Article Text

Abstract
Background Exposure to radiation and/or chemotherapy during cancer treatment can compromise respiratory function. We investigated the risk of long-term respiratory mortality among 5-year cancer survivors diagnosed before age 40 years using the British Childhood Cancer Survivor Study (BCCSS) and Teenage and Young Adult Cancer Survivor Study (TYACSS).
Methods The BCCSS comprises 34 489 cancer survivors diagnosed before 15 years from 1940 to 2006 in Great Britain. The TYACSS includes 200 945 cancer survivors diagnosed between 15 years and 39 years from 1971 to 2006 in England and Wales. Standardised mortality ratios and absolute excess risks were used.
Findings Overall, 164 and 1079 respiratory deaths were observed in the BCCSS and TYACSS cohorts respectively, which was 6.8 (95% CI 5.8 to 7.9) and 1.7 (95% CI 1.6 to 1.8) times that expected, but the risks varied substantially by type of respiratory death. Greatest excess numbers of deaths were experienced after central nervous system (CNS) tumours in the BCCSS and after lung cancer, leukaemia, head and neck cancer and CNS tumours in the TYACSS. The excess number of respiratory deaths increased with increasing attained age, with seven (95% CI 2.4 to 11.3) excess deaths observed among those aged 50+ years in the BCCSS and three (95% CI 1.4 to 4.2) excess deaths observed among those aged 60+ years in the TYACSS. It was reassuring to see a decline in the excess number of respiratory deaths among those diagnosed more recently in both cohorts.
Conclusions Prior to this study, there was almost nothing known about the risks of respiratory death after cancer diagnosed in young adulthood, and this study addresses this gap. These new findings will be useful for both survivors and those involved in their clinical management and follow-up.
- clinical epidemiology
- copd epidemiology
- paediatric interstitial lung disease
- pneumonia
This is an open access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
Key messages
What is the key question?
What are the long-term risks of respiratory-specific mortality among 5-year survivors of childhood, adolescent and young adult cancer?
What is the bottom line?
This large-scale population-based study provides evidence that such survivors are at an increased risk of respiratory death, with appreciable excesses observed among survivors of specific cancers and survivors aged over 50 years, although there is evidence of a reduction in the excess number of respiratory deaths among individuals diagnosed recently.
Why read on?
This article substantially advances the knowledge on respiratory mortality among childhood, adolescent and young adult cancer survivors by providing the most comprehensive analysis to date on respiratory mortality, which is useful for both survivors and those involved in their clinical follow-up.
Introduction
Survival after childhood, adolescent and young adult cancer has improved substantially over recent decades, with approximately 80% of those diagnosed now surviving at least 5 years.1 2 However, the curative treatments used to achieve such outcomes are associated with adverse health effects. One such adverse health effect concerns respiratory diseases (International Classification of Diseases (ICD) 10th revision: J00–J99) which, following circulatory diseases (ICD-10: I00–I99), account for the most non-neoplastic deaths among childhood cancer survivors.3 Previous research indicates that direct irradiation to the chest and lungs can cause developmental abnormalities of the thoracic cage, short-term treatment-induced lung disease presenting as pneumonitis or interstitial lung injury, and long-term damage manifesting as fibrosis.4 Furthermore, a number of chemotherapy drugs have been associated with respiratory late effects.4 5 Such respiratory morbidities can impact the quality of life of survivors5 and lead to premature death. As the number of childhood, adolescent and young adult cancer survivors is growing, with all having a substantial proportion of their expected lifespan remaining, it is crucial to investigate the risk of respiratory late effects in this population of survivors in order to identify vulnerable subgroups who may require closer clinical follow-up or intervention, as well as to improve our understanding of the pathogenesis of respiratory complications so that such late effects can be prevented in the future.
We assessed the long-term risks of respiratory-specific mortality among 5-year survivors of cancer diagnosed before the age of 40 years using the British Childhood Cancer Survivor Study (BCCSS) and Teenage and Young Adult Cancer Survivor Study (TYACSS). With over 235 000 survivors, more than 1200 observed respiratory deaths, and nearly 3.5 million person-years available, this study is by far the largest ever assembled to assess long-term respiratory mortality in survivors of childhood, adolescent and young adult cancers. The findings presented provide evidence for respiratory mortality risks overall, as well as the risks of specific types of respiratory death. The evidence produced will be useful for both survivors and those involved in clinical management and follow-up of survivors.
