputation was calculated following the methodology proposed by Groothuis-Oudshoorn and Buruen.27 To observe the effect of the data imputation, we replicated the analysis of the data without this imputation (online supplementary appendix etable 3). The R package ‘mice’ was used for these calculations. All statistical analyses and data processing procedures were performed using R software, V.3.3.1.28
Results
Description of the groups
Figure 1 shows a flow diagram outlining the recruitment and randomisation procedures. Three hundred two individuals were randomly assigned to the PC or SU group: 147 of the 149 patients randomised to the PC group (98.6%) completed the baseline visit, and 140 of the 153 randomised to the SU group (91.5%) completed the baseline visit. Nevertheless, from the patients who completed the baseline visit, the percentage of patients who completed the 6-month follow-up was similar between the two settings (83.6% in PC and 84.6% in SU). The time for the baseline visit was slightly higher in the SU than in the PC setting (7–10 days in PC and 15–30 days in the SU). Both groups consisted of predominantly middle-aged obese men with moderate-to-severe OSA. The PC group had a significantly higher baseline ESS score (with a difference of 1.25; table 1). In the PC group, 96% of patients were diagnosed using RP, and 4% of patients were diagnosed using PSG. In the SU group, 73% of patients were diagnosed using RP, and 27% of patients were diagnosed using PSG. Apnoea–Hypopnoea Index (AHI) was similarly computed independently of the sleep test used (RP or PSG). The median (IQR) AHI was 23.1 (26.8) events/h in the PC group and 21.8 (35.2) events/h in the SU group. The percentage of patients with severe OSA (AHI ≥30 events/h) was 33.3% in the PC group and 38.3% in the SU group. The percentage of patients who were treated with CPAP was 47.6% in the PC group and 41.4% in the SU group.
