Article Text

Abstract
Rationale There is no consensus as to when treatment for idiopathic pulmonary fibrosis (IPF) should be initiated. Some physicians prefer not to treat patients with preserved lung volume.
Objective To investigate whether patients with IPF and preserved lung volume receive the same benefit from nintedanib as patients with more impaired lung volume.
Methods Post hoc subgroup analyses of pooled data from the two replicate phase III INPULSIS trials by baseline FVC % predicted (≤90%, >90%).
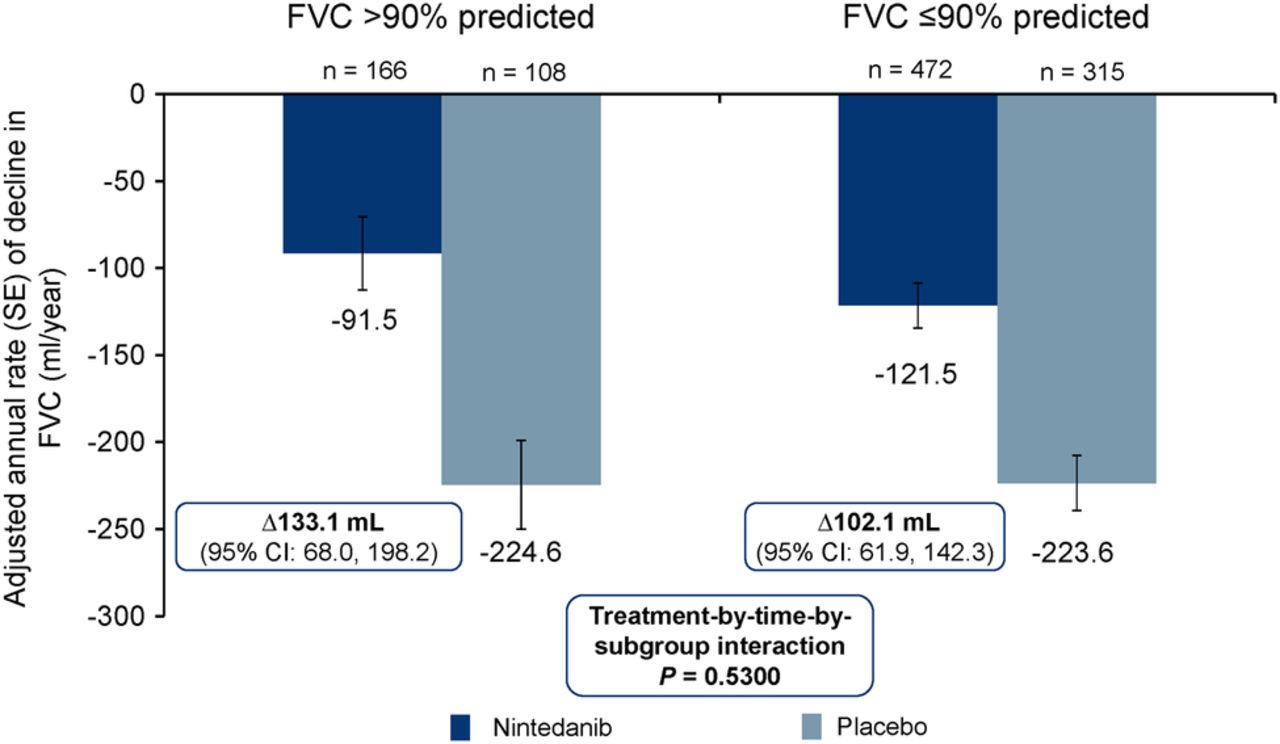
Results At baseline, 274 patients had FVC >90% predicted and 787 patients had FVC ≤90% predicted. In patients treated with placebo, the adjusted annual rate of decline in FVC was consistent between patients with FVC >90% predicted and FVC ≤90% predicted (−224.6 mL/year and −223.6 mL/year, respectively). There was no statistically significant difference between these subgroups in the effect of nintedanib on annual rate of decline in FVC, change from baseline in St George's Respiratory Questionnaire total score or time to first acute exacerbation. In patients with baseline FVC >90% predicted and ≤90% predicted, respectively, the adjusted annual rate of decline in FVC with nintedanib was −91.5 mL/year (difference vs placebo: 133.1 mL/year (95% CI 68.0 to 198.2)) and −121.5 mL/year (difference vs placebo: 102.1 mL/year (95% CI 61.9 to 142.3)). Adverse events associated with nintedanib were similar in both subgroups.
