Article Text

Statistics from Altmetric.com
Key messages
What is the key question?
What is the underlying cause for fatigue, excessive daytime sleepiness and impaired quality of life in patients with Ehlers-Danlos syndrome?
What is the bottom line?
The high prevalence of obstructive sleep apnoea in the Ehlers-Danlos population may account for significant adverse health effects.
Why read on?
This is the first study to establish a link between obstructive sleep apnoea and the connective tissue disorder Ehlers-Danlos syndrome and provides background information for clinicians.
Introduction
The Ehlers-Danlos syndrome (EDS), a paradigm collagen disorder, comprises a spectrum of monogenic conditions with multisystemic and variable clinical manifestations affecting primarily the skin, ligaments and joints, blood vessels and internal organs. The clinical spectrum varies from mild skin and joint hyperlaxity to severe physical disability and life-threatening complications, and symptoms are usually present in early childhood. The prevalence of EDS is directly related to physician awareness and is estimated to be approximately 1 in 5000 births, which classifies it as a ‘rare’ or ‘orphan disease’.1 Diagnosis of EDS relies mainly on clinical features. It can be supported by biochemical analysis of collagens in cultured fibroblasts, by urinary pyridinoline analysis and by electron microscopy of skin biopsies. Genetic defects affecting the biosynthesis or structure of collagen type I, III and V have currently been implicated in EDS and form the basis of the 1997 Villefranche classification of EDS, which recognises six types, based on clinical phenotype, inheritance pattern and underlying biochemical and molecular defect(s).1–6 Since then, classifications have evolved as new diagnostic parameters became available and thus several new subtypes have been described in recent years.7 ,8
Fatigue, sleep disturbances and daytime sleepiness are clinical problems frequently reported by patients with EDS.9 ,10 EDS features such as those described along with genetically related cartilage defects, craniofacial abnormalities and increased pharyngeal collapsibility due to tissue flaccidity have been proposed to cause obstructive sleep apnoea (OSA)11 ,12—a condition characterised by recurring cessations or reductions in respiratory flow due to upper airway collapse during sleep. When OSA leads to sleep disruption resulting in excessive daytime sleepiness, it is known as OSA syndrome (OSAS), which is thought to affect up to 4% of the middle-aged population in western countries.13 Regardless, up to now the prevalence of OSA and its consequences have not been systematically investigated in patients with EDS. However, compared with the general population, a higher proportion of patients with EDS seem to be investigated in sleep laboratories.11
A vast body of evidence suggests that untreated OSA can lead to a variety of adverse effects including vascular damage and cardiovascular events.14 Recently, we suggested that patients with connective tissue disorders (eg, EDS, Marfan's syndrome) might be especially vulnerable to cardiovascular consequences of OSA, particularly along the aorta.15 Based on the evidence from studies on Marfan's syndrome,16–21 where OSA is highly prevalent and associated with distinct craniofacial phenotypes and cardiovascular consequences, and the fact that patients with EDS are also at high risk to develop aortic aneurysms,22 the same association between OSA and aortic disease could be true for patients with EDS.
Because data on OSA in patients with EDS are lacking we have addressed this knowledge gap by a large parallel-cohort study. We hypothesised that the prevalence of OSA is higher in patients with EDS than in a matched control population, and that it contributes to excessive daytime sleepiness, impaired quality of life and aortic disease.
Methods
Study design and participants
The primary outcome was the prevalence of OSA in patients with EDS compared with a matched control group. Secondary outcomes (optional for study participants) included the association of OSA with quality of life, craniofacial phenotypes, and aortic dimensions. Participants for this study were enrolled from three different sources: University Hospital Zurich EDS database, University Children's Hospital Zurich EDS database and an international network based on EDS associations. EDS was diagnosed and categorised into subtypes according to the Villefranche diagnostic criteria1 and hypermobility was assessed according to the Beighton score.23 If applicable, the clinical EDS diagnosis was objectively confirmed by either (1) gene analysis for an identified EDS culprit gene listed in the ‘Online Mendelian Inheritance in Man’ (see online supplementary eTable 1); (2) pathological finding suggestive for a specific EDS subtype in an electron microscope study or abnormal biochemical analysis of collagen in cultivated fibroblasts3 or (3) increased ratio (>0.5) of deoxypyridinoline to pyridinoline crosslinks in biochemical urine analysis for EDS VIA.24–26 For each patient with EDS, a control subject from the local population in Zurich was recruited to specifically match the patient with EDS in terms of sex, age (±3 years), height (±20 cm) and weight (±15 kg). Control subjects were recruited via online advertisements and leaflets stating the main inclusion criteria for the study including the desired age, sex, height and weight but not mentioning ‘sleep apnoea’ or ‘sleep disturbances’ to minimise selection bias. Subjects were eligible for study enrolment if they were aged 18 years or above, not pregnant and physically and intellectually capable to adhere to the study protocol.