Methods
Study populations
This study uses two of the largest population-based cohorts of childhood, adolescent and young adult cancer survivors: the BCCSS6 and TYACSS.7 The BCCSS comprises 34 489 5-year survivors of childhood cancer diagnosed under the age of 15 years in Great Britain from 1940 to 2006. The cohort was identified using the National Registry of Childhood Tumors,8 and all first primary neoplasms (FPN) were classified using the International Classification of Childhood Cancer (online supplementary etable 1).9 The TYACSS includes 200 945 5-year survivors of adolescent and young adult cancers diagnosed between 1971 and 2006, in England and Wales, when aged between 15 years and 39 years. The cohort was established in collaboration with the Office for National Statistics and Welsh Cancer Registry. Adolescent and young adult FPNs were classified using the categories proposed by Birch et al, which were then slightly modified to produce finer groupings (online supplementary etable 2).10 11
Supplementary file 1
Death ascertainment
The BCCSS and TYACSS cohorts were linked to the National Death Registration systems in order to ascertain each survivor’s vital and emigration status. This linkage provided the death certificate and underlying cause of death, as coded using the relevant ICD at time of death. Respiratory deaths were determined by using the ‘diseases of the respiratory system’ chapters of the relevant ICD editions. ICD codes were further subcategorised into the following clinically relevant groups for analysis: pneumonia, chronic lower respiratory disease (excluding asthma), fibrosis, pneumonitis and other respiratory deaths (online supplementary etable 3). Follow-up for respiratory mortality commenced at 5-year survival and continued until the first occurrence of emigration, death or 28 February 2014.
Statistical analyses
To investigate the risk of respiratory mortality among survivors compared with that expected from the general population, standardised mortality ratios (SMRs) and absolute excess risks (AERs) were calculated using standard cohort techniques.12 The SMR was defined as the ratio of the observed over the expected number of respiratory deaths. The AER was defined as the observed minus the expected number of respiratory deaths divided by person-years at risk multiplied by 10 000; when reporting AERs, we often simply provide the excess, or extra, number of deaths without specifying the 10 000 person-years denominator. Expected numbers were calculated by multiplying the person-years at risk for each sex-specific, age-specific (5-year bands) and calendar year-specific (1-year bands) stratum by the corresponding respiratory mortality rate for the population of England and Wales and then summing across the strata.13 Likelihood ratio tests comparing multivariate Poisson regression models adjusting for the simultaneous effects of sex, FPN type, age at cancer diagnosis, treatment era and attained age were used to test for significant heterogeneity or a significant linear trend in the adjusted SMRs and AERs for each explanatory factor. In reporting, we focus on AERs because of their direct and clear interpretation as the excess number of deaths beyond that expected, indicating extent of adverse public health impact. All analyses were completed using Stata Corp, 2013 V.13.1, where the criterion for statistical significance was a two-sided P<0.05.
Role of the funding source
The funder had no role in this study. The lead and corresponding authors had full access to all the data in the study and had final responsibility of the decision to submit for publication.
Results
British Childhood Cancer Survivor Study
All respiratory deaths
The BCCSS cohort was followed up for a total of 620 758 person-years from 5-year survival. The mean follow-up from FPN diagnosis was 23.0 years (range: 5.0–73.7) and mean attained age at the end of current follow-up was 29.6 years (range: 5.5–85.6). Of the 4475 deaths observed, 164 (3.7%) were due to respiratory causes (table 1). Over half of the respiratory deaths were observed in survivors of central nervous system (CNS) tumours, including CNS primitive neuroectodermal tumours (PNET). However, when the proportion of deaths attributable to respiratory causes was assessed, germ cell tumour survivors had the highest percentage at nearly 11%.