Conclusions Patients with IPF and preserved lung volume (FVC >90% predicted) have the same rate of FVC decline and receive the same benefit from nintedanib as patients with more impaired lung volume.
Trial registration number NCT01335464 and NCT01335477.
- Idiopathic pulmonary fibrosis
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is the key question?
Do patients with idiopathic pulmonary fibrosis (IPF) and preserved lung volume receive the same benefit from nintedanib as patients with more impaired lung volume?
What is the bottom line?
Patients with IPF and FVC >90% predicted at baseline have the same rate of FVC decline and receive the same benefit from nintedanib as patients with more impaired lung volume.
Why read on?
These data provide, for the first time, evidence in a significant subgroup of patients with preserved lung volume to support the concept of offering early treatment to patients with IPF.
Introduction
Idiopathic pulmonary fibrosis (IPF) is a specific form of interstitial pneumonia associated with chronic dyspnoea and cough, and the progressive loss of lung function.1 The clinical course of IPF is variable and difficult to predict, with some patients progressing rapidly, others relatively slowly and some experiencing acute deteriorations in respiratory function that are associated with high morbidity and mortality.2 A decline in FVC reflects disease progression in patients with IPF and is predictive of mortality.3–6 Data from phase II–III trials in patients with IPF and mild or moderate impairment of lung function suggest that the decline in FVC in patients receiving placebo is ∼200 mL/year.7–12
Nintedanib is an intracellular inhibitor of tyrosine kinases13 that has been approved for the treatment of IPF in several countries and regions including the USA, EU, Canada and Japan. Nintedanib received a conditional recommendation for use in the treatment of IPF in the latest international clinical practice guideline.14 The efficacy and safety of nintedanib 150 mg twice daily in patients with IPF were assessed in the two replicate, randomised, placebo-controlled, 52-week, phase III INPULSIS trials (NCT01335464 and NCT01335477).12 In both INPULSIS trials, nintedanib significantly reduced the annual rate of decline in FVC (primary endpoint). A benefit of nintedanib versus placebo on the key secondary endpoints of time to first investigator-reported acute exacerbation and change from baseline in St George's Respiratory Questionnaire (SGRQ) total score over 52 weeks was observed in INPULSIS-2, but not in INPULSIS-1. The adverse events most frequently associated with nintedanib were gastrointestinal events, particularly diarrhoea.12
IPF is commonly described using the terms ‘mild’, ‘moderate’ and ‘severe’, or ‘early’ and ‘advanced’.15 However, there is no standard definition for what constitutes ‘mild disease’ or ‘marginally impaired lung function’ in patients with IPF and no consensus regarding at which point therapy should be initiated or stopped, particularly as no treatment has been shown to provide significant symptomatic benefit. Some national guidelines use thresholds of FVC as a percentage of the predicted value (FVC % predicted) to determine when pharmacological treatment for IPF should be used16 but these are not based on scientific evidence.
The inclusion criteria used in the INPULSIS trials set no upper limit on FVC % predicted. A recently published prespecified subgroup analysis demonstrated a consistent effect of nintedanib in subgroups of patients with FVC ≤ and >70% predicted at baseline.17 In this analysis, we investigated whether patients with IPF and preserved lung volume (FVC > 90% predicted) received the same benefit from nintedanib as patients with greater impairment in lung volume. Some of these results have been reported as an abstract.18
Methods
The design of the INPULSIS trials has been described.12 The clinical trial protocol was approved by an Independent Ethics Committee and/or Institutional Review Board at all the participating centres. All patients provided written informed consent prior to study entry. Eligible patients had been diagnosed with IPF within the previous 5 years and had an FVC ≥50% predicted (no upper threshold), a diffusion capacity of the lung for carbon monoxide (TLCO) 30% to 79% predicted and a FEV1/FVC ratio ≥0.7. Patients were randomised to receive nintedanib 150 mg twice daily or placebo in a 3:2 ratio.