Baseline characteristics of the intention-to-treat population
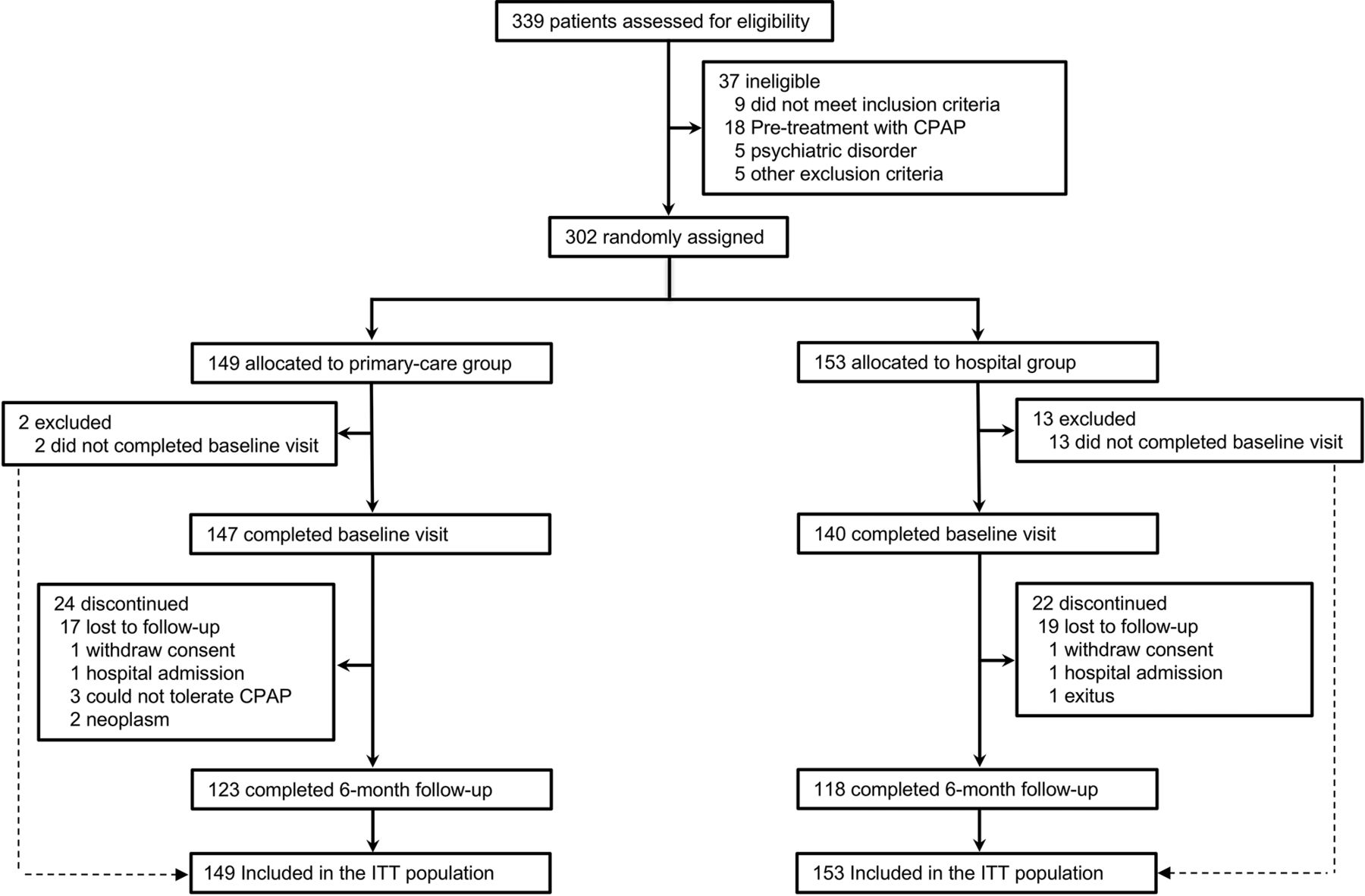
Study flowchart. ITT, intention-to-treat analysis.
Primary outcomes
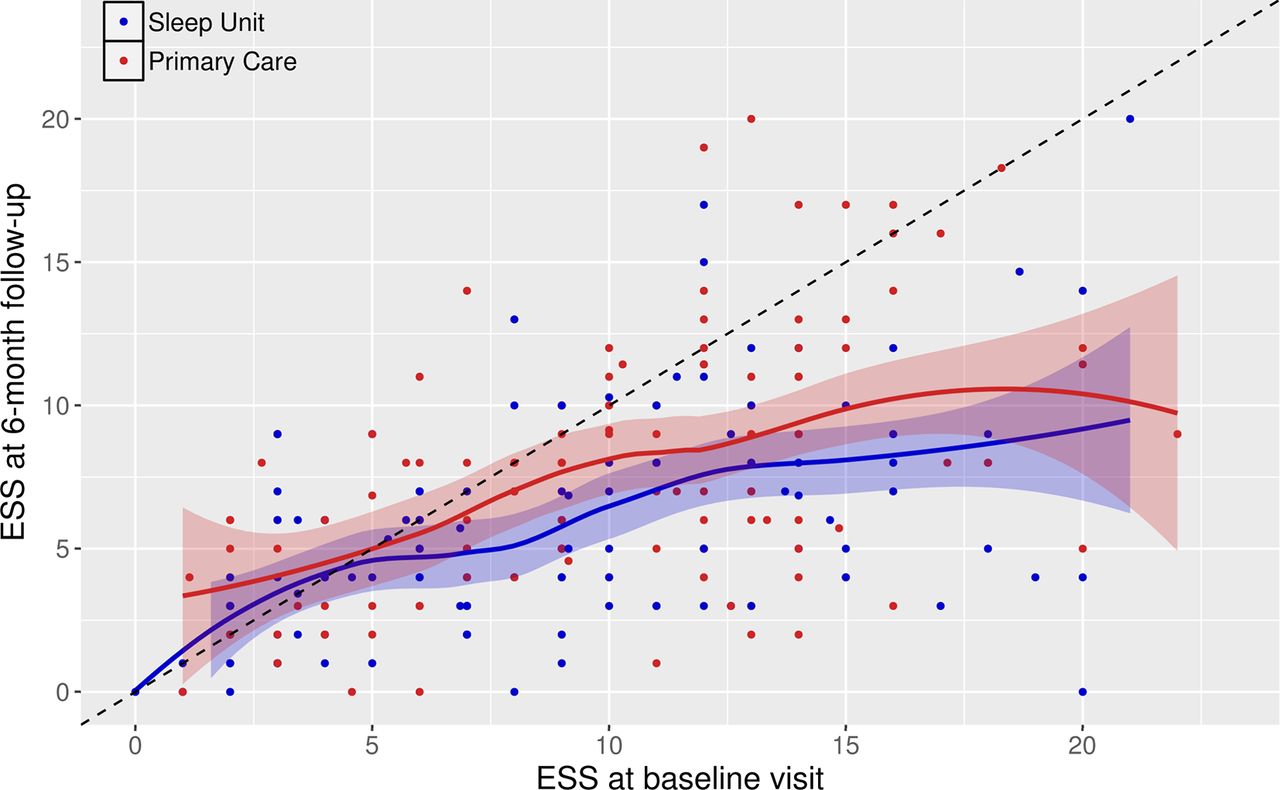
The mean ESS score of the PC group improved from 10.1 at baseline to 7.61 at 6 months, for an adjusted mean difference of −2.49 (95% CI −3.30 to −1.69; p<0.001). In the SU group, the mean ESS score improved from a baseline mean of 8.85 to 5.73 at 6 months, for a mean difference of −3.11 (95% CI −3.94 to −2.28; p<0.001). Figure 2 shows the evolution of each patient in terms of ESS score. After controlling for the baseline ESS score, the adjusted difference between groups for the mean change in the ESS score was −1.25 (lower bound of the one-sided 95% CI −1.88; p=0.025) for the ITT sample and −1.24 (lower bound of the one-sided 95% CI −1.98; p=0.046) for the PP sample. Both results support the non-inferiority of PC management because the lower bounds of the one-sided 95% CI for the analysis were greater than the prespecified non-inferiority margin of −2 points for the ESS score (table 2).
Analysis of primary outcomes measured at 6 months

Changes in Epworth Sleepiness Scale (ESS) scores among groups throughout the follow-up period. The dashed line indicates no change in ESS value during follow-up. The left side to the dashed line represents worsening of the patient in ESS and the right side represents improvement. The red colour represents the primary care patients, and the blue colour indicates the sleep unit patients.