Study characteristics of the British Childhood Cancer Survivor Study
Survivors of childhood cancer were 6.8 times (95% CI 5.8 to 7.9) more at risk of respiratory death than expected in the general population; this equated to 2.3 (95% CI 1.8 to 2.7) excess respiratory deaths (figure 1). Survivors of each FPN type with at least 5 observed deaths were found to be significantly more at risk of respiratory death than expected; the excess number of respiratory deaths exceeded 5 among survivors of CNS PNET and CNS tumours (excluding PNET) at 7.7 (95% CI 3.6 to 11.7) and 5.1 (95% CI 3.8 to 6.5), respectively. As attained age increased, the AERs increased (adjusted p trend=0.0127); at 5–19 years age, the AER was 1.7 (95% CI 0.3 to 3.1), while beyond 50 years age the AER was 6.8 (95% CI 2.4 to 11.3). Among those treated more recently, the number of excess respiratory deaths declined (adjusted p trend=0.0153); survivors diagnosed before 1970 and between 1990 and 2006 experienced 3.4 (95% CI 2.3 to 4.6) and 1.0 (95% CI 0.5 to 1.5) excess respiratory deaths, respectively.

SMRs and AERs per 10 000 person-years for all respiratory mortality in the British Childhood Cancer Survivor Study. P heterogeneity and p trend were calculated by using likelihood ratio tests within multivariable Poisson regression models that adjusted for sex, first primary neoplasm type, age at diagnosis, treatment era and attained age. Strata with less than five observed events should be interpreted with caution. AER, absolute excess risk; AML, acute myeloid leukaemia; CNS, central nervous system; E, expected; O, observed; PNETs, primitive neuroectodermal tumour; SMR, standardised mortality ratio.
Of the 164 respiratory deaths observed, there were 77 pneumonia, 18 pneumonitis, 15 fibrosis, 11 chronic lower respiratory disease and 43 other respiratory deaths (online supplementary etable 4). The corresponding SMRs were 8.2 (95% CI 6.5 to 10.2), 16.9 (95% CI 10.0 to 26.8), 13.8 (95% CI 7.7 to 22.8), 1.8 (95% CI 0.9 to 3.2) and 6.5 (95% CI 4.7 to 8.8), respectively, and the corresponding AERs were 1.1 (95% CI 0.8 to 1.4), 0.3 (95% CI 0.1 to 0.4), 0.2 (95% CI 0.1 to 0.3), 0.1 (95% CI 0.0 to 0.2) and 0.6 (95% CI 0.4 to 0.8). As nearly half of the respiratory deaths observed were due to pneumonia, further analyses were only undertaken for this specific group of deaths. However, it is worth noting that 13/18 (72.2%) of the pneumonitis deaths occurred in CNS tumours (excluding PNET) survivors, which equated to a 53.8-fold (95% CI 28.6 to 92.0) increased risk compared with that expected.
Pneumonia deaths
Survivors of CNS PNET, CNS tumours (excluding PNET) and germ cell tumours experienced the greatest excess numbers of pneumonia deaths at 5.2 (95% CI 1.9 to 8.5), 2.8 (95% CI 1.8 to 3.8) and 2.1 (95% CI 0.1 to 4.1), respectively (figure 2). With more recent treatment era, there was a decline in the excess number of pneumonia deaths observed (adjusted p trend <0.0001), where the AER decreased from 2.2 (95% CI 1.3 to 3.0) to 0.1 (95% CI −0.1 to 0.2) among those diagnosed before 1970 and between 1990 and 2006, respectively.

SMRs and AERs per 10 000 person-years for pneumonia mortality in the British Childhood Cancer Survivor Study. P heterogeneity and p trend were calculated by using likelihood ratio tests within multivariable Poisson regression models that adjusted for sex, first primary neoplasm type, age at diagnosis, treatment era and attained age. Strata with less than five observed events should be interpreted with caution. AER, absolute excess risk; AML, acute myeloid leukaemia; CNS, central nervous system; E, expected; O, observed; PNETs, primitive neuroectodermal tumours; SMR, standardised mortality ratio.