Post hoc analyses in subgroups of patients with baseline FVC >90% versus ≤90% predicted were conducted using pooled data from the two INPULSIS trials. Analyses were conducted in patients who received ≥1 dose of study drug. Analyses were conducted on the primary endpoint (annual rate of decline in FVC) and the key secondary endpoints (time to first investigator-reported acute exacerbation and change from baseline in SGRQ total score) by repeating the primary analysis for each endpoint (described in ref. 12) in each subgroup. The statistical model used for the primary analysis assumed that missing data were missing at random; missing data were not imputed. For the primary endpoint, the terms subgroup and an interaction term treatment-by-time-by-subgroup were included in the model. For the key secondary endpoints, the terms subgroup and an interaction term treatment-by-subgroup were included in the model.
Time to disease progression over 52 weeks, defined as an absolute decline in FVC ≥10% predicted or death, or an absolute decline in FVC ≥5% predicted or death, was assessed using a Cox's regression model with the terms subgroup and an interaction term treatment-by-subgroup included. Safety was assessed through clinical and laboratory evaluation and recording adverse events with onset after the first dose and up to 28 days after the last dose of study drug. Adverse events were coded using the Medical Dictionary for Regulatory Activities (MedDRA), V.16.1. Safety analyses were descriptive.
Results
Patients
A total of 274 (25.8%) patients had baseline FVC >90% predicted (166 treated with nintedanib, 108 treated with placebo) and 787 (74.2%) patients had baseline FVC ≤90% predicted (472 treated with nintedanib, 315 treated with placebo). Baseline characteristics of patients in each subgroup are presented in table 1.
Baseline characteristics by subgroup (mean±SD or n (%))
Compared with patients with FVC ≤90% predicted, patients with FVC >90% predicted had a shorter time since diagnosis, higher TLCO % predicted and lower SGRQ total score (indicating better health-related quality of life), and were more likely to have centrilobular emphysema (based on high-resolution CT scan) and to be female. Within each subgroup, baseline characteristics were similar between the nintedanib and placebo groups.
In the subgroup of patients with baseline FVC >90% predicted, 43 patients (25.9%) in the nintedanib group and 11 patients (10.2%) in the placebo group prematurely discontinued trial medication. In the subgroup of patients with baseline FVC ≤90% predicted, 113 patients (23.9%) in the nintedanib group and 69 patients (21.9%) in the placebo group prematurely discontinued trial medication.
In patients with baseline FVC >90% predicted, mean (SD) duration of exposure was 10.1 (3.6) months and 11.3 (2.0) months in the nintedanib and placebo groups, respectively. In patients with baseline FVC ≤90% predicted, mean (SD) duration of exposure was 10.4 (3.3) months and 10.7 (3.0) months in the nintedanib and placebo groups, respectively.
Annual rate of decline in FVC
In patients with baseline FVC >90% predicted, the adjusted annual rate of decline in FVC was −91.5 mL/year in the nintedanib group and −224.6 mL/year in the placebo group (difference of 133.1 mL/year (95% CI 68.0 to 198.2)) (figure 1). In patients with baseline FVC ≤90% predicted, the adjusted annual rate of decline in FVC was −121.5 mL/year in the nintedanib group and −223.6 mL/year in the placebo group (difference of 102.1 mL/year (95% CI 61.9 to 142.3)) (figure 1). The treatment-by-subgroup interaction p value was not significant (p=0.530), indicating that the treatment effect of nintedanib was not different between the subgroups. The primary endpoint results were supported by the observed changes from baseline in FVC over time in each subgroup (see online supplementary figure S1).

Adjusted annual rate (SE) of decline in FVC (mL/year) by subgroup.