Based on the HUI analysis, the 6-month utilities were similar between the PC and SU groups (0.813±0.033 for the PC group and 0.802±0.036 for the SU group; p=0.871). The change in effectiveness at 6 months (according to the HUI analysis) was similar between the PC and SU protocols (0.024±0.003 for the PC group and 0.033±0.031 for the SU group) with a adjusted difference between groups of −0.005 (95% CI −0.042 to 0.032; p=0.762). Thus, the estimated value of the incremental cost-effectiveness ratio is not interpretable due to the minimal differences between the two groups. The comparison of within-trial costs showed a median cost of €286 per randomised patient in the PC group and €844.14 in the SU group (difference between groups, €558.14). The cost per reduction of one ESS point was €114.85 and €271.42 for the PC arm and SU, respectively. The differences in cost were primarily related to the diagnostic methods used and the cost of care by the physician/nurse (see online supplementary etable 6). Based on the analysis of probabilistic sensitivity, which was represented in a cost-effectiveness plan (see figure 3), the PC setting was more cost-efficient than the SU setting. The variations in the group costs support the results showing that PC management was more cost-efficient than SU management (sensitivity analysis; see online supplementary etable 8). The same cost-effectiveness analysis was performed using the ESS scores, resulting in similar conclusions (see additional details in the online supplementary appendix).

{kind=link}
{kind=link}
{kind=link}
Plot of the cost-effectiveness of primary care (PC) versus sleep unit (SU) management. Results of 25 000 bootstrap replications of the cost and Health Utilities Index (HUI) differences between the PC and SU groups on the incremental cost-effectiveness plane.
Secondary outcomes
The secondary outcomes measured at baseline and the changes observed after 6 months of follow-up are shown in table 3. BP improved in both groups, and a non-significant difference was observed between the groups, −0.73 (−5.12 to 3.65) and −1.47 (−4.63 to 1.46) mm Hg for systolic and diastolic BPs, respectively. We did not observe changes in the BMIs in either group. Finally, non-relevant differences were found for patient satisfaction and CPAP compliance (table 3).
Analysis of secondary outcomes measured at 6 months
Discussion
In the present study, the PC model was not inferior to the standard SU model in terms of our primary outcome measure, the ESS score. In addition, no differences were observed between groups in the HUI change. Based on the demonstrated difference in costs between both models, it can be concluded that the comprehensive management of OSA in the PC setting is a cost-efficient and feasible alternative to the standard care management exclusively performed in specialised SUs. Regarding secondary outcomes, the patients who received follow-up care in the PC setting reported similar measures. A previous study performed in patients with high pre-test probabilities of having moderate-to-severe OSA13 evaluated the use of a simplified method for the initial management of OSA. After comparing this method with SU-based care, no differences in changes in the ESS scores or quality of life were found. Similarly, improvement in daytime function and adherence to CPAP in patients evaluated using a management pathway consisting of home testing with portable monitors were not clinically inferior to the results obtained in patients receiving standard in-laboratory PSG testing.29 Moreover, as shown in the study by Antic et al,22 compared with physician-directed care, a simplified nurse-led model of care produced non-inferior results, including changes in the ESS scores and CPAP compliance, in managing symptomatic moderate-to-severe OSA. Additionally, in the randomised controlled trial by Chai-Coetzer et al,11 the clinical efficacy of a simplified model of diagnosis and care in a PC unit was compared with that of specialist SUs, and the results showed that treatment under a PC model compared with a specialist model did not result in worse sleepiness scores among patients with high pre-test probability of OSA. Finally, as shown in a previous randomised controlled trial performed by our group, follow-up care for CPAP treatment under a PC model compared with a specialist model did not result in worse CPAP compliance among patients diagnosed with OSA.12
The present study has notable differences with respect to these previous studies that included (1) patients attending a PC visit due to suspected OSA or resistant hypertension (no high pre-test probability of having OSA), (2) the opportunity for the PC physician to decide on the method used to diagnose OSA (PSG or a simplified diagnostic method using RP) and the specific therapeutic interventions, and (3) the presentation of a realistic and cost-efficient comprehensive care model that is easily incorporated into routine clinical practice in a PC setting. Moreover, this new model for the comprehensive management of a patient with suspected OSA in a PC setting contributes to a significant financial and median savings of €558.14 per patient, with a non-clinically relevant and assumable loss of efficacy, based on a reduction in the ESS score of 1.25 points.
