Article Text

Abstract
We investigated associations of plasma lipoproteins with subclinical interstitial lung disease (ILD) by measuring high attenuation areas (HAA: lung voxels between −600 and −250 Hounsfield units) in 6700 adults and serum MMP-7 and SP-A in 1216 adults age 45–84 without clinical cardiovascular disease in Multi-Ethnic Study of Atherosclerosis. In cross-sectional analyses, each SD decrement in high density lipoprotein cholesterol (HDL-C) was associated with a 2.12% HAA increment (95% CI 1.44% to 2.79%), a 3.53% MMP-7 increment (95% CI 0.93% to 6.07%) and a 6.37% SP-A increment (95% CI 1.35% to 11.13%), independent of demographics, smoking and inflammatory biomarkers. These findings support a novel hypothesis that HDL-C might influence subclinical lung injury and extracellular matrix remodelling.
- Clinical Epidemiology
- Idiopathic pulmonary fibrosis
- Imaging/CT MRI etc
- Interstitial Fibrosis
Statistics from Altmetric.com
Cardiovascular disease (CVD) is a prevalent comorbidity in adults with fibrotic interstitial lung disease (ILD), yet the mechanisms underlying this association remain unclear.1–3 Lipids and lipoproteins contribute to the pathogenesis of CVD and in recent years have been linked to a number of lung diseases, including asthma and COPD.4 ,5 However, few studies have looked at the role of lipids and lipoproteins in interstitial lung injury, inflammation and fibrosis.6 ,7
Imaging-based identification of lung injury, matrix remodelling and fibrosis in asymptomatic individuals is a novel way of studying subclinical ILD and may lead to a better understanding of the early causes of fibrosis. Two methods have been developed and validated to identify subclinical ILD: automated detection using quantitative CT densitometry to measure increased lung attenuation (high attenuation areas, HAA) and visual inspection for the presence of interstitial lung abnormalities (ILA).8–11 In the current study, we examined associations of plasma lipids and lipoproteins with HAA, ILA and serum biomarkers of lung inflammation and extracellular matrix remodelling (SP-A and MMP-7) in the Multi-Ethnic Study of Atherosclerosis (MESA).12–15 We hypothesised that the presence of coronary artery calcium, high low density lipoprotein cholesterol (LDL-C), low high density lipoprotein cholesterol (HDL-C) and their respective components would be associated with HAA, ILA and higher MMP-7/SP-A levels independent of demographic characteristics, smoking and inflammatory biomarkers.
Full Methods are available in the online supplementary data.
supplementary data
The MESA is a multicentre, prospective cohort study of 6814 adults age 45–84 sponsored by the National Heart Lung and Blood Institute to investigate the progression of subclinical CVD. The participant selection criteria have been previously described.16 Notably, there were no selection criteria based on lung disease, respiratory symptoms or smoking history. MESA was approved by institutional review boards at all collaborating centres, and all participants provided written informed consent for participation.
Lung attenuation was measured on cardiac CT scans performed at baseline. Quantitative image attenuation was measured using a modified version of the Pulmonary Analysis Software Suite at a single reading centre by trained readers. HAA was defined as the volume of imaged lung having CT attenuation values between −600 and −250 Hounsfield units.8 ,9 ILA was visually assessed on full lung CT scans, as previously described.9–11
Of the 6814 MESA participants, there were 6700 with available lipid measurements included in HAA analyses, 2391 in ILA analyses and 1216 in MMP-7 and SP-A analyses, with sampling frame previously described.9 The median (IQR) HAA was 4.2% (3.5%–5.4%) of total imaged lung.
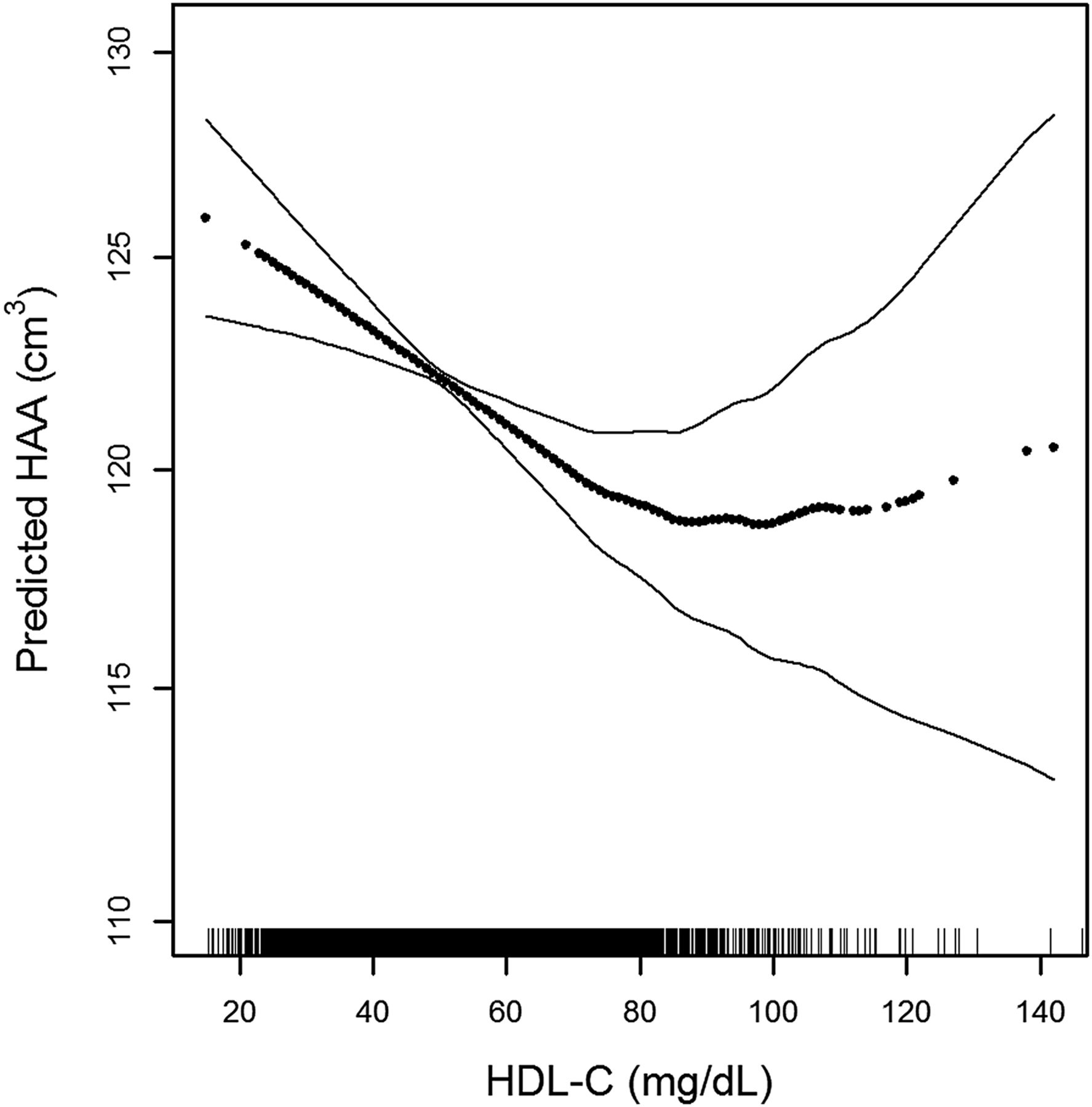
In multivariable-adjusted models, there was a significant association between the presence of coronary artery calcium, HAA and ILA. The presence of coronary artery calcium was associated with 1.47% increment in HAA (95% CI 0.19 to 2.77) and with a 57% greater odds of ILA (OR 1.58, 95% CI 1.18 to 2.08). Greater total cholesterol, HDL-C, LDL-C and triglyceride levels were each associated with lower HAA (table 1). However, the associations of both LDL-C and triglycerides with HAA were greatly attenuated by further adjustment for left ventricular function. On the other hand, the association between greater HDL-C and lower HAA was only marginally changed and remained significant (figure 1). This association also persisted across HDL particle size and for ApoA-1, the major protein component of HDL.
Associations of cholesterol and lipoproteins with high attenuation area (HAA)
{kind=link}
Continuous association between HDL-C and high attenuation areas (HAA) adjusted for age, gender, race/ethnicity, educational attainment, height, body mass index, waist circumference, smoking status, cigarette pack-years, presence of hypertension, presence of diabetes, low-density lipoprotein, triglycerides, C reactive protein, interleukin 6, glomerular filtration rate, statin use, diuretic use, coronary artery calcium, study site, milliampere dose, total volume imaged lung, per cent emphysema on CT, left ventricular ejection fraction and left ventricular end-diastolic mass; p for non-linearity 0.009, p for association <0.001. Dark dotted line is the continuous association. Thin solid lines are the 95% confidence bands. Each point in the graph and each vertical hashmark in the rug plot along the x axis represent one study participant.
In a multivariable-adjusted model, there were no associations of baseline HDL-C, LDL-C, triglycerides, ApoA-1, ApoB, presence of diabetes mellitus, hypertension or statin use with the presence of ILA assessed at 10-year follow-up. In a multivariable-adjusted model (table 2), each SD decrement in HDL-C was associated with a 3.53% increment in MMP-7 (95% CI 0.93% to 6.07%) and a 6.37% increment in SP-A (95% CI 1.35% to 11.13%).
Associations of cholesterol and lipoproteins with MMP-7 and SP-A
Additional analyses are presented in online supplementary tables S1–S9 and figures S1–S2.
In this large cohort of community-dwelling adults, the presence of coronary artery calcium was associated with two measures of subclinical ILD (HAA and ILA), providing further support for a link between CVD and ILD.1–3 We also found that lower plasma HDL-C and ApoA-1 were each associated with greater HAA and greater serum MMP-7 and SP-A levels, independent of smoking, demographic factors, inflammatory biomarkers and measures of left ventricular function, a finding consistent with a previous study that found lower HDL-C levels in 39 adults with pulmonary fibrosis compared with healthy controls.6 Our findings suggest a novel hypothesis that HDL-C levels or its components might exert protective effects in subclinical ILD. Candidate mechanisms by which HDL-C might attenuate subclinical lung inflammation, extracellular matrix remodelling and fibrosis include modulation of endothelial function, protection against inflammation and oxidative stress, and alterations in surfactant function.17–19 ApoA-I has previously been shown to have beneficial effects in reducing lung inflammation and fibrosis in animal models,7 and greater small and medium-size HDL particle concentrations are associated with increased non-cardiovascular, non-cancer chronic inflammation-related deaths in MESA,20 supporting an anti-inflammatory role of small HDL particles in the lungs.
There are several limitations to our study, including the potential for residual confounding, the possibility that HAA likely includes pulmonary oedema, the lack of pathological validation of HAA and the use of cardiac rather than full lung CT scans to measure HAA. In addition, we found that HDL-C was not associated with ILA. This lack of consistency may reflect the 10-year latency period between baseline measurements of lipids and ILA, or it may reflect different stages of disease identified by the two measures of subclinical ILD. Furthermore, the clinical significance of elevated HAA, MMP-7 and SP-A in asymptomatic individuals is uncertain, limiting inferences about the role of HDL-C in fibrotic lung disease.
In summary, we found novel associations of greater HDL-C and ApoA-1 levels with lower HAA, a quantitative CT measure of subclinical lung inflammation and extracellular matrix remodelling, and with biomarkers of lung injury and extracellular matrix remodelling. This finding remains unexplained, but suggests a protective role of lipoproteins in ILD pathogenesis. More work is needed now to elucidate the mechanisms linking these two conditions, and the role that low lipoprotein levels might play in the pathogenesis of ILD.
Acknowledgments
The authors thank the other investigators, the staff and the participants of the Multi-Ethnic Study of Atherosclerosis (MESA) study for their valuable contributions. A full list of participating MESA investigators and institutions can be found at http://www.mesa-nhlbi.org.
References
Footnotes
Twitter Follow David Lederer @davidlederer
Contributors AJP, DJL, RGB, SJS, KW and SMK conceived and designed the study. AJP, GR, MYT, RGB, EAH, FSA, SJS and DJL acquired the data. AJP, SMK, PLE, EP, RS, DR, CJ, RGB, KHS, JJC, DRJ, KW, SJS and DJL analysed the data. AJP drafted the initial manuscript. All authors contributed to the conception and design of the study and to the acquisition, analysis, or interpretation of data. All authors revised the manuscript for important intellectual content. All authors approved the final version of the manuscript. All authors agree to be accountable for all aspects of the work.
Funding The work is funded by the National Institutes of Health contracts HHSN268201500003I, N01-HC-95159, N01-HC-95160, N01-HC-95161, N01-HC-95162, N01-HC-95163, N01-HC-95164, N01-HC-95165, N01-HC-95166, N01-HC-95167, N01-HC-95168 and N01-HC-95169 and grants UL1-TR-000040, UL1-TR-001079, R01-HL-103676, RC1-HL100543, R01-HL-093081, R01-HL-077612, T32-HL-105323 and K24-HL-131937; by the Pulmonary Fibrosis Foundation; and by the Rocco Guinta Research Fund.
Competing interests DJL has received modest consulting fees from Genentech/Roche, Boehringer Ingelheim, Gilead, Pharmakea, Veracyte, Patara Pharmaceuticals, Degge Group and the France Foundation related to IPF. Columbia University has received funding for clinical trials in IPF from Boehringer Ingelheim, Gilead, Bayer and Global Blood Therapeutics. Columbia University has received funding from the Pulmonary Fibrosis Foundation for DJL's consulting services. DJL has received modest fees for serving as a deputy editor for the Annals of the American Thoracic Society and as a statistical editor for Thorax. SMK reports grants from NIH during the conduct of the study and non-financial support from the ATS. He has received personal fees from the European Respiratory Journal for serving on an editorial board. The University of Pennsylvania has received grants from Actelion, United Therapeutics, Gilead, Lung Biotech and Bayer for CME courses. EAH is a founder and shareholder in VIDA Diagnostics, a company commercialising lung image analysis software developed, in part, at the University of Iowa.
Ethics approval Institutional Review Boards at all collaborating centres.
Provenance and peer review Not commissioned; externally peer reviewed.