Teenage and Young Adult Cancer Survivor Study
All respiratory deaths
From 5-year survival, the TYACSS cohort was followed up for a total of 2 867 878 person-years. The mean follow-up from FPN diagnosis was 19.3 years (range: 5.0–43.2) and mean attained age at exit was 51.0 years (range: 20.3–82.7). Overall, 34 180 (17.0%) adolescent and young adult survivors had died; of these, 1079 (3.2%) were due to respiratory causes (table 2). The proportion of deaths attributable to respiratory causes was highest among lung cancer survivors at 10%, followed by head and neck cancer survivors and cervical cancer survivors at 6% each.
Study characteristics of the teenage and young adult cancer survivor study
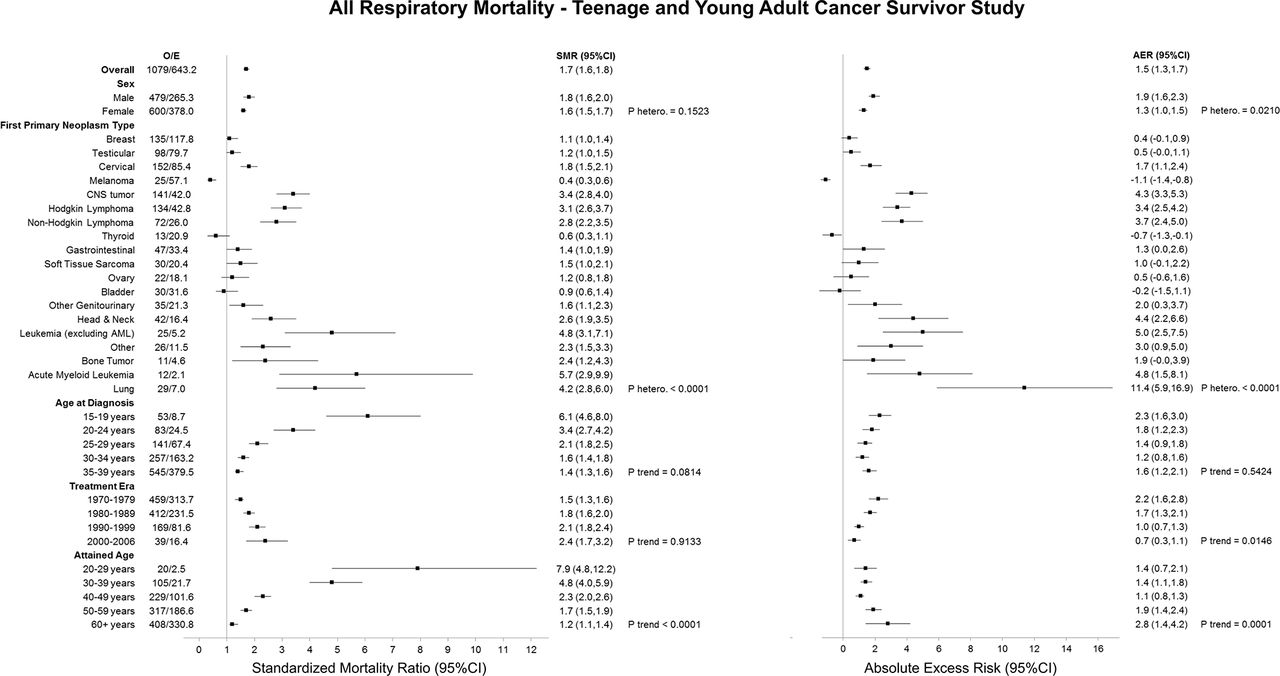
Overall, adolescent and young adult survivors were 70% (SMR: 1.7; 95% CI 1.6 to 1.8) more likely to die from a respiratory cause than expected from the general population, which equated to 1.5 (95% CI 1.3 to 1.7) excess respiratory deaths (figure 3). The excess number of respiratory deaths was significantly higher among males compared with females (adjusted p heterogeneity=0.0210). Survivors of lung, leukaemia (excluding acute myeloid leukaemia (AML)), head and neck cancer and CNS tumours experienced the greatest excess number of respiratory deaths at 11.4 (95% CI 5.9 to 16.9), 5.0 (95% CI 2.5 to 7.5), 4.8 (95% CI 1.5 to 8.1), 4.4 (95% CI 2.2 to 6.6) and 4.3 (95% CI 3.3 to 5.3), respectively. As attained age increased. the AERs increased from 1.4 (95% CI 0.7 to 2.1) among those aged 20–29 years to 2.8 (95% CI 1.4 to 4.2) among those aged 60+ years (adjusted p trend=0.0001). A decline in the excess number of respiratory deaths with more recent treatment era was observed (adjusted p trend=0.0146), where the AER decreased from 2.2 (95% CI 1.6 to 2.8) to 0.7 (95% CI 0.3 to 1.1) in those treated in the 1970s and 2000s, respectively.