The present study has several strengths and limitations. The strengths include its design, which is closely associated with clinical practice; therefore, the findings are easily generalisable. Based on the findings of this study, a PC setting is appropriate for the clinical management of patients with sleep apnoea in a manner similar to the methods used for other chronic diseases, thereby achieving results equivalent to the results obtained in a specialised SU, but at a lower cost. Several limitations of the present study deserve comment. First, this study was conducted in a region of Catalonia in Spain, and the cost differences between the two settings may be different from the differences observed in other countries. Nevertheless, previous studies performed in other countries have shown cost savings similar to the results obtained in our study,11 12 and our sensitivity analysis confirmed these results (online supplementary etable 8). Moreover, when considered in the US context, the equivalent median costs per patient were estimated at US$396.18 in the PC group and US$1002.28 in the SU group (online supplementary etable 9). Importantly, it should be noted that the sleep study costs were the main contributor to the increased within-trial cost in the SU group. In the present study, we performed an additional analysis considering the same cost for sleep studies in the PC and SU settings, which showed that the management of a patient via PC generated a savings of €117.16. Second, 8 of the 11 participating PC centres had participated in a previous study by our group12 and had previously received specific training in managing patients with OSA before completing the new education programme. Therefore, there was no complete uniformity in the experience in the PC group with respect to education programmes. Third, the baseline ESS score was different between the groups, being higher in the PC group than in the SU group. The self-administered ESS is a validated questionnaire for assessing subjective daytime sleepiness. As with other subjective assessments, the results are dependent on characteristics of the patient and/or other external factors that could influence the patient’s perceptions and responses to this subjective questionnaire. Thus, previous studies have reported differences in subjective questionnaire responses between PC and tertiary referral units. Fink-Miller et al 30 showed that PC patients reported more severe pain than their counterparts at tertiary care facilities. However, in the present study, the estimated difference in the ESS score change between the groups was adjusted by the baseline value. Fourth, the mean baseline ESS score in the SU unit was relatively low and may have generated a ‘floor effect’ that allowed less room for improvement in this group. The primary goal of OSA treatment is to reduce EDS. Previous studies have identified the ESS score as the primary outcome of interest to compare the SU versus PC setting for OSA management with a consensus-based two-point improvement in ESS score.31 This study had the objective of evaluating the non-inferiority of efficacy of OSA management through PC from a pragmatic point of view, considering the inclusion of patients with suspected OSA, including all the conditions frequently associated with OSA (mainly clinical symptoms, snoring, observed apnoea and/or resistant hypertension). This real-life approximation of the recruitment of patients with suspected OSA also included patients with low ESS scores (ie, snoring without EDS or patients with resistant hypertension without EDS). The obtained mean ESS score at baseline in the SU group was similar to those obtained in previous studies.12 32 33 Despite the relatively low baseline ESS score, it is worth noting that 68.5% and 71% of the patients in the PC and SU groups, respectively, showed an ESS score decrease after 6 months of follow-up (figure 2). Fifth, AHI was similarly computed independently of the sleep test used (in the present study, 84.6% of sleep studies were performed with RP and 15.4% with PSG). This could lead to underestimation of the AHI in RP in relation to PSG and may generate misdiagnosis in patients diagnosed with RP. Nevertheless, a recent randomised controlled trial34 compared the long-term effectiveness of RP and PSG management protocols in a large population of patients with intermediate-to-high suspicion of OSA who were treated with or without CPAP. That study found that the effectiveness of the RP protocol (assessed by ESS) was not inferior to that of the PSG protocol.
Conclusions
The comprehensive management of OSA in a PC setting is a cost-efficient and feasible alternative to the standard care and management that are exclusively performed in specialised SUs. Based on the relevant existing literature that has explored the feasibility of PC management of OSA, the incorporation of PC settings as a feasible alternative for the management of patients with suspected OSA could be recommended.
Acknowledgments
The authors thank all the PC personnel involved in the study (Group of Translational Research in Respiratory Medicine, IRB Lleida, Spain) for their kind support.
References
Footnotes
NT and MST contributed equally.
Contributors Study design: MSdlT, FB. Data acquisition: NT, NN, AC, MCU, VS, IL, MML, AF, JC, LL, LV, MCJ, AJ, MG, LP, OM. Data analysis and interpretation: NT, MSdlT, NN, JDB, IDB, FB. Manuscript draft and revision for intellectual content and approval of the final version: NT, MSdlT, NN, JDB, IDB, AC, MCU, VS, IL, MML, AF, JC, LL, LV, MCJ, AJ, MG, AC, LP, OM, FB. Guarantor of the study: FB.
Funding Fondo de Investigación Sanitaria (PI13/02004) (Fondo Europeo de Desarrollo Regional (FEDER), Una manera de hacer Europa), the Spanish Respiratory Society (SEPAR) and ALLER.
Competing interests None declared.
Patient consent Not required.
Ethics approval The study protocol and consent documents were approved by the Ethical Committee for Clinical Research of the Hospital Arnau de Vilanova–Santa Maria (Lleida, Spain; registration no. CEIC1221).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The authors commit to making the relevant anonymised patient level data available on reasonable request.