Supplemental material
Disease progression
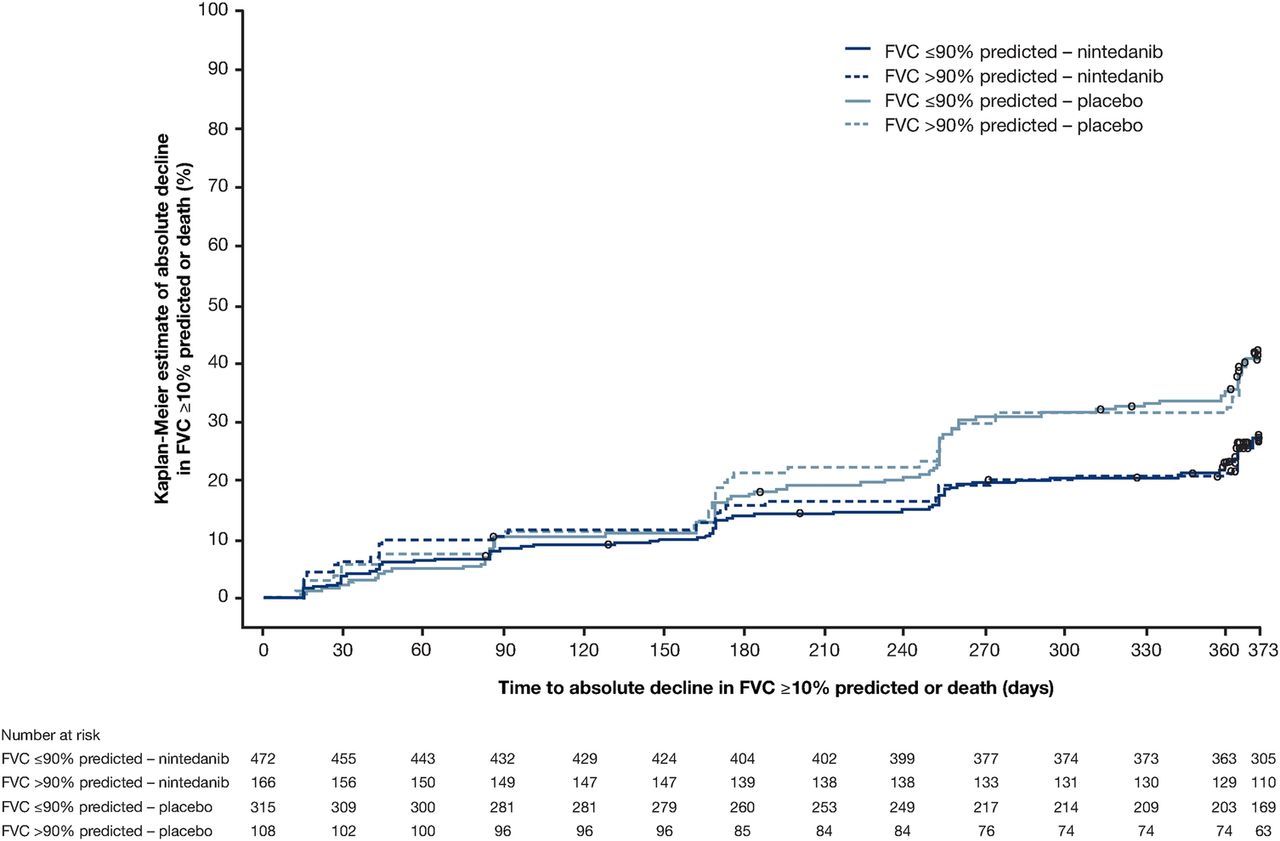
In patients with baseline FVC >90% predicted, the HR for time to an absolute decline in FVC ≥10% predicted or death was 0.59 (95% CI 0.38 to 0.89) in favour of nintedanib (table 2; figure 2). In patients with baseline FVC ≤90% predicted, the corresponding HR was 0.61 (95% CI 0.48 to 0.78) in favour of nintedanib (table 2; figure 2). The treatment-by-subgroup interaction p value was not significant (p=0.830), indicating that the treatment effect of nintedanib was not different between the subgroups by baseline FVC. In both subgroups, most patients who met this endpoint did so based on absolute decline in FVC ≥10% predicted rather than death, but the proportion of patients who died over 52 weeks was higher in patients with FVC ≤90% predicted than >90% predicted at baseline (table 2).