SMRs and AERs per 10 000 person-years for all respiratory mortality in the Teenage and Young Adult Cancer Survivor Study. P heterogeneity and p trend were calculated by using likelihood ratio tests within multivariable Poisson regression models that adjusted for sex, first primary neoplasm type, age at diagnosis, treatment era and attained age. Strata with less than five observed events should be interpreted with caution. AER, absolute excess risk; AML, acute myeloid leukaemia; CNS, central nervous system; E, expected; O, observed; PNETs, primitive neuroectodermal tumour; SMR, standardised mortality ratio.
When the 1079 respiratory deaths were assessed by specific respiratory causes of death, there were 395 pneumonia, 393 chronic lower respiratory disease, 74 fibrosis, 49 pneumonitis and 168 other respiratory deaths (figure 4, table 3). Although adolescent and young adult survivors were at a statistically significant increased risk of death from each specific type of respiratory death, the SMR was greatest for pneumonitis and pneumonia deaths at 2.2 (95% CI 1.6 to 2.9) and 2.1 (95% CI 1.9 to 2.3), respectively.
SMRs and AERs per 10 000 person-years for chronic lower respiratory mortality, fibrosis mortality, pneumonitis mortality and other respiratory mortality by potential explanatory factors, for the Teenage and Young Adult Cancer Survivor Study†

{kind=link}
{kind=link}
{kind=link}
{kind=link}
SMRs and AERs per 10 000 person-years for pneumonia mortality in the Teenage and Young Adult Cancer Survivor Study. P heterogeneity and p trend were calculated by using likelihood ratio tests within multivariable Poisson regression models that adjusted for sex, first primary neoplasm type, age at diagnosis, treatment era and attained age. Strata with less than five observed events should be interpreted with caution. AER, absolute excess risk; AML, acute myeloid leukaemia; CNS, central nervous system; E, expected; O, observed; PNETs, primitive neuroectodermal tumour; SMR, standardised mortality ratio
Pneumonia deaths
Male survivors of adolescent and young adult cancers experienced more excess pneumonia mortality compared with females (adjusted p heterogeneity=0.0061) (figure 4). Survivors of lung cancer, CNS tumours and head and neck cancers experienced the greatest excess number of pneumonia deaths at 3.6 (95% CI 0.6 to 6.7), 2.5 (95% CI 1.7 to 3.2) and 2.1 (95% CI 0.7 to 3.5), respectively. The excess number of pneumonia deaths increased as age at diagnosis increased (adjusted p trend=0.0312) and declined among those treated more recently (adjusted p trend=0.0083).
Chronic lower respiratory disease deaths
Survivors of lung cancer experienced the greatest excess number of deaths at 6.6 (95% CI 2.5 to 10.6) (table 3). AERs increased with attained age from 0.1 (95% CI −0.1 to 0.4) to 1.3 (95% CI 0.2 to 2.3) among those aged 20–29 years and 60+ years, respectively (adjusted p trend <0.0001). Survivors diagnosed more recently experienced less excess chronic lower respiratory disease deaths (adjusted p trend=0.0024).
Fibrosis and pneumonitis deaths
With regards to fibrosis death, female survivors were found to experience a greater excess number of deaths than male survivors (adjusted p heterogeneity=0.0040) (table 3). For both fibrosis and pneumonitis deaths, the AERs were consistently less than one after each specific FPN type, except for fibrosis deaths among AML survivors, though only three deaths were observed. Finally, the AER increased with increasing attained age for pneumonitis deaths (adjusted p trend=0.0078).