supplementary data
Respiratory polygraphy
Full night respiratory polygraphy was performed using an out-of-centre level-3 portable sleep test (ApneaLink Air, ResMed, San Diego, California, USA) during the habitual sleep time of the subjects. All sleep recordings took place in the home environment of patients in accordance with the recommended setup.27 OSA was defined as an apnoea–hypopnea index (AHI) ≥5/hour and OSAS was diagnosed according to the criteria of the International Classification of Sleep Disorders 2014 (ICSD-3).28 The diagnosis of OSAS required either an AHI ≥15/hour (obstructive events) or an AHI ≥5/hour coupled with signs/symptoms (ie, excessive daytime sleepiness assessed via the Epworth sleepiness scale, loud snoring or observed apnoeas assessed via the STOP-Bang score) or a specific medical disorder (ie, hypertension).28 Sleep studies were all reviewed manually by two trained investigators (TG, NS) and scored according to the 2007 American Academy of Sleep Medicine recommendations (≥30% drop of airflow lasting at least 10 s with ≥4% oxygen saturation drop).27 Investigators were blinded to the EDS status and results of the questionnaires. A third clinical sleep expert (DF) performed random quality checks. When polysomnography level-1 data were available (n=3), they were preferred over level-3 monitor data. Methods for secondary outcomes (including quality of life, aortic diameter, blood pressure, craniofacial photogrammetry and lung function) can be found in the online supplementary information.
Statistical analysis
A sample size of 200 was established (α=0.05 β=0.2) to detect an absolute difference in symptomatic OSA prevalence of approximately 12%, assuming the prevalence in the control arm (young, non-obese) is 3%.19 Continuous outcomes were summarised by EDS and non-EDS participants (controls) using mean (SD) or median (25th–75th percentiles) as appropriate. Conditional logistic regression was used to compare the prevalence of OSA and OSAS between the two groups in an adjusted analysis, adjusting for the matching variables. Mixed-effects linear regression was used to compare continuous variables assessing sleep apnoea severity (ie, AHI) between patients with EDS and controls, adjusting for the matching variables and accounting for the cluster of each ‘EDS/non-EDS’ pair as a random effect. Continuous secondary outcomes, which did not measure sleep apnoea severity, were analysed using multiple linear regression without accounting for the clustering, due to lack of complete data in each pairing. A 2-sided p value <0.05 was considered statistically significant for all reported tests. All analyses were conducted with Stata V.14 (StataCorp LP, College Station, Texas, USA).
Ethics
The study was approved by the Cantonal Ethics Committee Zurich, Switzerland (KEK-ZH 2015-0144). All participants gave written informed consent before study participation and the study is registered with ClinicalTrials.gov, number NCT02435745.
Results
Characteristics of participants
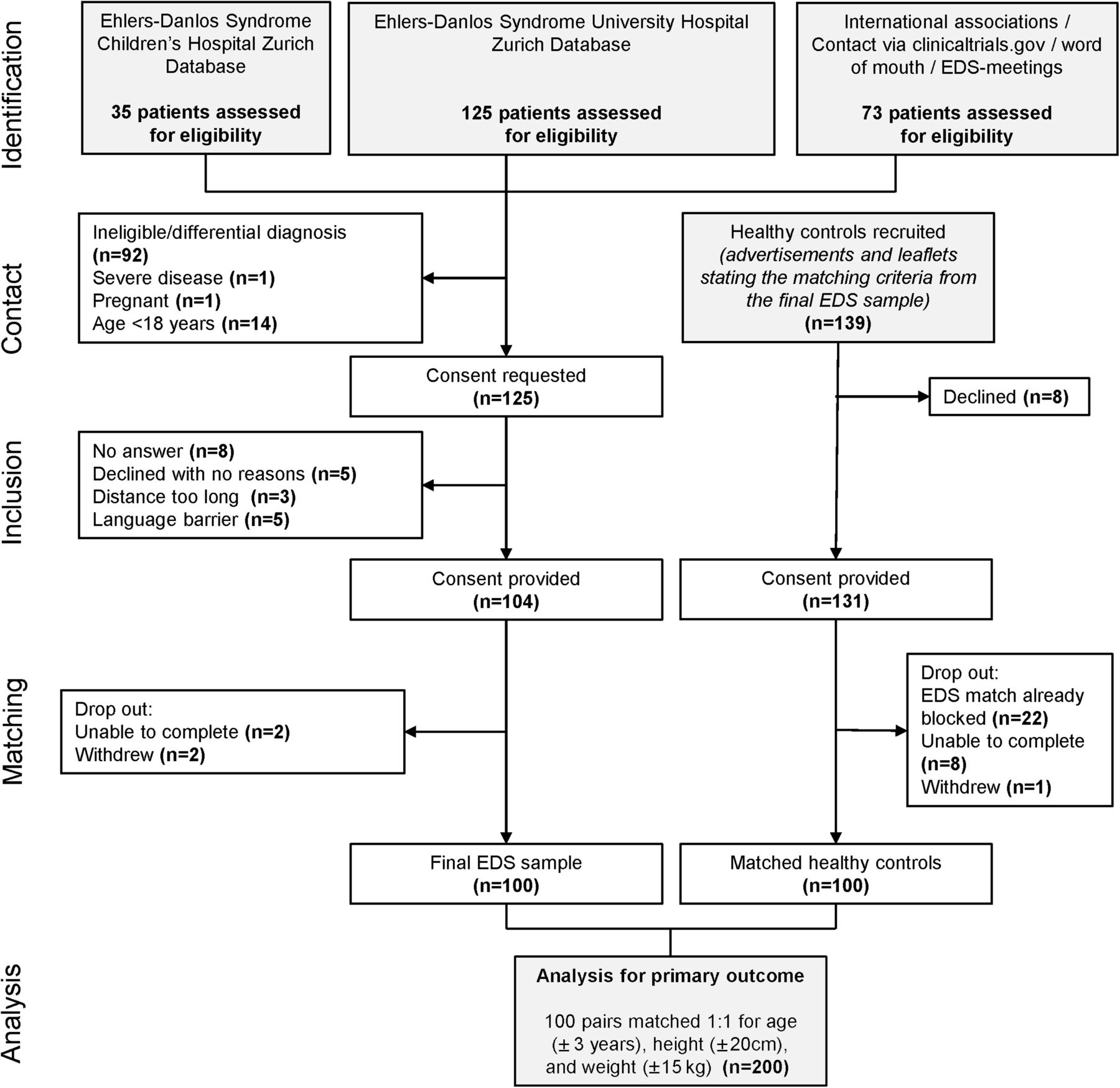
The study flow is shown in figure 1. EDS diagnosis according to the Villefranche criteria3 was confirmed in all cases and additionally objectified in 83% of cases (see online supplementary eTables 2–5.
Summary statistics for patients with EDS and matched controls

Study flow chart. The majority of study participants were recruited by hospital-wide screens of electronic databases (Children's Hospital Zurich and University Hospital Zurich). Between April and December 2015, 200 study participants were enrolled. EDS, Ehlers-Danlos syndrome.
Primary outcome
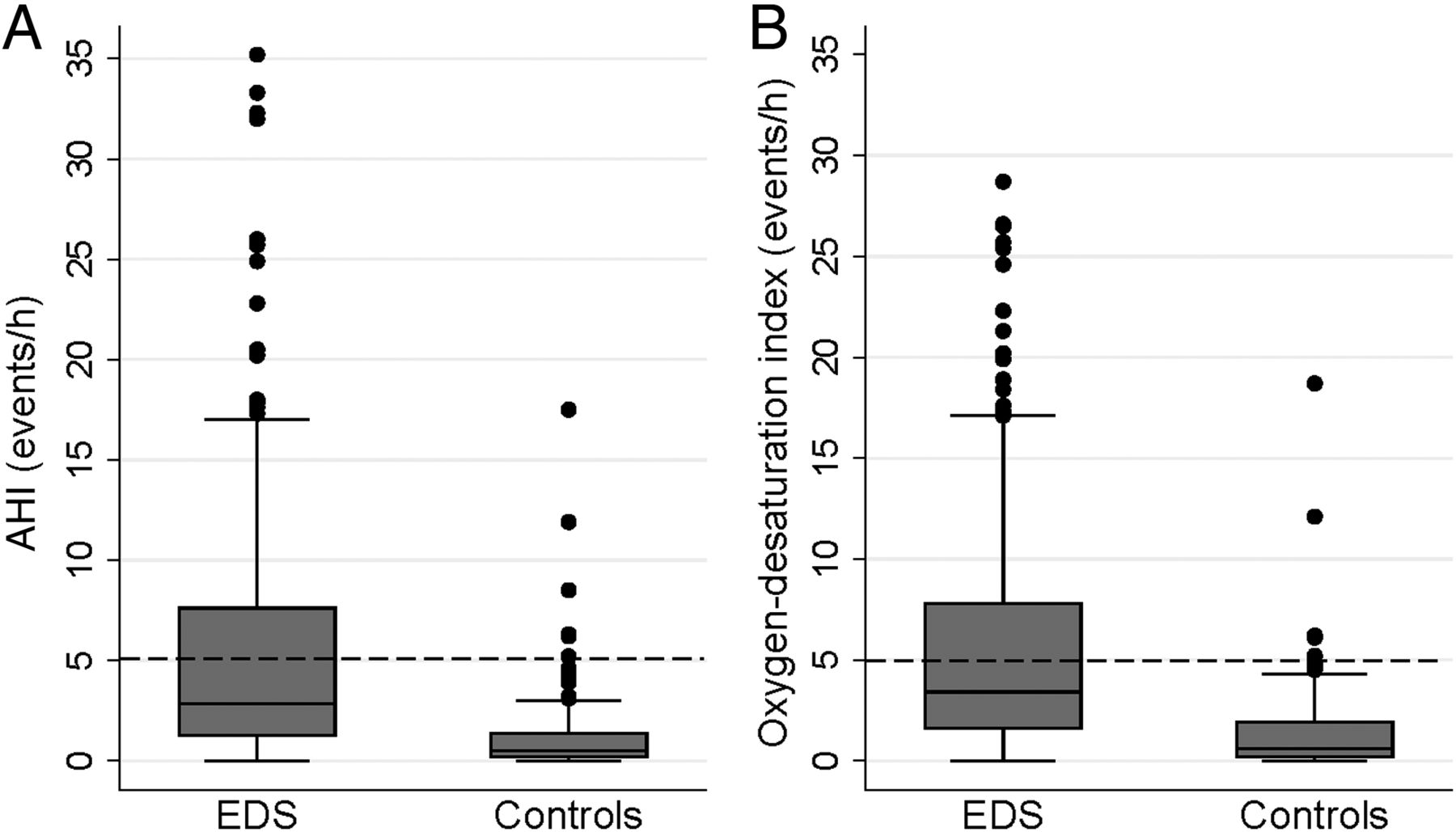
Eleven study participants (5.5%) repeated the sleep study due to insufficient data recorded on the first occasion. OSA prevalence in patients with EDS was higher when compared with matched controls (32% and 6%, respectively; (OR 5.3 (95% CI 2.5 to 11.2); p<0.001). OSAS was significantly more prevalent in patients with EDS compared with control subjects and total time in bed during the study night was longer in patients with EDS (table 2; figure 2). However, there was no difference in self-reported average hours of sleep during the past month (EDS 6.98±1.12 hours vs Controls 6.77±1.84 hours, p=0.272). In a post hoc analysis of the patients with EDS only, no difference in AHI was found between solely clinically diagnosed EDS (n=17) and objectively confirmed EDS (n=83) participants (2.7/hour (1.3–8.7) vs 2.9/hour (1.2–7.2); p=0.55).
Sleep study data for the study population and subgroup results
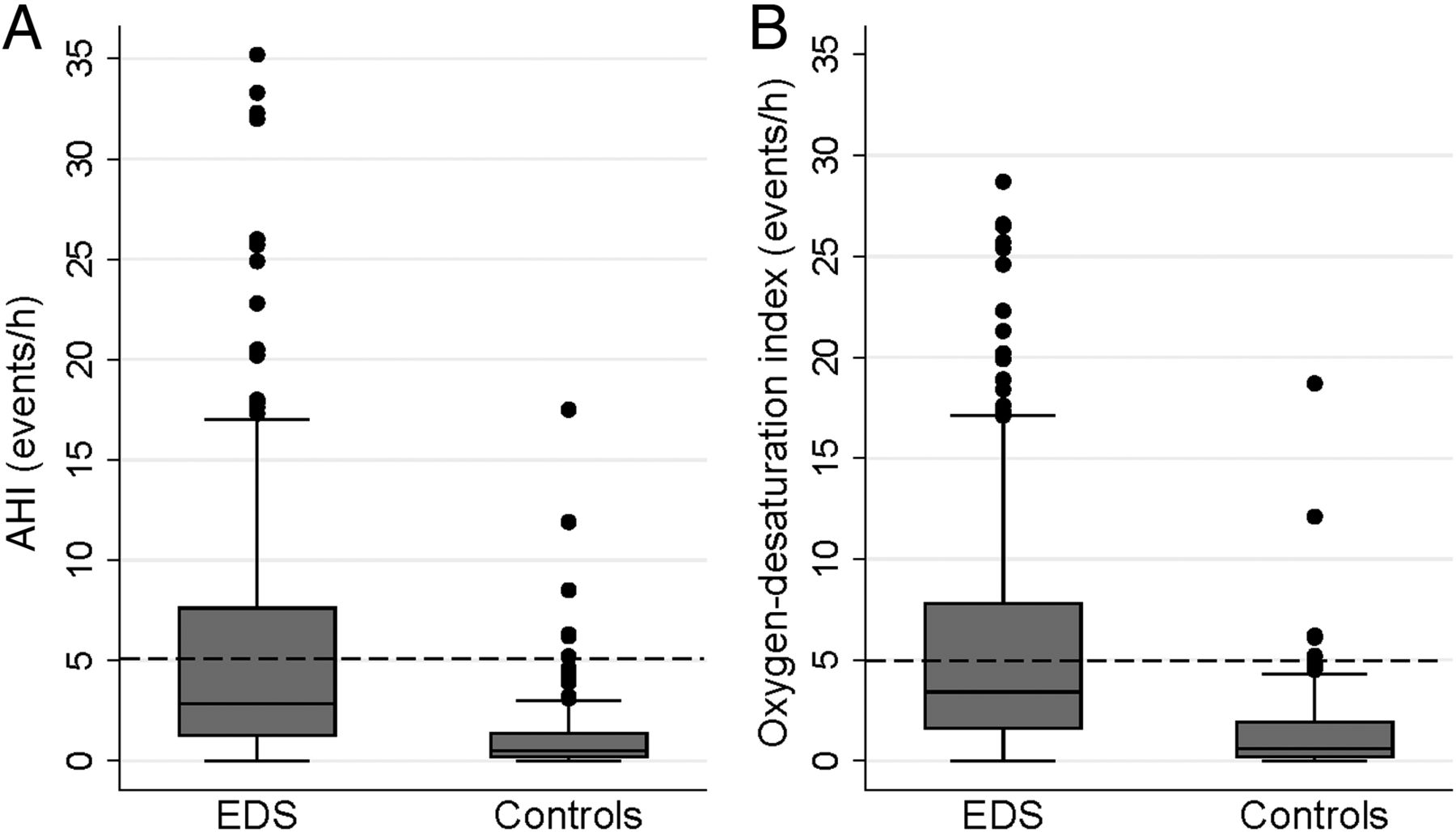
Apnoea–hypopnea index (AHI) (A) and oxygen-desaturation index (B) by groups. The threshold for obstructive sleep apnoea is marked by the dashed line. Both median (quartiles) indices (events/hour) were higher in the group with Ehlers-Danlos syndrome (EDS) when compared with the control group with 2.9 (1.3–7.6) versus 0.5 (0.2–1.5), p=0.007 and 3.4 (1.6–7.8) versus 0.6 (0.2–1.9), p<0.001.
In the EDS cohort, hypopneas were the most common respiratory events (64%), followed by apnoeas (36%). No Cheyne-Stokes respiration patterns were documented. The median number of snoring events per hour was higher in patients with EDS and OSA than in patients with EDS who have an AHI <5/hour (14/hour (6–41) vs 5/hour (3–9); p<0.001), which adds confidence that the apnoeas were of the obstructive type. In an unadjusted analysis, patients with OSA scored higher on the Epworth Sleepiness Scale (ESS) when compared with patients with an AHI <5/hour (8.8±4.7 vs 10.7±4.0; p=0.02) indicating that OSA was associated with increased daytime sleepiness.
Secondary outcomes
Generally, patients suffering from OSAS reported lower quality of life compared with asymptomatic patients (e figure 3). Patients with EDS reported lower quality of life (figure 3), higher daytime sleepiness (Epworth Sleepiness Scale), a lower sleep quality (Pittsburgh Sleep Quality Index) and more depressive symptoms Patient Health Questionnaire-9 (PHQ-9) when compared with matched controls (see online supplementary eTable 6). There was no evidence of a difference between the two study groups in terms of aortic dimensions and blood pressure (table 2). However, patients with EDS featured a higher daytime resting and night time heart rate (table 2). Lung function, a potential confounder of nocturnal desaturations, was within normal limits (see online supplementary eTable 7). In terms of craniofacial phenotyping, the predefined 40 facial parameters29 indicated no evidence of a difference between these groups (see online supplementary eTable 8). Additional subgroup analyses can be found in online supplementary eTables 9–12.
{kind=link}
{kind=link}
{kind=link}
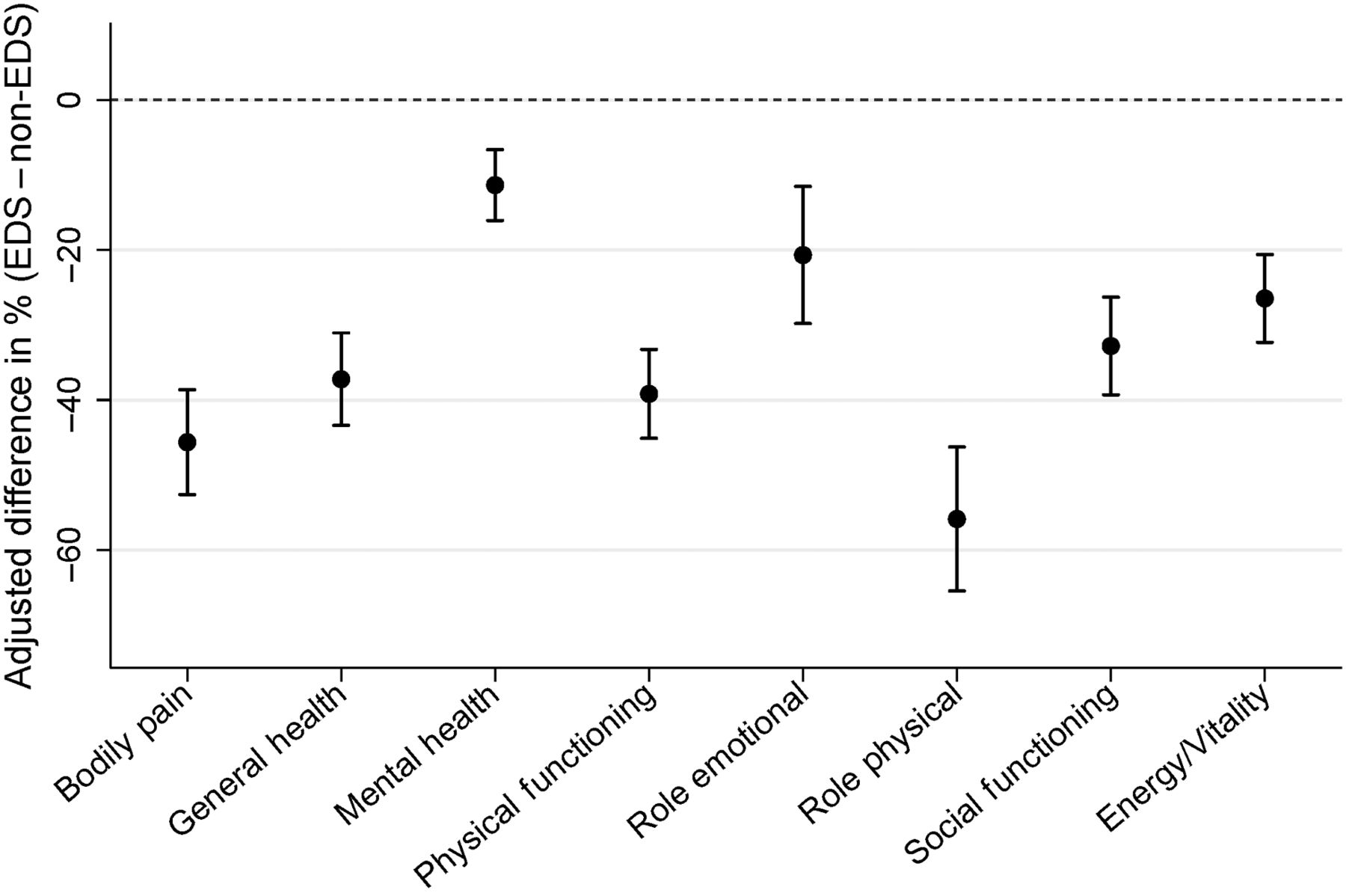
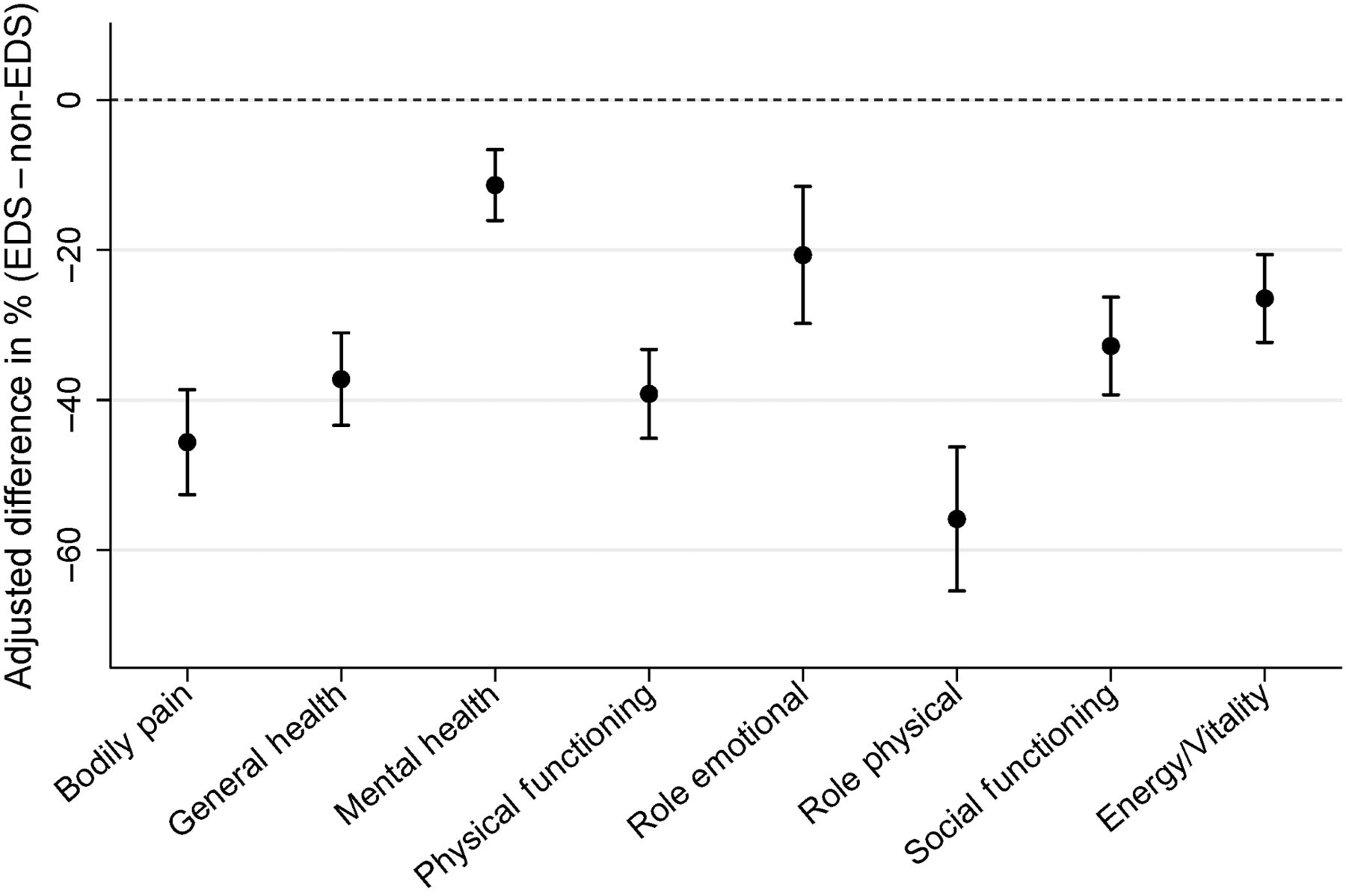
Short-form 36 (SF-36) adjusted difference between the population with Ehlers-Danlos syndrome (EDS) (n=100) and the control group (n=100). Mean and 95% CI each of the SF-36 domains displayed in % adjusted difference (EDS−non-EDS).
Predictors of OSA
In the mixed effects model, weight and age were statistically significant direct predictors of a high AHI (both p<0.01). Furthermore, in patients with EDS, neck circumference was moderately correlated with AHI (r=0.44; p<0.001). The median Beighton score was 6 (4–8) and there was no association with OSA severity (eg, AHI, p=0.97).
Discussion
To our knowledge, this is the first study to determine the prevalence of OSA in patients with EDS. We approximated that a quarter of patients with EDS suffer from symptomatic OSAS and fulfil the formal criteria for treatment. Our data also suggest that OSA has a role in the development of fatigue, daytime sleepiness and impaired quality of life in patients with EDS. A large body of evidence has documented that these symptoms represent significant problems in day-to-day life in the EDS population.9 ,10 ,30 High-quality data about adverse effects of OSA in EDS are clinically crucial, because OSA is treatable and its therapy has been shown to effectively reduce daytime sleepiness, to increase quality of life and to successfully prevent other adverse consequences.31–33
According to our study, 32% of patients with EDS suffer from OSA (AHI ≥5/hour) and 23% suffer from symptomatic OSAS. In the control population, these numbers were 6% and 3%, respectively. This novel finding is particularly interesting given that the subjects were predominantly premenopausal women. These absolute numbers may vary depending on how OSA is defined and the AHI is measured. Epidemiological studies using the same methods (ie, 4% drop-off for oxygen desaturations) reported a similar 32.8%20 OSA prevalence in Marfan's syndrome and 5% prevalence of oxygen-desaturation index ≥5/hour34 in a matched healthy population. However, more recent studies report considerably higher OSA prevalence rates in the general population.35 ,36 This is most likely due to different study populations in terms of age, body mass index (BMI), and sex, other sampling frames, distinctive recording techniques (full polysomnography), and alternative scoring criteria. Therefore, caution is needed when comparing the prevalence of OSA with other population-based studies or sleep studies from individuals, which emphasises the need for a matched control group.
OSA is a common disorder yet sometimes very challenging and relatively expensive to diagnose. Despite a high OSA prevalence among patients with EDS in this study and frequently reported significant sleep disturbances,9 ,10 patients were not familiar with OSA. When they were asked the question at the beginning of the questionnaire ‘Did you already know about the disorder “OSA” before the start of the study?’ 54% of the EDS population in this study answered ‘no’.
The fact that greater weight, male sex and older age were statistically significant predictors of OSA among patients with EDS suggests a similar pathophysiology for the condition in patients with EDS as in the general population. Moreover, our craniofacial photography data, which reflects underlying aspects of craniofacial skeletal abnormalities,37 appears to exclude such abnormalities as key mediators of OSA risk in patients with EDS. Therefore, the first-line therapy in overweight patients with EDS should be weight loss. Beyond that, EDS-specific traits such as genetically related cartilage defects and increased pharyngeal collapsibility due to tissue flaccidity have already been proposed to cause OSA.11 ,12 In our study, the impact of the binary EDS variable on AHI was comparable to that of a +11 kg/m2 BMI gain (based on the control data in this study).
We previously hypothesised an adverse impact of OSA on aortic disease in patients with EDS.15 A study has reported a 28% prevalence of aortic root dilation among patients with classical and hypermobile EDS subtype.22 We could, however, not replicate these findings in our study population, consisting mainly of the classical (35%) and hypermobile (45%) EDS subtype. Only 4% (n=2) of the patients with EDS fulfilled the criteria of an aortic aneurysm but neither of them fulfilled the criteria for OSA. Notably, all patients with a vascular EDS subtype undergoing measurements (n=3) received an aortic replacement graft.
Of those diagnosed by the ‘clinical’ Villefranche criteria (n=17; see online supplementary eTable 3), the majority of 12 patients was suspected to have EDS hypermobile type at the time of this study. First, this EDS type is known to be prone to subjective tests, such as the Beighton score and skin assessment, as often no molecular diagnostic tests are available to confirm the clinical diagnosis (ie, presence of both major criteria).3 To date, there is no consensus on the minimum criteria for the diagnosis of EDS hypermobile type. Second, EDS hypermobile type shares many overlapping phenotypic features with the joint hypermobility syndrome and the boundaries between the two entities are somewhat blurred. Recently, experts suggested that EDS hypermobile type and the joint hypermobility syndrome represent the same phenotypic group of patients.38 It is expected that the diagnostic criteria might shift for these 12 candidates but to date there is no molecular evidence to clarify their relationship. Because of this classification problem, in the current study, the most recent diagnostic criteria for the joint hypermobility syndrome (Beighton criteria23) and the EDS (Villefranche criteria3) for differential diagnosis were applied. Skin involvement was the major discriminative symptom in this study for these two conditions, excluding 92 subjects during the recruitment process (see flow chart). We acknowledge that diagnostic accuracy in this ‘clinical’ subgroup suffers from subjective judgement. However, post hoc subgroup analysis (see online supplementary eTable 10) suggested no difference in the primary outcome for the EDS hypermobile type and thus this group is unlikely to affect the overall results of this study. Whether OSA is also highly prevalent in joint hypermobility syndrome remains to be established.
Limitations
As we did not perform full polysomnography, we were not able to assess sleep stages and the exact nature of apnoeas (eg, obstructive vs central). However, a recent meta-analysis has shown that level-3 portable devices (ie, ApneaLink Air devices used in this study) showed good diagnostic performance for OSA compared with the gold standard polysomnography, and in 19 studies, no significant difference in the clinical management parameters between patients who underwent either test to receive their diagnosis was found.39
Although rigorous one-to-one matching was performed, a confounding bias below the 0.05 level may remain. Furthermore, within-group comparisons (eg, within patients with EDS) and post hoc analysis may lack statistical power since the primary outcome was powered based on whole group comparisons (ie, EDS vs non-EDS). More generally, a study population with a predominantly white female European background and with a low prevalence of obesity could limit generalisability of our data to other populations (ie, predominantly male, or other ethnicities).
In a post hoc analysis, we found no evidence of a possible selection bias in regard to the original EDS population (see online supplementary eTable 9). The high proportion of females in our registry databases is consistent with proportions reported by other EDS registers9–11 ,30 but ultimately may be considered as a limitation when it comes to the generalisability of the data.
Implications
Based on our results, we advise clinicians in the care of patients with EDS to specifically ask for OSA-related symptoms—especially when fatigue and daytime sleepiness are present. The STOP-Bang score represents an attractive tool for this task and its discriminatory property remains similar in the EDS population (see online supplementary eTable 13). In a patient with EDS suspected of OSA, our data suggest performing a polysomnography or respiratory polygraphy (rather than oximetry alone) to capture the predominantly high numbers of hypopneas in this population. It also should be noted that a low BMI does not necessarily rule out a possible OSA diagnosis in a patient with EDS. When it comes to OSA treatment in the EDS population, it needs to be acknowledged that the effect of OSA on daytime sleepiness (ESS Δ+1.9 points) and quality of life (SF-36 Δ-18% across all 8 domains) was about half of the overall difference in the comparison to a non-EDS population (ESS Δ+4 points; SF-36 Δ-33% across all 8 domains). Thus, OSA treatment may only have moderate effects on symptoms in patients with EDS.
Adverse effects of OSA were observed in our cohort such as the resulting demand of a longer total time in bed (table 2) or a higher resting heart rate at night time and daytime (table 2), which reflects chronic sympathetic nervous system activation—another well-known consequence of OSA.40 Other potential long-term consequences of untreated OSAS include increased risk of road traffic accidents, reduced quality of life and possibly higher mortality.41 Recent meta-analyses confirm the effectiveness of OSA treatment on various outcomes.31 ,32 Randomised controlled trials are needed to assess the effectiveness of various treatments in the EDS population.
Conclusion
OSA is highly prevalent and under-recognised in EDS. Because OSA may contribute substantially to fatigue, daytime sleepiness and impaired quality of life in this population, patients with EDS and excessive daytime sleepiness should be evaluated for OSA.
Acknowledgments
We thank the patients, organisations and relatives who gave so much for this study and often travelled long distances to participate in this study; without them this study would not have been possible. Specifically, Dirk Hochtritt, Rea Spörri and Jasmin Polsini (Ehlers-Danlos Netz Schweiz); Juergen Grunert, Friederike Müller, Markus Irene and Wibke Jungermann (Deutsche Ehlers-Danlos-Initiative e.V.); Barbara Kleffmann (Ehlers-Danlos-Selbsthilfe e.V.) for administrative support; Stefanie Armbruster who supported the recruitment process; Matthias Baumann (Medical University of Innsbruck, Austria) for the help during the recruitment process.
References
Footnotes
Contributors TG, CG, MR and MK conceived, designed and analysed the overall study. TG and DJB designed and coordinated data collection and statistical analysis. TG, KS, CS and NS assessed study outcomes. TG, MK and PAC undertook the administration of the study. TG and MK applied for funding for this study. TG, NS, DF and CS oversaw the study assessments (craniofacial photographs, ultrasound measurements, and aortic stiffness). All authors oversaw, contributed and approved the final manuscript. TG and MK had full access to all the data in the study and had final responsibility for the decision to submit for publication. This was an investigator-initiated study.
Funding The research was supported by grants from ‘Lunge Zürich’ and ‘Lungenliga Schweiz’.
Disclaimer The funder of the study had no role in study sponsoring, design, data collection, data analysis, data interpretation, or writing of the manuscript.
Competing interests PAC reports grants, non-financial support and other from ResMed, grants, non-financial support and other from SomnoMed, grants and personal fees from Exploramed, personal fees and non-financial support from Zephyr Sleep Technologies, personal fees from NovoNordisk, other from Fisher & Paykel Healthcare, personal fees from Quintessence Publishing, personal fees from UpToDate, all outside the scope of the submitted work.
Patient consent Obtained.
Ethics approval Cantonal Ethics Committee Zurich.
Provenance and peer review Not commissioned; externally peer reviewed.