Article Text

Abstract
Background Standardised home-based pulmonary rehabilitation (PR) programmes offer an alternative model to centre-based supervised PR for which uptake is currently poor. We determined if a structured home-based unsupervised PR programme was non-inferior to supervised centre-based PR for participants with COPD.
Methods A total of 287 participants with COPD who were referred to PR (187 male, mean (SD) age 68 (8.86) years, FEV1% predicted 48.34 (17.92)) were recruited. They were randomised to either centre-based PR or a structured unsupervised home-based PR programme including a hospital visit with a healthcare professional trained in motivational interviewing, a self-management manual and two telephone calls. Fifty-eight (20%) withdrew from the centre-based group and 51 (18%) from the home group. The primary outcome was dyspnoea domain in the chronic respiratory disease questionnaire (Chronic Respiratory Questionnaire Self-Report; CRQ-SR) at 7 weeks. Measures were taken blinded. We undertook a modified intention-to-treat (mITT) complete case analysis, comparing groups according to original random allocation and with complete data at follow-up. The non-inferiority margin was 0.5 units.
Results There was evidence of significant gains in CRQ-dyspnoea at 7 weeks in both home and centre-based groups. There was inconclusive evidence that home-based PR was non-inferior to PR in dyspnoea (mean group difference, mITT: −0.24, 95% CI −0.61 to 0.12, p=0.18), favouring the centre group at 7 weeks.
Conclusions The standardised home-based programme provides benefits in dyspnoea. Further evidence is needed to definitively determine if the health benefits of the standardised home-based programme are non-inferior or equivalent to supervised centre-based rehabilitation.
Trial registration number ISRCTN81189044.
- pulmonary rehabilitation
- exercise
Statistics from Altmetric.com
Key messages
What is the key question?
Can a structured home-based unsupervised pulmonary rehabilitation (PR) programme of activity, coping and education for COPD be considered non-inferior to centre-based PR?
What is the bottom line?
The home-based programme achieved improvements in dyspnoea and exercise endurance capacity to a similar level to conventional supervised PR. However, non-inferiority remains inconclusive.
Why read on?
This study demonstrates that a structured home-based PR programme can provide some health improvements and may provide an alternative for those unable to attend centre-based PR.
Introduction
Pulmonary rehabilitation (PR) is a highly effective intervention for individuals with COPD and other chronic respiratory diseases. International guidance suggests that the programme should be a package of supervised exercise and education over a minimum of 6 weeks.1 Over the years the format of rehabilitation has altered very little. The content and formats of rehabilitation have been extensively investigated but alternative modes of delivery have been poorly reported.2 Maltais et al 3 reported that home-based exercise training was equivalent to a centre-based programme but this programme was supplemented by an initial 4-week centre-based education programme. Although the data suggested that home training was possible (with the provision of an exercise bike), the programme did require regular attendance at a rehabilitation centre. There have been small-scale studies that have looked at alternative forms of home-based rehabilitation but the design and sample size has not been adequate for a firm recommendation to be made.4 5 A more recent trial6 demonstrated that a weekly monitored home programme was equivalent to centre-based PR, however included a home visit by a physiotherapist and weekly telephone calls including personalised educational content. There is a lack of evidence for a standardised and unsupervised rehabilitation programme that has no home visits by a physiotherapist or intensive monitoring. A current research priorities document acknowledged this slow progress and proposed that alternative modes of delivery be investigated.7
Developing and testing an acceptable alternative to centre-based supervised rehabilitation would seem reasonable to increase the scope and choice of intervention. Furthermore, it may be a viable alternative for a number of people who are either unwilling or unable to attend a supervised programme.8 Many centres face challenges in meeting the demand and an alternative approach may help alleviate capacity issues.9
We have recently reported the effectiveness of a supported, but unsupervised home-based PR programme that was facilitated by a standardised manual that participants worked through (SPACE for COPD—a Self-management Programme of Activity Coping and Education10). Compared with control subjects we observed important changes in health-related quality of life (self-report dyspnoea domain on the Chronic Respiratory Questionnaire (CRQ-SR) mean change at 6 weeks 0.71 units, 95% CI 0.45 to 1.00, p=0.049) and exercise capacity (endurance shuttle walk test (ESWT) mean change at 6 weeks 209.7 s, 95% CI 122.3 to 297.1, p=0.006). These are two important outcomes that define the success of a conventional rehabilitation programme. We were therefore interested to examine whether the use of this home-based programme would provoke similar improvements to those in supervised PR. The use of a home-based approach supported by a standardised manual already exists for cardiac rehabilitation.11 It would seem that a comparison of structure and standardised home-based rehabilitation with centre-based PR would be a valuable addition.
Therefore, the aim of this study was to compare the home-based programme supported by the SPACE for COPD manual with conventional supervised centre-based PR. We hypothesised that this novel approach to deliver a home-based programme would not result in an inferior outcome at 7 weeks compared with supervised rehabilitation at 7 weeks. The primary outcome of the study was a change in dyspnoea at 7 weeks, measured by the CRQ-SR.12 Secondary aims were to explore the impact of the home programme in comparison to other measures of health-related quality of life, exercise capacity and psychological status at 7 weeks and 6 months.
Methods
We conducted an assessor-blinded, non-inferiority, randomised controlled trial comparing centre-based PR with a home-based programme supported with the SPACE for COPD manual with the primary endpoint at 7 weeks, and follow-up at 6 months. The study took place between November 2007 and July 2012. All participants gave written informed consent, and ethical approval for the study was granted by Leicestershire Northamptonshire and Rutland Regional Ethics Committee, reference 07/Q2501/6.
Subjects
Participants with COPD and Medical Research Council (MRC) score of 2–5 were recruited from those referred to PR at Glenfield Hospital and Leicester General Hospital, UK. Exclusion criteria included those who would normally prohibit access to PR such as lower limb disability and other unstable comorbid conditions. Participants who had completed PR in the previous 12 months were also excluded. Participants were required to have a proficient level of English.
Study design
The study was designed to show non-inferiority of a home-based rehabilitation programme as compared with a standard centre-based programme. The primary outcome was the self-report dyspnoea component of the CRQ-SR at 7 weeks, this was chosen because of its clinical relevance and its potential to show differences between the two groups. Secondary endpoints included measures of exercise tolerance, self-efficacy, anxiety and depression.
Recruitment and randomisation
Participants were recruited at their referral appointment to PR and all baseline measures were taken as part of the usual referral process. Participants interested in the study were subsequently contacted and a consent appointment arranged. Randomisation was completed using a random permuted blocks method with a 1:1 allocation ratio and sealed opaque envelopes. Randomisation was completed by a researcher not involved in the study.
Intervention
Participants randomised to the PR group completed the usual centre-based programme of twice weekly hospital-based supervised exercise and education programme over 7 weeks, as previously described.13 Participants randomised to the home-based group had an initial introductory session at the hospital led by a healthcare professional trained in motivational interviewing, instructing them how to use the manual to facilitate their home exercise programme.14 Participants in this group received two standardised telephone calls during the 7 weeks to assess their progress, support and motivate the participant to continue and to answer any questions. It was anticipated that participants would take 7 weeks to progress through the SPACE for COPD manual. However, the manual was theirs to keep and could support lifelong lifestyle changes. Details of the SPACE for COPD manual have been previously been reported.10 14 Both interventions were progressive and based on a daily walking programme with speed and initial duration determined by their performance in the incremental shuttle walk test (ISWT) and ESWT at their baseline assessment. Participants were advised to increase the duration of their walk each day. Resistance exercises covered the major muscle groups and were completed three times a week. A detailed description of both interventions is available in the online supplementary file 1.
Supplementary file 1
Outcome measures
Outcome measures were completed at baseline, 7 weeks and 6 months post intervention to understand the durability of the intervention. Outcome measures taken at 7 weeks and 6 months were conducted by a member of staff blinded to the allocation of the participants. Participants were instructed not to identify group allocation. If assessment appointments were missed, we attempted to reschedule on two further occasions. If they did not attend, these participants were then withdrawn from the study. All participants completed the outcome measures relating to health status and exercise performance (unless stated).
The primary outcome for this paper is the CRQ-SR at 7 weeks, although we have included 6-month findings. Our ISRCTN (International Standard Randomised Controlled Trial Number) previously stated that our primary outcome was the dyspnoea domain of the CRQ-SR12 at 7 weeks and 6 months. This was inaccurate, it is unusual to have a primary outcome at two time points. A higher score for the CRQ-SR indicates less impairment to quality of life. Secondary outcomes were the fatigue, emotional functioning and mastery domains of the CRQ-SR, and anxiety and depression as measured by the Hospital Anxiety and Depression Scale (HADS15), self-efficacy by the Pulmonary Rehabilitation Adapted Index of Self-Efficacy (PRAISE16) and the ISWT and ESWT.17 18
Sample size
For the primary outcome measure, a difference of 0.5 has been recognised as the minimum clinically important difference (MCID19), with a common SD of 1.1.13 Using these values in the sample size calculation to assess non-inferiority, with an alpha level of 0.025, and a two-sided test with 90% power, the required sample size was 314. Based on an attrition rate of 15% typically seen in the hospital rehabilitation group, 320 participants per group were targeted for recruitment. As it took longer to recruit and the dropout rate experienced was higher than anticipated we reduced the power to 80%. This resulted in a lower participant sample size of 177 required. We continued to recruit until sample size was achieved.
Data analysis