Discussion
Compared with the previous literature, our study is by far the largest to assess respiratory mortality among 5-year survivors of childhood, adolescent and young adult cancers, reporting for the first time results for specific types of respiratory death and risks beyond 50 years of age. There have been two previous studies of survivors of cancer diagnosed in individuals aged at least 20 years—one included 11 417 5-year survivors and 29 respiratory deaths,14 the other included 1248 5-year survivors and 7 respiratory deaths,15 and we included 188 697 5-year survivors and 1079 respiratory deaths. As a result of these large numbers, and our study’s population-based design and long period of follow-up, we provide the most comprehensive investigation of risks and risk factors for respiratory mortality among childhood, adolescent and young adult cancer survivors to date.
Our principal new findings include the following. Among survivors of childhood cancer, the greatest excess numbers of respiratory deaths were experienced after PNETs of the CNS and other CNS tumours at 7.7 and 5.1 extra, respectively. Among survivors of adolescent and young adult cancer, the greatest excess number of respiratory deaths was experienced after lung cancer, leukaemia (excluding AML), AML, head and neck and CNS tumours at 11.4, 5.0, 4.8, 4.4 and 4.3 extra, respectively. The excess number of respiratory deaths increased with increasing attained age, reaching 6.8 excess deaths among those aged 50+ years in the BCCSS, and reaching 2.8 excess deaths among those aged 60+ years in the TYACSS cohort. It was reassuring that the excess number of respiratory deaths declined among those treated more recently in both cohorts, and in each cohort, the AER declined to about one excess respiratory death among those treated most recently.
Our findings in relation to previous research
In this study, childhood cancer survivors were seven times more at risk of respiratory death than that expected from the general population, while adolescent and young adult cancer survivors were two times more at risk; these findings broadly correspond with previous reports.14–16 However, when assessed in more detail, the excess risks for specific types of respiratory death varied considerably. Significant excesses were observed for pneumonia, fibrosis, pneumonitis and other respiratory deaths for childhood cancer survivors, with the SMRs ranging from 7-fold to 17-fold that expected. Similarly, risks varied among adolescent and young adult cancer survivors depending on the specific type of respiratory death, although to a lesser extent than that observed among childhood cancer survivors. The fact that the SMR among childhood cancer survivors was higher than the corresponding SMR in adolescents and young adults for each type of respiratory death assessed could relate to the increased vulnerability of children to radiotherapy, chemotherapy and surgery side effects as the child is still growing and developing,17 while adolescents and young adults generally tolerate acute side effects of therapy relatively well.18
In regards to risk factors, the greatest excess numbers of respiratory deaths among survivors of childhood cancer were experienced after CNS PNET and other CNS tumours, and after lung cancer, leukaemia (excluding AML), AML, head and neck and CNS tumours among survivors of adolescent and young adult cancer. The large increased risks observed in these specific FPN types could relate to previous cancer treatment.5 19 For example, craniospinal irradiation and the use of nitrosureas in CNS survivors can induce pneumonitis and late restrictive lung disease,20 while restrictive and obstructive lung disease can develop as a result of the use craniospinal irradiation, total body irradiation or high-dose busulphan in bone marrow transplantation for leukaemia survivors.19 21 Other clinical correlations between therapeutic agents and respiratory late effects are as follows: (1) busulfan, carmustine or lomustine and the development of pulmonary fibrosis; (2) bleomycin and the development of interstitial pneumonitis, pulmonary fibrosis or acute respiratory distress syndrome; (3) irradiation to the axilla, chest, extended mantle, mantle, mediastinal, mini-mantle or whole lung, subtotal lymphoid irradiation, total body irradiation or total lymphoid irradiation and the development of pulmonary fibrosis, interstitial pneumonitis, restrictive lung disease or obstructive lung disease; (4) haematopoietic cell transplant with any history of graft-versus-host disease and the development of pulmonary toxicity, bronchiolitis obliterans, chronic bronchitis or bronchiectasis; and (5) thoracic surgery and the development of pulmonary dysfunction.22 However, there may be non-treatment factors that contribute to respiratory mortality. This is particularly apparent for chronic lower respiratory disease deaths in lung cancer survivors, which accounted for 55% (16/29) of the observed excess respiratory deaths in this FPN type, as it is hypothesised that these diseases share underlying host susceptibility factors.23 Similarly, the fact that over 60% (46/77) of the pneumonia deaths in childhood cancer survivors occurred in survivors of CNS tumours or CNS PNET suggests an increased risk of aspiration pneumonia, which may be linked to a weaker cough reflex due to chronic neurological deficits.24
Another interesting finding from our study is that there were an increasing number of excess respiratory deaths as survivors aged. These findings may relate to the fact that respiratory death is among the more common causes of death among mature members of the general population. Consequently, because the expected number of deaths is substantial, even a modest multiplicative excess risk will result in substantial excess numbers of death.