Proportions of patients with disease progression over 52 weeks and HR for time to first event by subgroup

Time to absolute decline in FVC ≥10% predicted or death over 52 weeks by subgroup. HR was 0.59 (95% CI 0.38 to 0.89) in patients with baseline FVC >90% predicted and 0.61 (95% CI 0.48 to 0.78) in patients with baseline FVC ≤90% predicted. Treatment-by-subgroup interaction p=0.830.
In patients with baseline FVC >90% predicted, the HR for time to an absolute decline in FVC ≥5% predicted or death over 52 weeks was 0.67 (95% CI 0.50 to 0.90) in favour of nintedanib; the proportion of patients who met this endpoint was 60.2% in the nintedanib group and 77.8% in the placebo group. In patients with baseline FVC ≤90% predicted, the corresponding HR was 0.59 (95% CI 0.49 to 0.71) in favour of nintedanib (figure 3); the proportion of patients who met this endpoint was 48.7% in the nintedanib group and 69.5% in the placebo group. The treatment-by-subgroup interaction p value was not significant (p=0.486), indicating that the treatment effect of nintedanib was not different between the subgroups by baseline FVC.

Time to absolute decline in FVC ≥5% predicted or death over 52 weeks by subgroup. HR was 0.67 (95% CI 0.50 to 0.90) in patients with baseline FVC >90% predicted and 0.59 (95% CI 0.49 to 0.71) in patients with baseline FVC ≤90% predicted. Treatment-by-subgroup interaction p=0.486.
Acute exacerbations
In patients with baseline FVC >90% predicted, the HR for time to first acute exacerbation was 0.46 (95% CI 0.09 to 2.48) in favour of nintedanib (figure 4); the proportion of patients with ≥1 acute exacerbation was 1.8% in the nintedanib group and 2.8% in the placebo group (three patients in each group). In patients with baseline FVC ≤90% predicted, the HR for time to first acute exacerbation was 0.66 (95% CI 0.39 to 1.11) in favour of nintedanib (figure 4); the proportion of patients with ≥1 acute exacerbation was 5.9% in the nintedanib group and 9.2% in the placebo group (28 and 29 patients, respectively). The treatment-by-subgroup interaction p value was not significant (p=0.956), indicating that the treatment effect of nintedanib was not different between the subgroups.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Time to first acute exacerbation over 52 weeks by subgroup. HR was 0.46 (95% CI 0.09 to 2.48) in patients with baseline FVC >90% predicted and 0.66 (95% CI 0.39 to 1.11) in patients with baseline FVC ≤90% predicted. Treatment-by-subgroup interaction p=0.956.
SGRQ total score
In patients with baseline FVC >90% predicted, the adjusted mean change from baseline in SGRQ total score at week 52 was 2.16 in the nintedanib group and 3.02 in the placebo group (difference of −0.87 (95% CI −3.97 to 2.24)) (see online supplementary figure S2). In patients with baseline FVC ≤90% predicted, the adjusted mean change from baseline in SGRQ total score at week 52 was 4.00 in the nintedanib group and 5.64 in the placebo group (difference of −1.65 (95% CI −3.60 to 0.31)) (see online supplementary figure S2). The treatment-by-subgroup interaction p value was not significant (p=0.3382), indicating that the treatment effect of nintedanib was not different between the subgroups.
Adverse events
A summary of adverse events is shown in online supplementary table S1. The proportions of patients who had ≥1 adverse event or ≥1 serious adverse event were comparable between the nintedanib and placebo groups within each subgroup. A higher proportion of patients had ≥1 serious adverse event in the subgroup of patients with baseline FVC ≤90% predicted than FVC >90% predicted. Adverse events led to premature discontinuation of study drug in 21.7% of nintedanib-treated patients with baseline FVC >90% predicted and 18.4% of patients with baseline FVC ≤90% predicted, compared with 7.4% and 14.6% of placebo-treated patients in these subgroups, respectively. Diarrhoea was the most frequent adverse event in patients treated with nintedanib, reported in 62.0% of patients with baseline FVC >90% predicted and 62.5% of patients with baseline FVC ≤90% predicted, compared with 15.7% and 19.4% of placebo-treated patients in these subgroups, respectively. Diarrhoea led to premature discontinuation of study drug in 4.2% of nintedanib-treated patients with baseline FVC >90% predicted and 4.4% of patients with baseline FVC ≤90% predicted, compared with no and 0.3% of placebo-treated patients in these subgroups, respectively.
Discussion
Our data from the INPULSIS trials have shown for the first time that placebo-treated patients with a baseline FVC >90% predicted have the same rate of FVC decline over the following year as patients with greater impairment in lung volume and the same likelihood of disease progression defined as an absolute decline in FVC % predicted ≥10% or death. It is notable that over 40% of placebo-treated patients with an FVC >90% predicted at baseline, a subgroup that represented over 25% of patients recruited into the INPULSIS trials, reached this disease progression endpoint after 1 year. Furthermore, over 75% of placebo-treated patients with an FVC >90% predicted at baseline had an absolute decline in FVC % predicted of ≥5% after 1 year, suggesting that fewer than one in four patients with preserved lung volume at baseline had stable FVC over the following year. Treatment with nintedanib slowed the annual rate of decline in FVC in patients with FVC >90% and ≤90% predicted to the same extent. These are the first data to show the efficacy of an antifibrotic drug in patients with FVC >90% predicted.
Low or worsening FVC has been shown to be a risk factor for acute exacerbations.19–21 In this analysis, the proportion of patients who had ≥1 acute exacerbation over 52 weeks was higher in placebo-treated patients with FVC ≤90% than >90% predicted (9.2% vs 2.8%). Nintedanib appeared to have the same treatment effect on acute exacerbations in both subgroups, but the interpretation of these data is limited by the low number of acute exacerbations in the subgroup with FVC >90% predicted (six events in 274 patients). No difference was observed between subgroups in the effect of nintedanib in change in SGRQ total score, which was small in both subgroups, consistent with the overall patient population.
Data from the INSIGHTS-IPF registry of patients with IPF in clinical practice in Germany showed that patients with less severe impairment in FVC are less likely to be receiving treatment.22 However, the earlier that patients with IPF receive treatment, the more lung function remains to be preserved. Further, the clinical course of IPF in an individual patient is unpredictable; patients' pulmonary function may decline rapidly shortly after presentation6 ,23 and acute exacerbations can occur at any point.1 It should also be noted that patients with IPF whose lung function appears to be almost normal based on FVC % predicted may already have lost a substantial amount of functional lung tissue. Given the method used to calculate FVC % predicted,24 some individuals will have had an FVC % predicted some way above 100% before developing IPF. The presence of emphysema, a common comorbidity in patients with IPF,25 also increases FVC, presumably by mitigating the impact of fibrosis on ventilatory physiology.26
Our data argue against a ‘watch and wait’ approach for the treatment of IPF and support the importance of prompt diagnosis of IPF to enable patients to receive treatment to slow disease progression as soon as possible.27 ,28 Data from the CAPACITY and ASCEND trials of pirfenidone have also demonstrated a consistent effect of treatment across subgroups of patients by FVC % predicted (≤65, 65–80, >80%) at baseline, although patients with FVC >90% predicted were not eligible for the ASCEND study.29 However, it should be noted that the subgroup analyses of both the nintedanib and pirfenidone trials are based on group averages and these subgroups likely included a number of patients who had no FVC decline during the study period that could be stabilised with therapy. Other limitations include the short duration of treatment, considering that IPF is a chronic disease that may require treatment for longer than 1 year, and premature discontinuation of study medication in 22% of patients, consistent with treatment discontinuations seen in other clinical trials in patients with IPF with a treatment duration of similar length.11 ,30
A concern might be raised that commencing treatment with nintedanib earlier in the course of IPF might increase the risk that patients would become resistant to the effects of the drug. However, to date, there is no experimental or clinical evidence to suggest the development of resistance to nintedanib in patients with IPF. Indeed, the specificity of nintedanib against growth factor receptors involved in antiangiogenesis (ie, the fibroblast growth factor, platelet-derived growth factor and vascular endothelial growth factor receptors),31 together with its antiproliferative activity on fibroblasts prone to secrete growth factors,32 argues against potential for treatment resistance.33 An interim analysis of INPULSIS-ON, the open-label extension of the INPULSIS trials, has shown that the decline in FVC in patients continuing nintedanib in INPULSIS-ON was similar to the decline in FVC in patients treated with nintedanib in INPULSIS, suggesting that the effect of nintedanib on slowing disease progression is maintained for at least 3 years.34
In conclusion, in this analysis of pooled data from the INPULSIS trials, the annual rate of decline in FVC was similar in placebo-treated patients with preserved lung volume (FVC >90% predicted) at baseline as in patients with greater impairment in lung volume. Nintedanib slowed the decline in lung function independent of the degree of FVC impairment at baseline, with a similar adverse event profile in both subgroups. These findings support the concept of offering treatment to patients with IPF and preserved lung volumes at the time of diagnosis, until there are markers that predict individual disease course.
Acknowledgments
Medical writing assistance, supported financially by Boehringer Ingelheim, was provided by Julie Fleming and Wendy Morris of Fleishman-Hillard Group, London, UK, during the preparation of this article. The authors were fully responsible for all content and editorial decisions, and were involved at all stages of manuscript development and have approved the final version.
References
Footnotes
Contributors All the authors except WT were involved in the study design. All the authors were involved in analysis or interpretation of data and revising the manuscript for important intellectual content. All the authors have approved the final version of the manuscript.
Funding The INPULSIS trials were funded by Boehringer Ingelheim. Boehringer Ingelheim was involved in the study design, in the analysis and interpretation of the data and in the writing of this manuscript.
Competing interests MK reports receipt of grants and personal fees from Boehringer Ingelheim and Roche; personal fees from GlaxoSmithKline, Gilead, AstraZeneca, ProMetic and Genoa; and grants from Actelion, Respivert, the Canadian Institute for Health Research and the Canadian Pulmonary Fibrosis Foundation. LR reports receipt of grants and personal fees from Boehringer Ingelheim for being a member of the INPULSIS steering committee and co-principal investigator of the trials; grants and personal fees from InterMune for being a member of an advisory board; personal fees from MedImmune (advisory board member), Biogen Idec (consulting), Sanofi-Aventis (consulting), Roche (advisory board member), Takeda (advisory board member), ImmuneWorks (consulting), Shionogi (speaker honoraria) and GlaxoSmithKline (advisory board member). JB reports serving as an ILD expert for the current international IPF guidelines; serving as Chair or member of the steering committees for the Panorama, BUILD-3, Artemis-IPF, Artemis-PH and RISE-IIP clinical trials; receipt of grants and personal fees from Actelion and InterMune; and personal fees from Boehringer Ingelheim, Grünenthal, Gilead, Bayer, Roche and GlaxoSmithKline. TMM reports receipt of grants and personal fees from GlaxoSmithKline (advisory board member); grants from Novartis; grants and non-financial support from UCB; non-financial support from Takeda; personal fees from Boehringer Ingelheim, InterMune, Lanthio, Sanofi-Aventis, AstraZeneca, Roche, Bayer, Biogen Idec, Cipla, DOSA, ProMetic and Galapagos; and serving as an investigator in an ongoing Gilead phase 2b study. WT, SSt and CH are employees of Boehringer Ingelheim. RMdB has served as a steering committee member for Boehringer Ingelheim and InterMune, and as an advisory board member for GlaxoSmithKline and Actelion.
Ethics approval The clinical protocol was approved by an independent ethics committee or institutional review board at each participating centre.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves