Article Text

Abstract
With an increase in cases of multidrug-resistant Pseudomonas aeruginosa, alternative and adjunct treatments are needed, leading to renewed interest in bacteriophage therapy. There have been few clinically relevant studies of phage therapy against chronic lung infections. Using a novel murine model that uses a natural respiratory inhalation route of infection, we show that phage therapy is an effective treatment against chronic P. aeruginosa lung infections. We also show efficacy against P. aeruginosa in a biofilm-associated cystic fibrosis lung-like environment. These studies demonstrate the potential for phage therapy in the treatment of established and recalcitrant chronic respiratory tract infections.
- Cystic Fibrosis
- Bacterial Infection
- Respiratory Infection
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Chronic lung infections with Pseudomonas aeruginosa, associated with diseases such as cystic fibrosis (CF), non-CF bronchiectasis and COPD are often recalcitrant to treatment with antibiotics. With the rise of multidrug-resistant bacterial pathogens, there has been increased interest in the therapeutic potential of bacteriophages (phage) as an alternative or supplement to conventional antibiotics.1 Although progress has been made with the use of phage therapy against P. aeruginosa infections in chronic otitis2 and burn wounds,3 studies in chronic lung infections are restricted to a limited number of preclinical evaluations.4 Previous studies in animal models have demonstrated potential, but these have targeted short-term acute respiratory infections,5 ,6 or have involved very short time intervals between initial start of infection and therapeutic application.7 ,8 In addition, most models of chronic respiratory infection use agar beads impregnated with bacteria, which do not represent the natural infection process. Because of these limitations, previous studies were not designed to test phage efficacy against established chronic respiratory infections with P. aeruginosa.
We have recently developed a novel murine model of P. aeruginosa chronic lung infection9 that uses a natural respiratory inhalation route of infection. In this model, P. aeruginosa LESB65 (a representative of the most common clone of P. aeruginosa isolated from patients with CF in the UK, the Liverpool epidemic strain) adapts to its host niche in the nasopharynx, leading to migration and subsequent establishment in the lungs (as occurs in human chronic lung infection), and allows experiments to be conducted for much longer time periods (beyond 21–28 days).9 Infection is associated with the expression of biofilm-associated genes (as in CF), and ‘host-adapted’ bacteria recovered from the model are better able to establish lung infections when reintroduced to naïve mice.9 To provide a more stringent test of the potential of phage therapy in a clinically relevant model of chronic P. aeruginosa lung infection, we used a previously reported phage10 to challenge established populations of strain LESB65 (or the host-adapted derivative strain NP22_29), varying the length of time between establishment of initial infection and the application of the therapeutic agent.
The methodology associated with the murine model (using BALB/c mice 6–8 weeks old) has been described previously.9 The study was performed with the approval of, and in strict accordance with, the standards of the UK Home Office and the University of Liverpool Research Ethics Committee. Mice were infected intranasally with a fresh mid-log phase dose of 2×106 colony-forming units (CFU) of P. aeruginosa in 50 μL phosphate-buffered saline (PBS). An amount of 2×107 phage (phage PELP2010) or PBS control was administered by the same route at indicated times. Mice were culled at predetermined times post infection by cervical dislocation. Lungs were collected, homogenised, serial-diluted and plated on Pseudomonas-selective plates (Oxoid, UK) to obtain CFU counts of bacteria recovered. Each experiment was repeated twice with five mice per group to give a total of ten per group per time point. Statistical analysis was performed using two-way ANOVA.
We first confirmed the efficacy of phage against strain LESB65 in an artificial sputum medium biofilm model9 developed to resemble the key physicochemical features of the lung of a patient with CF, including the presence of amino acids, mucin and extracellular DNA (figure 1). There was a 3-log reduction in P. aeruginosa CFU recovered from the phage-treated biofilm (after 24 hours), indicating that PELP20 can penetrate and kill bacteria within a biofilm-associated CF lung-like environment (figure 1).
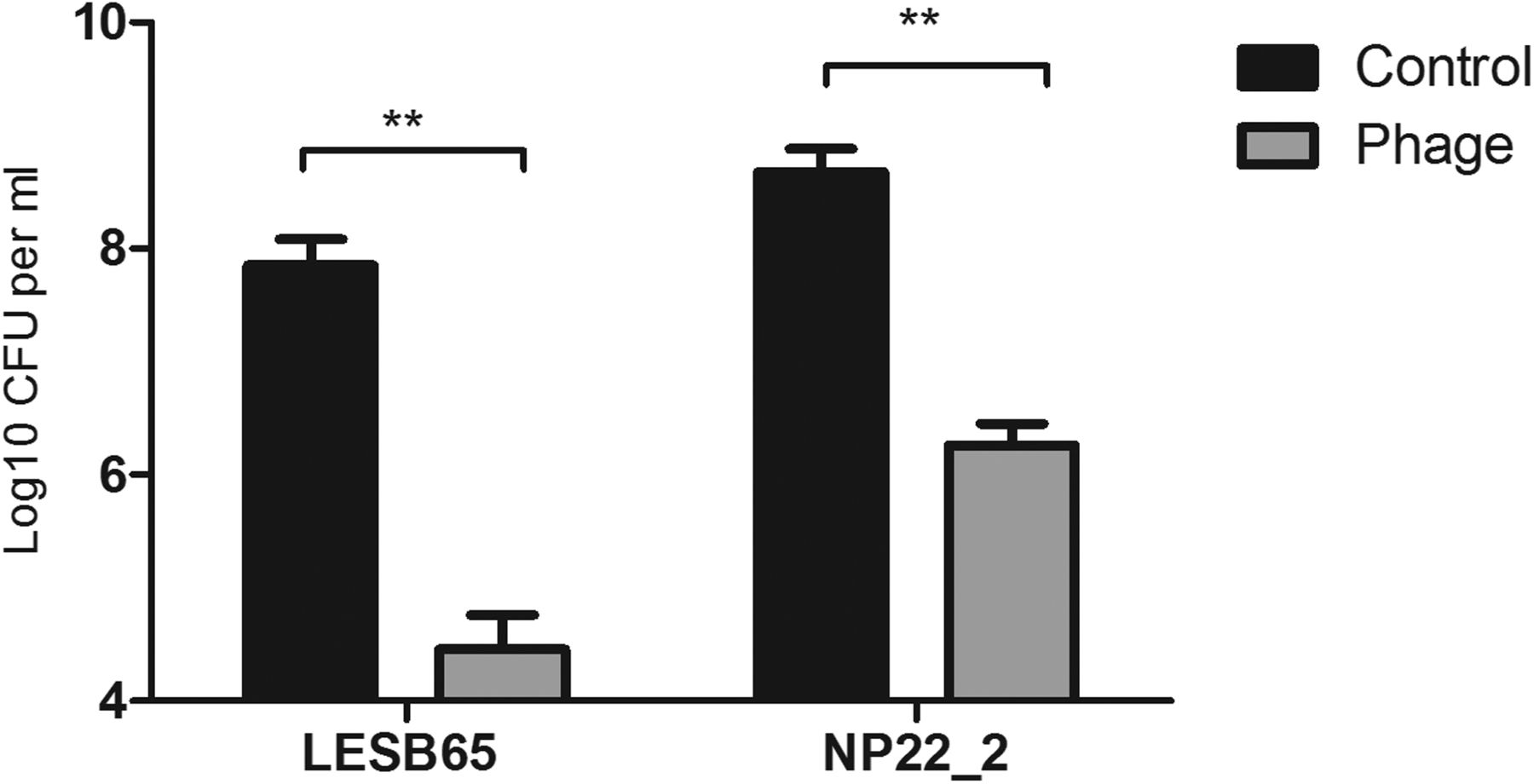
Phage activity against Pseudomonas aeruginosa (LESB65 wild type (WT) and adapted strain NP22_2) in an artificial sputum medium (ASM) model. Phage PELP20 (1×108 plaque-forming units) was administered 72 hours after establishment of P. aeruginosa mature biofilm in the ASM model; the figure shows colony-forming units (CFU)/mL at 24 hours post phage administration. Significant differences were determined using a two-way analysis of variance (**p≤0.01). Error bars indicate standard error of the mean SEM (n=6 biological replicates, mean values obtained from triplicate samples). There was no significant difference in fold reduction after phage treatment between LESB65 WT and NP22_2.
In our initial murine model experiments, after infection of the mice with P. aeruginosa LESB65, phage were administered either (a) at 24 and 36 hours post infection, with bacterial CFUs counted at 48 hours (treatment 1) or (b) phage administration at 48 and 60 hours post infection, with bacterial CFUs counted at 72 hours (treatment 2). In both cases, complete clearance of P. aeruginosa from the lungs was achieved (figure 2). No reduction in CFUs was seen when ultraviolet-inactivated phage with no lytic activity was used (data not shown). We further extended the treatment gap between infection and application of phage to 6 days post infection, using the adapted LESB65-derived strain NP22_2, which readily establishes chronic infection in the murine lung.9 Here, the phage were administered at 144 hours (6 days) and 156 hours (6.5 days) post infection, with CFU counts at 168 hours (7 days) post infection (treatment 3). Phage therapy was again highly effective against the established 6-day lung infection, completely clearing bacteria from the lungs of 70% of mice, and significantly reducing CFU counts in the other 30% compared with controls (figure 2).

{kind=link}
{kind=link}
Phage activity against Pseudomonas aeruginosa (LESB65 wild type and adapted strain NP22_2) infection in the murine lung. The figure shows colony-forming units (log CFU per lung) present in the lungs of mice following intranasal infection with LESB65 (treatments 1 and 2) and NP22_2 (treatment 3). The mice were randomly assigned to a group and subsequently treated with phage PELP20 or phosphate-buffered saline control using three different treatment protocols: (1) phage administration at 24 and 36 hours post infection, with bacterial CFUs counted at 48 hours; (2) phage administration at 48 and 60 hours post infection, with bacterial CFUs counted at 72 hours; (3) phage administered at 144 and 156 hours post infection, with CFU counted at 168 hours. Significant differences determined using a two-way analysis of variance and Bonferroni’s multiple comparison test as post hoc analysis are denoted using asterisks (***p≤0.001). The selected time points for sampling were based on our previous study.9
This is the first study reporting the efficacy of phage therapy up to 7 days post infection in a model where P. aeruginosa establishes a natural long-term chronic lung infection. Hence, we believe that it represents the sternest challenge yet for the efficacy of phage therapy in a respiratory infection model system. We show that phage administered intranasally up to 6 days after establishment of chronic lung infection were efficient in reducing bacterial numbers in the lungs of mice infected with P. aeruginosa, demonstrating the potential for phage therapy in the treatment of established and recalcitrant chronic respiratory tract infections. There are well-discussed potential limitations with respect to phage therapy, in terms of host range, potential toxicity and the development of resistance. However, the key unanswered issue still remains, whether phage can gain access to and kill the bacteria in the spatially complex biofilm-associated mixed communities present in, for example, the CF lung. We have found that in a biofilm-associated murine model of chronic lung infection, and in an artificial sputum medium biofilm model, phage can effectively kill P. aeruginosa. While there is still more work to be done in developing phage cocktails with sufficient range, these data suggest that phage therapy could be an effective therapeutic approach against chronic respiratory infections, either alone against antibiotic-resistant bacteria or in combination with conventional antimicrobials.
Acknowledgments
The authors acknowledge Marina Goderdzishvili and Nina Chanishvili Eliava (Institute of Bacteriophages, Microbiology and Virology, Tbilisi, Georgia) for providing the phage mixture from which phage PELP20 was isolated.
Footnotes
CW and AK are co-senior authors
Contributors EMW and DRN designed and performed the in vivo experiments. EMW, BK and JSS performed the in vitro experiments. EMW, DRN, MRJC, CW and AK analysed the data. EMW, CW and AK wrote the manuscript. CW and AK conceived, designed and supervised the study and contributed equally throughout.
Funding Institute of Infection and Global Health, University of Liverpool.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.