Nonetheless, it was reassuring that the excess number of respiratory deaths declined among those treated more recently in both cohorts. Such declines could be due to changes in cancer treatments, with the newer treatment regimens designed to reduce radiotherapy and chemotherapy exposures while maintaining long-term, disease-free survival3 25; moving forward, continued improvement is a reasonable expectation, especially with the use of proton beam therapy, which will further limit the dose of radiotherapy scatter to the lungs. Other potential contributors include the increased surveillance of late effects through regular follow-up and screening, as well as increased supportive care with improved antiviral and antifungal agents that may limit the severity of lung infections and complications compared with previously.3 25 26
Clinical implications
Although the findings presented in this study provide reliable (based on large numbers) and unbiased (population-based design) evidence on respiratory mortality risks, it is important that these results also inform clinicians and the vulnerable subgroups of survivors identified about the risks of respiratory morbidity. At-risk survivors and survivors with reduced lung reserve/function or abnormal/damaged lung tissues from cancer treatment should be monitored for chronic cough or dyspnoea through yearly pulmonary exams18 22 and should be aware of their susceptibility to further insults from recurrent respiratory infections (eg, pneumonia), lifestyle factors (eg, smoking27 28 or occupational exposure to toxic fumes/substances29) and other medical interventions (eg, exposure to high oxygen concentration with anaesthesia30–32); such subsequent insults can lead to further significant deterioration in lung function and reserve, respiratory failure and death. Furthermore, pneumococcal vaccination should be considered an important intervention for childhood, adolescent and young adult cancer survivors as pneumonia was the most common form of respiratory death in all groups, with substantial excess risks observed compared with that expected; although influenza-related deaths were observed less frequently in this study, influenza may act as a precursor to more serious respiratory conditions like pneumonia, and thus influenza vaccination may also be a useful preventative strategy for at-risk survivors. Finally, as the risks of respiratory mortality varied depending on the age at diagnosis of the survivor and the type of death being investigated, clinical follow-up guidelines should be refined in order to provide more accurate suggestions for survivors depending on whether they are a childhood, adolescent or young adult survivor, while interventions relating to specific respiratory complications should be developed.
Limitations
The first limitation of our study is that we only included individuals who survived at least 5 years after their cancer diagnosis, and thus the risks presented in this study are not representative of the risks for childhood, adolescent and young adult cancer survivors overall. Additionally, our calculations of SMRs and AERs are likely an underestimation of the multiplicative and additive excesses as competing causes of death are more common in our study population than in the general population33; as there is no accurate way to adjust for this bias,33 we acknowledge that our findings are likely to be conservative. Another limitation is that our study faced data sparsity for some stratifications; despite this being the largest study of respiratory mortality among such survivors, the outcome in question remains rare and thus our results with less than five observed events should be interpreted with caution. Furthermore, due to the fact that we determined respiratory deaths based on the underlying cause of death coded on the death certificate, there is possibly misclassification in our data as the underlying cause of death has imperfect accuracy.34–36 This study also lacked detailed treatment information, which prevented any examination of dose response patterns or treatment interactions. Information was also not available on lifestyle factors, making it impossible to assess the relative importance of smoking status, occupational hazards and other environmental factors. Finally, our findings suggest a significant increase in excess respiratory deaths as age increases. Although these findings provide important information for current survivors aged at least 50 years, it will be important to reassess our findings to see whether the risks remain consistent as younger survivors reach this age milestone since the cancer profile of 5 year survivors and treatment have changed over time. Similarly, it will be important to reinvestigate temporal trends in late respiratory mortality risks with additional follow-up in order to determine whether those most recently diagnosed remain with decreased risks.
Conclusions
This large-scale, population-based study provides evidence that survivors of childhood, adolescent and young adult cancers are at an increased risk of respiratory death, compared with that expected, both overall and for specific types of respiratory death. Although we report appreciable excess risks for respiratory death among specific FPN types and survivors aged over 50 years, there is evidence of a reduction in the excess number of respiratory deaths among individuals more recently diagnosed. These findings substantially advance the current knowledge on respiratory late effects among childhood, adolescent and young adult cancer survivors and will be useful for both survivors and those involved in their clinical management and follow-up.
Acknowledgments
The British Childhood Cancer Survivor Study (BCCSS) benefits from the contributions of the officers, centres and individual members of the Children’s Cancer and Leukaemia Group and the Regional Paediatric Cancer Registries. The BCCSS acknowledges the collaboration of the Office for National Statistics, the National Records of Scotland, the Welsh Cancer Intelligence and Surveillance Unit, the Health & Social Care Information Centre, the National Cancer Intelligence Network and Public Health England. The BCCSS would not have been possible without the support of our funders: Cancer Research UK and the European Commission to whom we offer our profound thanks. Finally, thanks to all BCCSS staff who have given many years of dedicated work to bring the BCCSS to fruition. The Teenage and Young Adult Cancer Survivor Study (TYACSS) would not have been possible without funding to the University of Birmingham from: Cancer Research UK and the National Institute for Health Research to whom we offer our profound thanks. The TYACSS acknowledges the collaboration of the Office for National Statistics, the Welsh Cancer Intelligence and Surveillance Unit and NHS-Digital. The TYACSS also acknowledges the following collaborators: Professor Sarah Darby, University of Oxford; Dr Angela Edgar, Royal Hospital for Sick Children, Edinburgh; Dr Richard Feltbower, University of Leeds; Dr Lorna Anne Fern, University College London; Dr Diana Greenfield, The University of Sheffield; Dr Tony Moran, North West Cancer Intelligence Service; Professor John Radford, University of Manchester; Dr Peter Rose, University of Oxford; Dr Helen Alexandra Spoudeas, University College London Hospitals NHS Foundation Trust; Dr William Hamish Wallace, Royal Hospital for Sick Children, Edinburgh; and Professor Jeremy Whelan, University College London Hospitals NHS Foundation Trust London. Finally, we are particularly thankful to the National Cancer Research Institute – Teenage and Young Adult – Clinical Studies Group.
References
Footnotes
Contributors Study design: MMF and MMH. Data collection: MMF, MMH, DLW, JSK, CJB, KEH, RCR and CF. Data analysis and interpretation: MMF, CJB, KEH and RCR. Drafting of the article: MMF and MMH. Critical revision: all authors. Final decision to submit: MMF and MMH.
Funding This work was supported by grant number C386/A10422 from Cancer Research UK and PanCareSurFup, which was funded by the European Commission 7th Framework Programme. Some of the work completed in this manuscript was undertaken while MMF was a postdoctoral fellow at the International Agency for Research on Cancer, which was partially funded by the European Commission’s 7th Framework Programme Marie Curie Actions-People-COFUND. No funder had a role in the study design, collection/analysis/interpretation of the data, writing of the report or in the decision to submit the article for publication.
Disclaimer The views expressed in this publication are those of the authors and not necessarily represent those of the funders or collaborators.
Competing interests None declared.
Patient consent Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
Ethics approval The National Research Ethics Committee and Confidentiality Advisory Group gave national ethical and legal consents for the BCCSS and TYACSS cohorts to proceed.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The data are not publicly available due to them containing semi-identifiable information that could compromise research participant privacy. Nonetheless, additional summary tables of count data or person-years are available from the corresponding author upon request.
Collaborators The British Childhood Cancer Survivor Study (BCCSS) is a national collaborative undertaking guided by a steering group that comprises Douglas Easton (chair), Michael Hawkins, Helen Jenkinson, Meriel Jenney, Raoul Reulen, Kathryn Pritchard-Jones, Elaine Sugden, Charles Stiller, Andrew Toogood and Hamish Wallace.