We analysed and reported primary and secondary outcomes following CONSORT (Consolidated Standards of Reporting Trials) guidelines for non-inferiority and equivalence trials.20 In our primary analysis, we compared primary and secondary outcomes between groups at post randomisation using linear regression models adjusted for baseline outcomes. We undertook modified intention-to-treat (mITT) complete case analysis and per protocol (PP) analysis, given that security of inference depends on both PP and mITT analysis demonstrating non-inferiority.20 Our mITT population comprises all participants according to and included in random allocation and with complete data. We defined the PP population as participants meeting the mITT definition and attending the final outcome assessment.
We accepted non-inferiority of home-based to centre-based PR (in a 0.025 level test) if the lower boundary of the two-sided 95% CI (equivalent to the upper bound of one-sided 97.5% CI) was within the non-inferiority margin of the MCID of 0.5 units for each of the four CRQ domains,19 1.5 units for the HADS,1548 m for the ISWT21 and 186 s for the ESWT.22 We checked for non-inferiority of the primary and secondary outcomes at the 6-month point using the same approach.
We undertook three groups of secondary analysis. First, we compared groups at follow-up, at 6 months as for primary analysis and checked for non-inferiority using the same approach as described above. Second, we assessed the likely effect of missing data using multiple imputation models. We did imputation by treatment group using chained equations to create 10 complete data sets under the assumption that data were missing at random. Twenty-two imputation models included covariates as defined for the primary model. After analysis, we combined the effect estimates from the imputed data sets using Rubin’s rule.23 Analysis was undertaken using STATA V.14.1.
Results
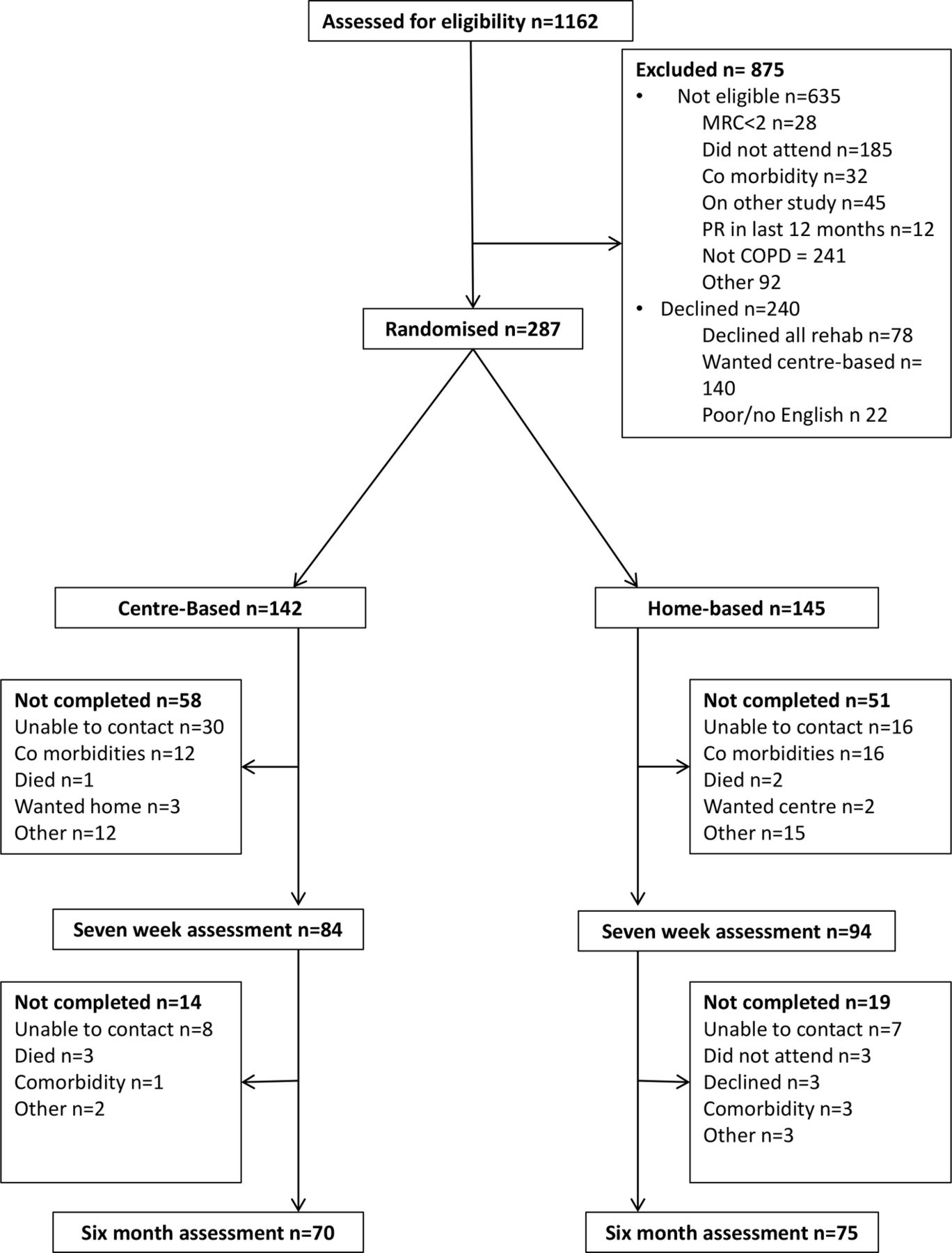
The flow of participants through the trial is summarised in figure 1. A total of 287 participants were recruited and randomised to the study, 142 to centre-based PR and 145 to home-based PR (table 1). There were patients with missing data from the baseline appointment. Missing data from questionnaires were due to non-completion of the form.
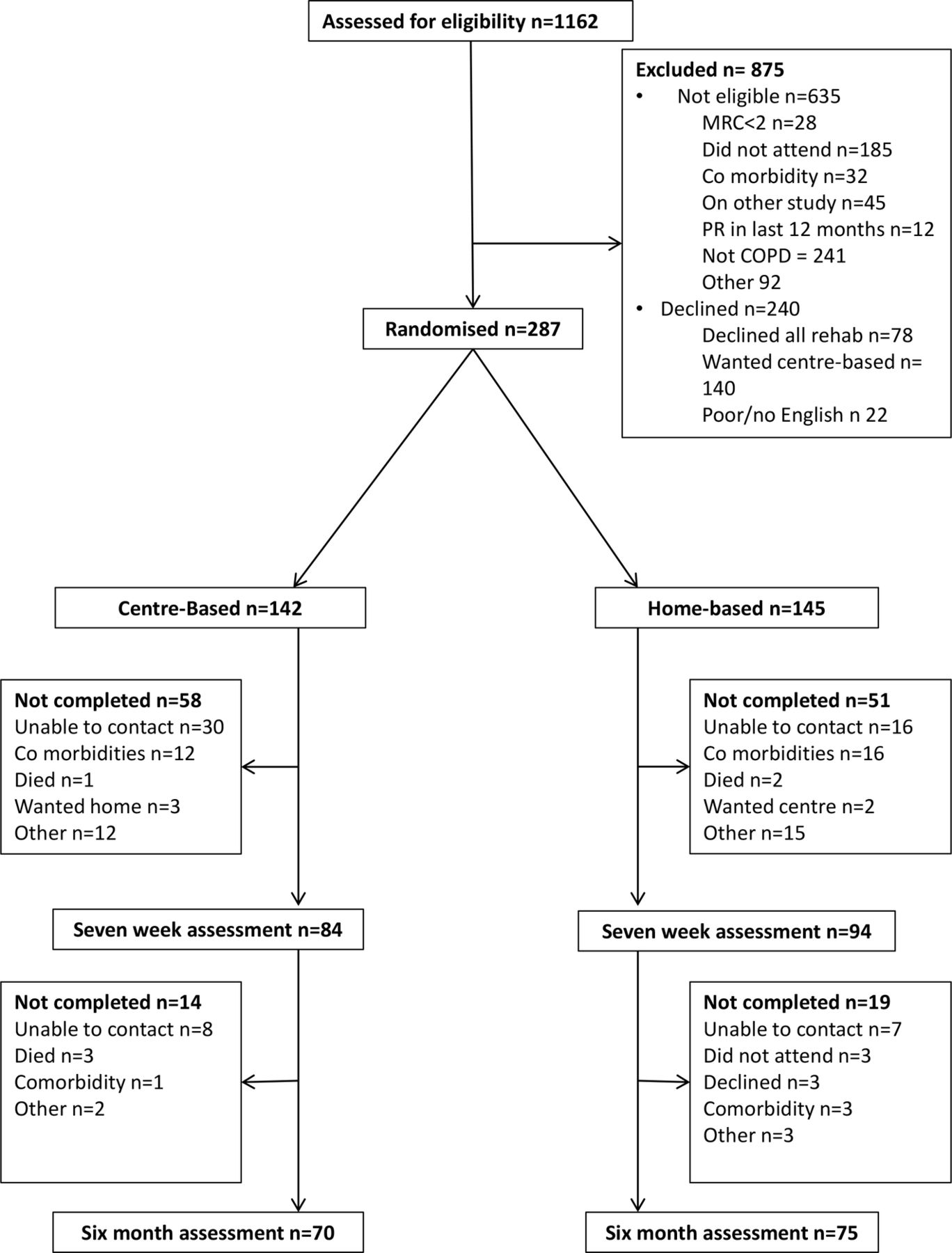
Consolidated Standards of Reporting Trials flow diagram of participation. MRC, Medical Research Council; PR, pulmonary rehabilitation.
Baseline characteristics and demographics
A total of 109 participants withdrew from the study. Fifty-eight people (41%) did not complete the 7-week assessment in the centre-based group and 51 people (35%) did not complete the 7-week assessment in the home-based group. Reasons for dropout are listed in figure 1. There was no evidence of substantive differences in baseline characteristics of those who did or did not complete the 7-week assessment (see online supplementary file 1).
Primary outcome
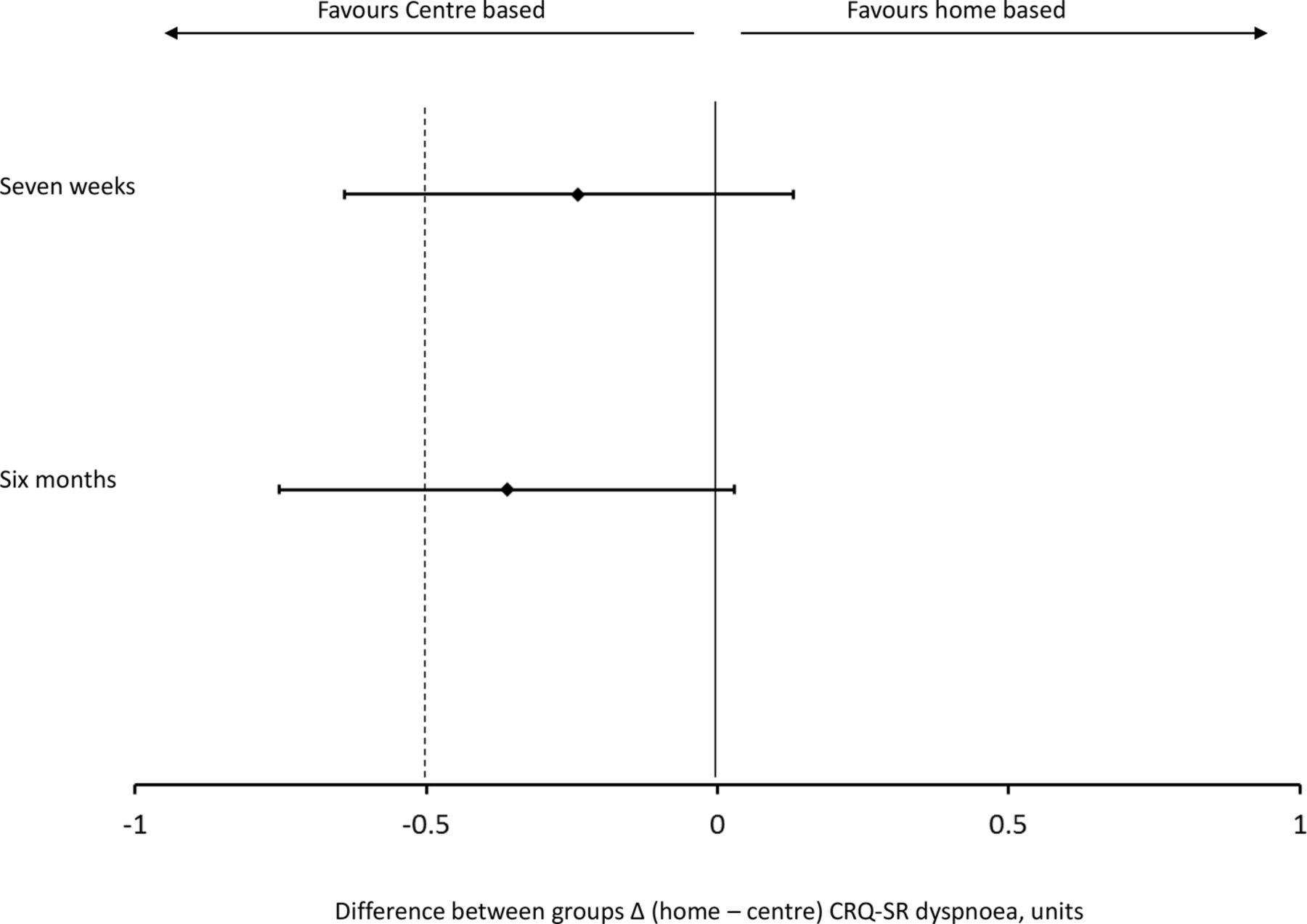
At 7 weeks we observed statistically significant improvements in both groups for the dyspnoea component of the CRQ-SR. The between-group differences were small (mITT: −0.24, 95% CI −0.61 to 0.12, p=0.18; PP: −0.38, 95% CI −0.79 to 0.02, p=0.06; table 2) and not statistically significant. The lower CI exceeds the MCID of 0.5 units, therefore, there remains a degree of uncertainty as to the effectiveness of the home-based intervention on dyspnoea (figure 2). The percentage of participants in each group meeting the MCID threshold of 0.5 for the dyspnoea domain of the CRQ-SR was not significantly different between the two groups (p=0.669), 58.9% and 53.9% for the centre and home-based programmes, respectively (table 3).
Between-group difference in primary and secondary outcomes at 7 weeks postrandomisation follow-up—complete case analysis
Participants meeting the MCID (0.5 units) for the CRQ-SR dyspnoea domain in centre and home-based groups. Complete case analysis
{kind=link}
{kind=link}
Between-group change in CRQ-SR dyspnoea and non-inferiority margin. Data are mean and 95% CI. The dotted line represents the non-inferiority margin. CRQ-SR, Chronic Respiratory Questionnaire self-report.
Secondary outcomes
Within-group changes in the CRQ-SR fatigue, emotion and mastery, from baseline to 7 weeks showed that there was a significant improvement in these domains in the centre-based group only. 95% CI implies that the non-inferiority of the home-based programme remains inconclusive (table 2 and online supplementary file 1).
There were no significant differences between the two groups for anxiety (−0.97, 95% CI −1.98 to 0.04) or depression (−0.79, 95% CI −1.63 to 0.04) (both p=0.06) at 7 weeks. However, the non-inferiority margin (1.5 units) is breached by the 95% CI for both domains (table 2 and online supplementary file 1). Therefore, the non-inferiority of home-based PR cannot be confirmed.
No MCID is established for self-efficacy and therefore inference cannot be made. However, between-group difference was significantly different in favour of the centre-based group.
Both groups improved their performance on the ISWT (p<0.001 for PR and p=0.015 for the home-based group). The between-group differences in ISWT distance were non-inferior to PR (mITT: −23.56, 95% CI −45.30 to −1.81, p=0.03; PP: −19.87, 95% CI −44.39 to 4.65, p=0.11; table 2 and online supplementary file 1).
Important gains were made in ESWT performance for both groups (centre based 353 s (95% CI 270 to 437), p=0.001; home based 212 s (95% CI 139 to 284), p<0.001), with mean change exceeding the MCID in both groups. There was a significant between-group difference in ESWT time (mITT: −141.43, 95% CI −253.25 to −30.63, p=0.01; PP: −128.10, 95% CI −254.31 to −1.89, p=0.05; table 2) in favour of centre-based rehabilitation. The non-inferiority margin (ie, the MCID 186 s) was breached by the lower CI and therefore the non-inferiority of home PR is inconclusive.
Six-month follow-up
At 6 months there was no significant difference in any of the recorded variables (table 4). Gains in ESWT performance were largely maintained at 6 months in both groups (table 4). This was not observed for the ISWT where both groups declined to baseline performance levels. Home based was non-inferior to centre based in the ISWT at 6 months. The gain observed in the dyspnoea component of the CRQ declined in both groups, but remained above the MCID of 0.5 in the centre-based PR group.
Between-group difference in primary and secondary outcomes at 6 months postrandomisation follow-up—complete case analysis
Results from the secondary analysis on the imputed data showed comparable finding to the complete case analysis (see online supplementary table S2 for 7-week data and supplementary table S3 for 6-month data). Within-group differences are shown in table S3 of the online supplementary file 1.
Adverse events
During the 7-week intervention phase of the study 23 adverse events occurred, 9 in the centre-based group and 14 in the home-based group. Two participants in the home-based group and one in the centre-based group died. Seven in the home-based group and three in the centre-based group were admitted to hospital for an exacerbation of their COPD. No serious adverse events were perceived as being related to the study intervention (see table S5 in the online supplementary file 1). There was no significant difference between groups for events reported.
Discussion
The hypothesis that the structure home-based unsupervised PR programme would improve self-reported dyspnoea to a similar degree to conventional centre-based PR remains inconclusive. This is in line with the CONSORT recommendations20 for reporting non-inferiority trials, as the 95% CI of the difference in change between the home-based and centre-based PR groups breached the MCID of 0.5 units. However, no statistically significant difference was detected at 7 weeks between home-based and centre-based PR groups for the primary outcome of dyspnoea. Interestingly, the proportion of participants achieving the MCID was also similar in each group.
There have been several home-based PR programmes reported that have deployed similar outcome measures to the current study.3 24 A key difference in this study is that it is a shorter intervention than many others, some of which have extended to 2 years of supervision and/or support.25 The duration of the supported phase of the intervention was comparable to the recommended length of a rehabilitation programme26 and uniquely offered less direct or indeed indirect supervision. More recently digital versions of rehabilitation have been tested with encouraging results for those completing the programme.27 This study is important as it demonstrates benefits acquired in a short time period similar to the outpatient model of PR. Many previous studies, although categorised as home based, actually provide more supervision and professional contact than a conventional 6 to 8-week course of PR.24–26 28 It is acknowledged that numerically the impact is probably not as great as PR for some of the outcomes and the issue of supervision could be the key factor for the differences seen. The Holland et al study6 demonstrated equivalence of a home-based PR with an 8-week centre-based PR programme, with very similar costs. Interestingly, their improvement in the 6 min walk test distance was below what you might expect in a centre-based PR programme (within-group differences mITT: 10.82 m, 95% CI −4.52 to 26.16).
The mean improvement in the ESWT in our study was above the MCID for both groups at 7 weeks, although numerically greater in the centre group, this difference was not statistically significant. The changes following conventional centre-based PR were not as great as anticipated in the ISWT. The mean (95% CI) change for the ISWT was 42 m (24–59 m) which falls just below the MCID of 48 m for this measure. Previous studies from our centre demonstrated that the mean change for the ISWT after PR met the MCID.10 13 29–31 These studies have recruited participants with, on average, lower baseline FEV1, larger numbers of participants in MRC 4 and 5 and lower mean ISWT scores. This highlights that the current study has potentially recruited a more select subgroup of participants from our PR population at this centre. It is therefore possible that the effect size of outcomes may be smaller in those with milder disease. The ISWT changes in the home-based group were lower than centre-based PR, although not significantly different. Participants were introduced to the study during their initial appointment and they may have seen the unsupervised home programme as the desired or ‘easier option’ and if subsequently randomised to PR may not have fully engaged in the programme (and therefore not complete their home exercise at a high enough intensity or frequency to elicit change in maximal exercise capacity).
Although preference to preferred intervention was not recorded in all participants, the majority of participants questioned would have chosen the home programme. It is therefore possible that this may have influenced their commitment to the programme. These numbers were small so analysis was not completed on these data. In future it would be of interest to determine how much preference influences the outcome of the intervention. Interestingly 55% of those eligible to take part in the trial accepted the trial, despite the initial referral and expectation being for supervised rehabilitation, suggesting that in principle, the home-based intervention seemed acceptable to a number of participants who had been expecting a formal course of rehabilitation.
Overall, the findings of the home-based PR programme suggest that it confers some short-term improvements in dyspnoea and exercise performance although not to the same degree as supervised centre-based PR. It is not possible to rule out non-inferiority as the CI exceeds the non-inferiority margin.
Limitations
The population recruited had a subtly different profile from those generally seen in PR programmes. The reasons for this are probably multifactorial. Participants recruited were generally less disabled by their COPD as there was a greater proportion of MRC grades 2 and 3 compared with other studies.24–26 28 It is likely that home programmes would allow for a more stratified approach to rehabilitation, with home programmes targeted towards those who are generally less disabled. It is also acknowledged that adherence to the programmes was not directly monitored, and that the volume of exercise was not evaluated in the home-based group. However, this was a pragmatic trial and therefore was intentional but may have impacted on the outcomes obtained.
The dropout rate for this study was higher than anticipated and may have led to a higher level of bias. However, it is comparable to other research trials completed in the real-life PR setting.32
We did not complete an economic evaluation of the home-based and centre-based programmes. However, the cost of the home programme with the supply of the SPACE for COPD manual has been previously estimated to be £181.33
Future studies should address the acceptability of this approach for individuals who decline the offer of rehabilitation at any stage of their COPD care pathway due to unacceptability of formal supervised rehabilitation programmes. Overall we believe that this standardised home-based programme, supported by SPACE for COPD, does offer significant benefits to participants as an alternative for supervised PR that should be considered.
Acknowledgments
The authors would like to acknowledge the pulmonary rehabilitation team at Glenfield Hospital, Leicester NHS Trust, who recruited participants. We are grateful to all participants for their involvement in this study. The University Hospitals of Leicester own the IP for the SPACE for COPD manual.
References
Footnotes
Contributors Study design: EJH, LS, MM and SJS. Data collection and management: EJH, KEM, VJW, LDA and LS. Data analysis: EJH and RST. Writing and editing of manuscript: all authors.
Funding GSK provided an unrestricted monetary grant to part fund the this study.
Competing interests None declared.
Ethics approval Leicestershire Northamptonshire and Rutland Regional Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves