Article Text

Abstract
Background Cured meat intake—a recent carcinogenic factor—may increase the risk of COPD, but its association with asthma remains unknown. Though body mass index (BMI) is a likely risk factor for asthma, its role in the diet–asthma association as a mediator has never been studied. We investigated the association between cured meat intake and worsening asthma symptoms in adults, and the role of BMI as a potential mediator.
Methods Using data from the French prospective EGEA study (baseline: 2003–2007; follow-up: 2011–2013), we applied a mediation analysis in the counterfactual framework, a marginal structural model (MSM), to estimate the direct effect of baseline cured meat intake (<1, 1–3.9, ≥4 servings/week) on change in asthma symptom score (worsening or not), and the indirect effect mediated by BMI.
Results Among the 971 participants (mean age 43 years; 49% men; 42% with asthma), 20% reported worsening asthma symptoms during the mean follow-up time of 7 years. Using the MSM, we reported a positive direct effect of cured meat intake on worsening asthma symptoms (multivariable OR=1.76, 95% CI 1.01 to 3.06 for ≥4 vs <1 serving/week). We also reported an indirect effect mediated by BMI (OR=1.07; 95% CI 1.01 to 1.14), accounting for 14% of the total effect.
Conclusions Higher cured meat intake was associated with worsening asthma symptoms over time, through a direct effect and to a lesser extent an effect mediated by BMI. This research extends the effect of diet on asthma in adults.
- Asthma
- Asthma Epidemiology
Statistics from Altmetric.com
Key messages
What is the key question?
Is high cured meat intake, a risk factor for several diseases, associated with worsening asthma symptoms in adults? Does body mass index (BMI) act as a mediator in this association?
What is the bottom line?
Correctly accounting for the BMI as a mediator, this paper shows that high cured meat intake was associated with worsening asthma symptoms over time, through a direct effect and to a lesser extent an effect mediated by BMI.
Why read on?
This paper is not only the first prospective study on the association between cured meat intake and asthma symptoms, it is also the first application of newly developed methods to estimate the role of BMI as a mediator in the diet–asthma association.
Introduction
Cured meat, an important component of the Western diet, has recently been classified as carcinogenic by WHO.1 High cured meat intake is a risk factor not only for cancer,2 but also for several chronic diseases3 ,4 and all-cause mortality.3 The deleterious health effects of high cured meat intake have been increasingly observed. Regarding lung health, frequent cured meat intake is associated with lung cancer,2 ,5 ,6 decreased lung function7 ,8 and COPD symptoms,6 ,7 exacerbations9 or incidence.10 ,11 As cured meat is known for its high-nitrite content12 which may lead to nitrosative stress related airway inflammation—one of the several physiological processes involved in asthma,13 it is reasonable to posit that cured meat intake is an independent risk factor for asthma. To our knowledge, only two studies—both performed in the USA—have investigated the association between cured meat intake and the risk of adult-onset asthma, and they reported no significant association after adjustment for body mass index (BMI) and other confounders.10 ,11
Since obesity is a likely risk factor for incidence and exacerbations14–16 of asthma, one challenge when investigating the association between diet and asthma is to properly account for BMI. As diet affects BMI, it is plausible that BMI lies in the causal pathway between diet and asthma.17 Thus the classical way, in which we consider BMI as a confounder in the analysis and adjust for BMI, may over adjust the diet–asthma association due to the likely mediating role of BMI.17 ,18 Recently, mediation analyses in the counterfactual framework have been proposed to disentangle direct and indirect effects.19–21
Asthma is a complex disease, with strong clinical phenotypic heterogeneity and temporal phenotypic variability. Whereas the doctor-diagnosed incidence of asthma is widely used, there have been increasing concerns about its limitations, particularly due to the dichotomous assumption of asthma.22 Recently, an asthma symptom score has been proposed to study risk factors for asthma in longitudinal studies.23 ,24 Being a multi-categorical measure, the score provides more power to detect risk factors for asthma incidence and asthma control.23 ,24 Moreover, the asthma symptom score detects the change in asthma symptoms over time, reflecting either asthma incidence, or captures the temporal variability of the disease among participants with asthma—remission, relapse or persistence.23 Given that previous studies showed weak association between dietary factors and adult-onset asthma incidence,25 the asthma symptom score might be particularly relevant to studying the role of dietary factors as an aetiological risk factor and as a disease modifier.26
In the current study, we aimed to investigate the association between cured meat intake and the change in asthma symptom score in a French prospective study of adults, and to assess the role of BMI as a mediator using a counterfactual approach to mediation analysis.
Methods
Study sample
The EGEA study (Epidemiological study on the Genetics and Environment of Asthma, bronchial hyperresponsiveness and atopy) is a longitudinal study with an initial group of asthma cases, their first-degree relatives, and a group of controls, followed up over 20 years (https://egeanet.vjf.inserm.fr/index.php/fr/). Protocol and descriptive characteristics of the EGEA study have been previously published.27 ,28 Briefly, 2047 participants from five cities in France were enrolled between 1991 and 1995. Between 2003 and 2007, this population was contacted for the second survey (EGEA2). Out of 2002 participants alive, 1845 completed a short self-administered questionnaire and 1601 had a complete medical examination (among whom 715 (42%) ever had asthma). As a follow-up study of EGEA2, the third survey (EGEA3) was performed between 2011 and 2013 using a self-completed questionnaire, and 1558 questionnaires were returned.
Since diet was measured at EGEA2 only, we used data collected at EGEA2 as baseline and EGEA3 as the follow-up. Out of the 1601 participants from EGEA2, 35 adolescents (<16 years old) were first excluded. Among adults (n=1566), we excluded 330 participants who did not complete the food frequency questionnaire, had an inadequate assessment of diet, or had an implausibly high or low total energy intake.29 Ten participants with missing data for the asthma symptom score were further excluded. Among the 1226 remaining, 185 (15%) were lost to follow-up; compared with participants lost to follow-up (n=185), participants followed at EGEA3 (n=1041) were less likely to be men or smokers, and were similar regarding age, BMI, educational level, physical activity and asthma status (see online supplementary table S1). After excluding 70 participants out of 1041 with missing data for the asthma symptom score assessed at EGEA3, the final study sample included 971 participants (figure 1).
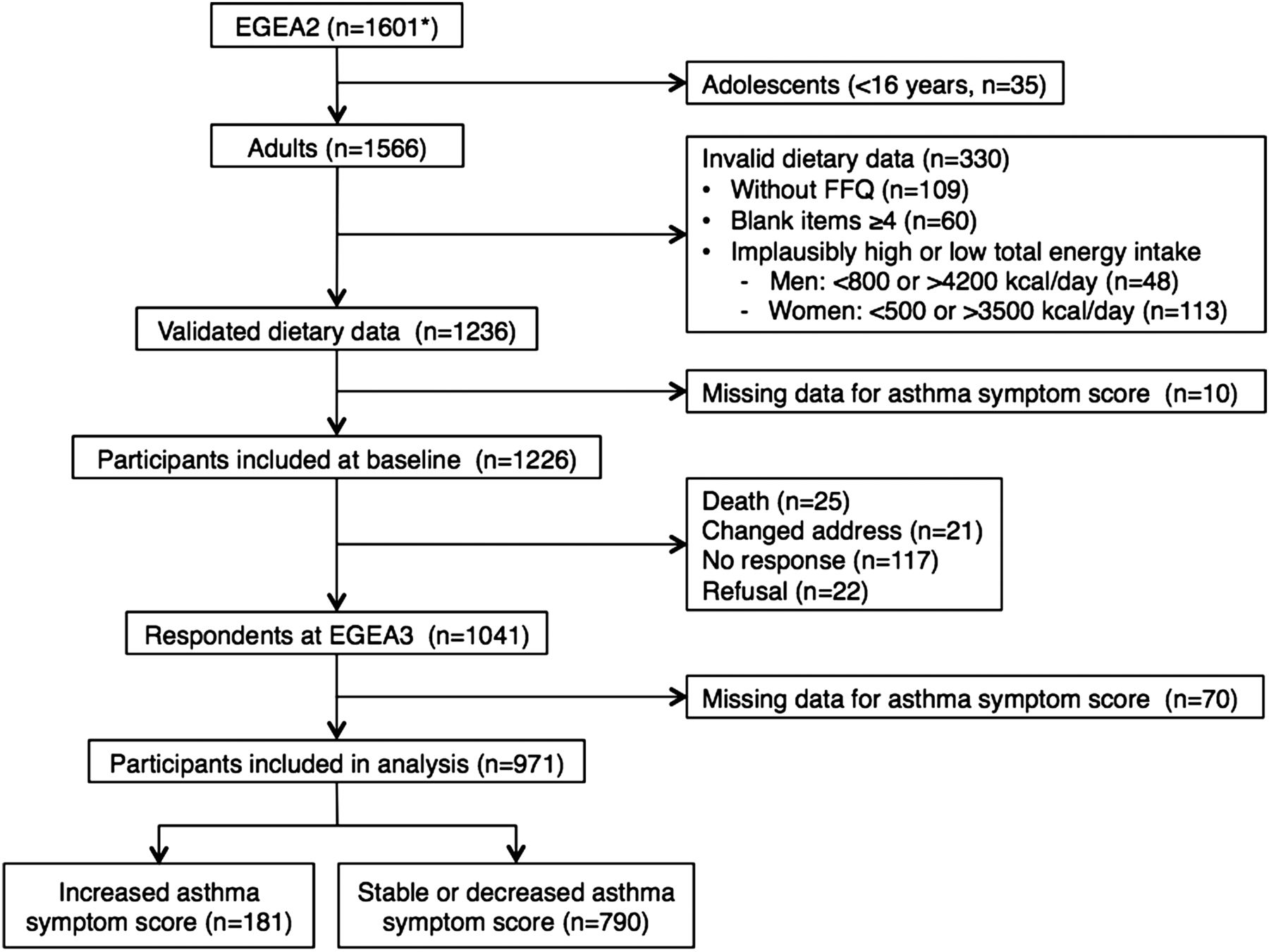
Flowchart for inclusion of participants. *Among the 1601 participants, 715 (45%) had ever asthma. FFQ, food frequency questionnaire.
supplementary data
Among adults, excluded participants (n=595) were similar compared with participants included in the analysis (n=971) regarding age, BMI, physical activity, sex, smoking and asthma status, but they were more likely to have a lower educational level (see online supplementary table S2).
Ethical approval was obtained from the relevant institutional review board committees (Cochin Port-Royal Hospital and Necker-Enfants Malades Hospital, Paris). All participants provided written informed consent.
Dietary intakes
At EGEA2, we used a 118-item food frequency questionnaire based on a French validated dietary questionnaire30 to assess average dietary intakes during the previous 12 months. These 118 items were grouped into 46 food groups and average intake was calculated for each group.29 The French food composition table from the SU.VI.MAX survey was used to calculate the nutrient intakes and total energy intake (kcal/day).31 The cured meat group included three items: ham (2 slices/portion), sausage (1/portion) and dried sausage (2 slices/portion). According to the distribution of cured meat intake, exposure was categorised in three classes: <1 serving/week (lowest; 19%), 1–3.9 servings/week (medium; 48%) and ≥4 servings/week (highest; 33%). The group with the lowest intake was considered as ‘non-exposed’ and was taken as the reference group.
To account for the overall remaining effect of diet in the cured meat–asthma association, analyses were adjusted for dietary patterns derived from all food groups except cured meat. In the EGEA study, two dietary patterns were previously identified using confirmatory factor analysis (CFA) on the 46 food groups: (1) a prudent pattern characterised by a high intake of vegetables, fruits, oils, whole grain cereals and fish; and (2) a Western pattern loaded by a high consumption of prepared meals, French fries, cured meat, condiments, alcohol, beer/cider, sandwiches and potatoes.29 In the current analysis, we derived a ‘modified Western pattern’ and a prudent pattern using CFA on 45 food groups (all food groups except cured meat, see online supplementary table S3). The individual scores obtained from CFA for the two dietary patterns were used as potential confounders in the analysis.
Asthma symptom score
The asthma symptom score has been proposed as a continuous measure to study risk factors for asthma in longitudinal studies. Compared with a dichotomous definition of asthma, increased power in the analysis identifying risk factors was suggested when using the asthma symptoms score.23 ,24 In the EGEA study, the asthma symptom score was calculated both at EGEA2 and EGEA3. Ranging from 0 to 5, the score is based on the number of respiratory symptoms during the past 12 months reported in the questionnaire: (1) breathless while wheezing; (2) woken up with chest tightness; (3) attack of shortness of breath at rest; (4) attack of shortness of breath after exercise; and (5) woken by attack of shortness of breath. Change in asthma symptom score was categorised as ‘stable or improved’ if EGEA3 score–EGEA2 score ≤0, and ‘worsening’ if EGEA3 score–EGEA2 score >0.
Body mass index
Weight and height of participants were measured at EGEA2. BMI (kg/m2) at EGEA2 was calculated as weight/height2 and was categorised into five classes: <22.5, 22.5–24.9, 25–27.4, 27.5–29.9, ≥30.
Other variables
Age, sex, smoking status (never and ever smoking), educational level, and physical activity were assessed at baseline (EGEA2). Educational level was categorised into two classes depending on whether the participants had higher education (university or equivalent). Leisure-time physical activity was assessed in metabolic equivalents per week (METs/w) taking into account a variety of intensive activities (such as jogging, aerobic, swimming, cycling, tennis, soccer, digging in the garden), moderate activities (such as cleaning, walking, golf, slight gardening), and light activities (such as reading, watching TV, office work, driving, eating). Average physical activity was estimated by summing the product of average active time per week and the metabolic equivalent value of each activity.
Due to the case-control design of the EGEA study, the study population was enriched with participants with asthma. To take into account this study design, ever asthma was considered as a covariate in analysis. Ever asthma was defined by being recruited as an asthma case in chest clinics at EGEA1 or responding positively to at least one of the two questions at EGEA1 or EGEA2: (1) ‘Have you ever had attacks of breathlessness at rest with wheezing?’ and (2) ‘Have you ever had asthma attacks?’ Never asthma was defined by absence of asthma at EGEA1 and EGEA2.
Statistical analysis
We used a direct acyclic graph to represent our mediation model (figure 2). Age (continuous), sex, smoking status (never/ever), educational level (low/high (ie, university or equivalent)), leisure-time physical activity (expressed in metabolic equivalents/week, continuous), dietary patterns, total daily energy intake, and asthma status at EGEA2 were considered as potential confounders.
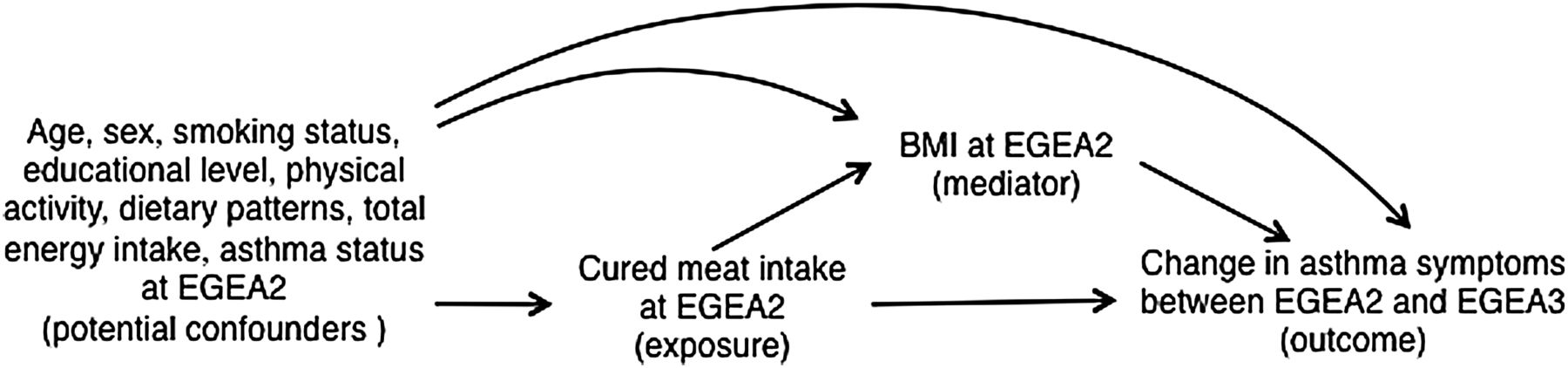
Direct acyclic graph of the proposed mediation model.
Several methods with practical implementation have been recently proposed to disentangle the natural direct and indirect effects in the counterfactual framework.19–21 In the current analysis, we applied the marginal structural model proposed by Lange and colleagues,20 which has been described as a simple approach and can be implemented in standard software for almost any variable type. Detailed implementation of this method is described in the online supplementary methods. As previously described,19 ,20 several conditions are required to apply such methods, and we assumed that they were satisfied (see online supplementary methods).
To evaluate how much of the total effect was due to the effect of BMI, we calculated the ‘proportion explained’ by BMI as (ORTE−ORNDE)/(ORTE−1), where ORTE and ORNDE were respectively the OR of total effect and natural direct effect.32 The total effect was calculated as ORNDE×ORNIE, where ORNIE denoted the natural indirect OR.
We tested potential interactions between cured meat intake and BMI in the association with asthma.20 In addition, since cured meat intake is usually higher in men than in women,33 ,34 and often associated with smoking habit,35 we conducted sensitivity analyses stratified on sex and smoking status, and formally tested interactions of cured meat intake with sex and smoking. Furthermore, considering the case-control design of EGEA study, we also performed a stratified analysis on asthma status at EGEA2.
As a sensibility analysis, we replicated our results using another method of mediation analysis in the counterfactual framework, a two-stage regression model, which provides estimation of total effect and SEs using bootstrapped samples19 (see online supplementary methods for details).
All analyses were performed using SAS V.9.3 (SAS Institute Inc., Cary, North Carolina, USA).
Results
Description of population
The study sample was comprised of 971 participants. The mean age was 43 years and 49% were men. At EGEA2, 42% participants had ever asthma, 51% were never smokers, 35% were overweight and 9% were obese. The median cured meat intake was 2.5 (Q1–Q3: 1.5–4.5) servings/week.
Baseline characteristics of the participants according to cured meat intake are presented in table 1. Compared with participants with the lowest intake (<1 serving/week) of cured meat, participants with the highest intake (≥4 serving/week) were younger (p<0.001), more likely to be men (p<0.001) and smokers (p=0.04), to report a higher total energy intake (p<0.001), and to have ever asthma (p=0.03); as expected, they also consumed more sodium (p<0.001) and saturated fat (p<0.001). Besides, participants who had a higher intake of cured meat were more likely to be in a higher BMI category (p=0.01).
Characteristics for participants at baseline (EGEA2) according to cured meat intake (n=971)
Cured meat intake and change in asthma symptom score
At EGEA3, after a mean follow-up time of 7 years (ranging from 5 to 9 years), 513 participants (53%) reported the same asthma symptom score as EGEA2 (stable), 191 (20%) reported more symptoms (worsening), and 267 (27%) had fewer symptoms (improved). The proportion of participants with worsening asthma symptoms was 14%, 20% and 22% respectively among those who ate <1, 1–3.9 and ≥4 servings/week of cured meat (p for trend=0.04).
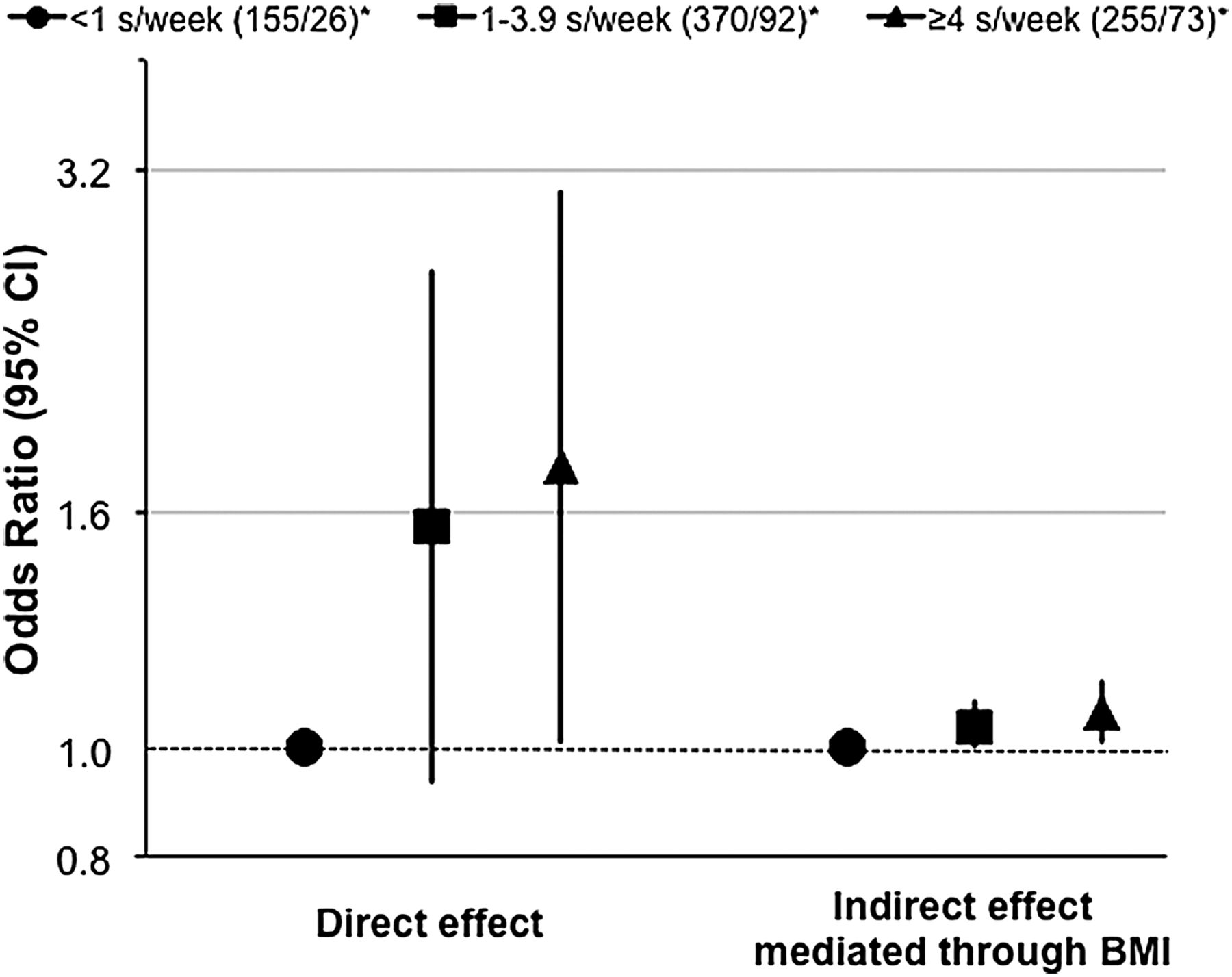
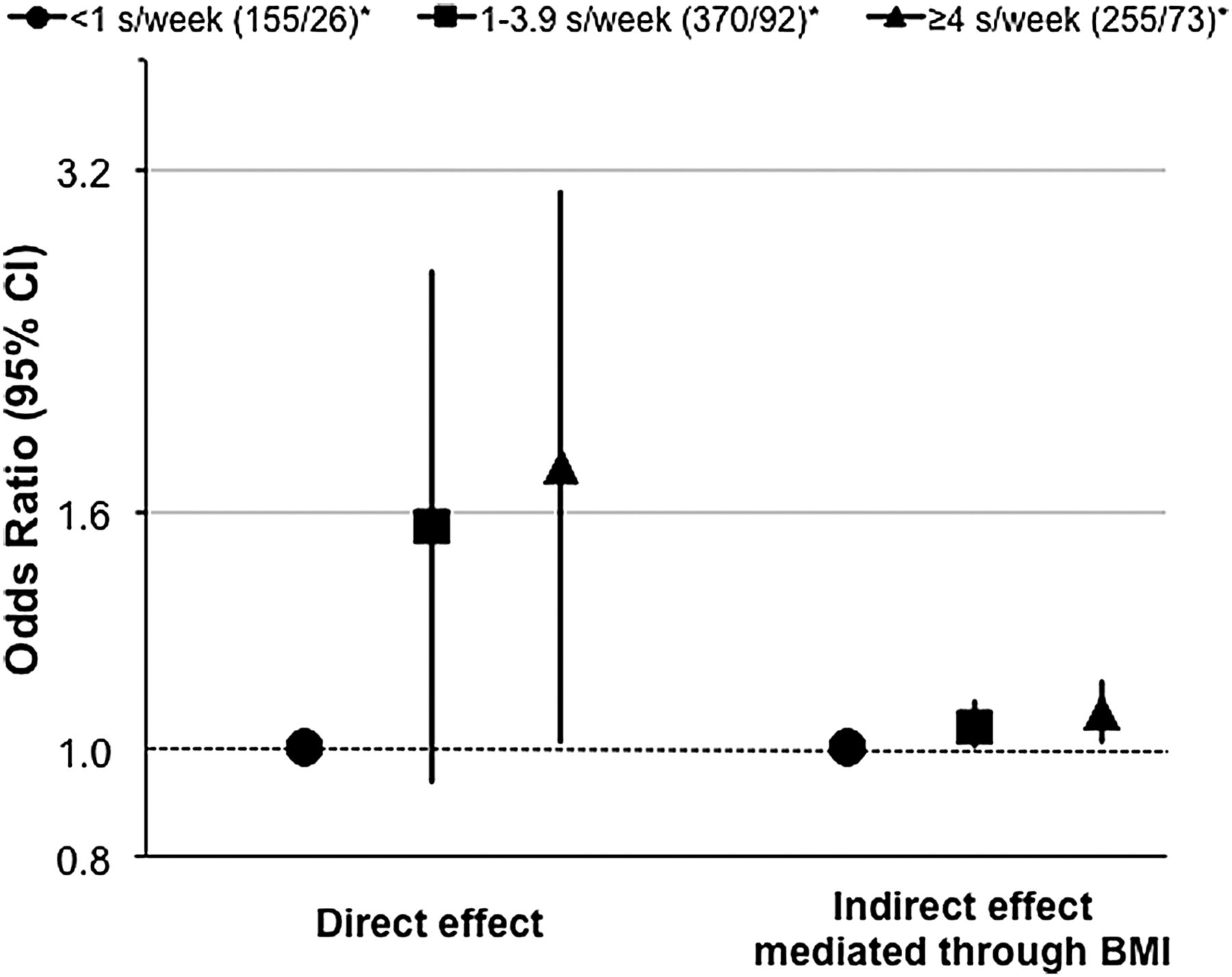
Results of mediation analyses using the marginal structural model are presented in table 2. Among all the participants, after adjustments for age, sex, smoking, educational level, physical activity, dietary patterns, total energy intake, and asthma status, we observed a positive direct effect of cured meat intake on worsening asthma symptoms: the OR was 1.76 (95% CI 1.01 to 3.06) when comparing the highest with the lowest intake. We also reported a positive indirect effect mediated by BMI: the adjusted OR was 1.07 (95% CI 1.01 to 1.14) when comparing the highest to the lowest intake (figure 3). The percentage mediated by BMI of the association was 14%. No interaction was observed between cured meat intake and BMI (p for interaction=0.90) in the associations with asthma. We formally tested interactions for total effect between cured meat intake with sex (p for interaction=0.50), smoking status (p for interaction=0.60), and asthma status (p for interaction=0.50). When we performed stratified analyses according to sex, smoking, and asthma status, results were similar in all subgroups (OR>1), although the power was limited (table 2).
Direct and indirect effects of cured meat intake on worsening asthma symptoms between EGEA2 and EGEA3, using the marginal structural model (n=971)
{kind=link}
{kind=link}
{kind=link}
Direct and indirect effects of cured meat intake on worsening asthma symptoms between EGEA2 and EGEA3, using the marginal structural model (n=971). We adjusted for age, sex, smoking status, educational level, leisure-time physical activity, modified Western and prudent patterns, total energy intake, and asthma status at EGEA2. *Numbers of participants (stable or improved/worsening). s/week, serving/week.
Analyses using another method of mediation analysis in the counterfactual framework yielded similar results to those obtained through the marginal structural model (see online supplementary tables S5 and S6).
Discussion
In this French prospective study of adults, using mediation analysis in the counterfactual framework, we reported a positive association between high cured meat intake (≥4 serving/week) and worsening asthma symptoms over time. While the indirect effect mediated through BMI accounted for only 14% of this association, the direct effect explained a greater proportion, suggesting a deleterious role of cured meat independent of BMI.
Diet is highly influenced by culture as well as geographical, environmental and socioeconomic factors. In our study, cured meat food group included three typical French cured meats—ham, sausages and dried sausage. The mean intakes of cured meats in the EGEA study were similar to those reported by the French National Individual Survey on Food Consumption 2006–2007.34 The EGEA results are in agreement with previous researches indicating a harmful association between cured meat intake and different measures of lung health in several countries, where the types and preparation of cured meats may be different.5–9 However, two large prospective American studies,10 ,11 with different types of cured meat (mainly bacon, hot dogs and sausages), reported that cured meat intake may increase the risk of newly diagnosed COPD, but not the risk of incident asthma, after adjustment for BMI and other potential confounders. This different finding may result from the role of BMI in the association (confounder vs mediator) or the assessment of respiratory phenotypes (incidence vs change in asthma symptoms).
In the present study, BMI was taken into account as a mediator rather than a confounder. The modification of dietary habits, the obesity epidemic, and the decrease in physical activity have been suggested to play a role in the increase of asthma worldwide during the last decades.36 Overweight and obesity reflect an imbalance between energy provision (ie, intake of calories) and expenditure (ie, physical activity), so the interrelations between these factors make it difficult to disentangle their separate roles on asthma, and to identify confounders and mediators in the diet–asthma association.17 To date, the adjustment for BMI has been widely used when investigating the role of nutritional factors in obesity-related diseases. Previous studies have consistently suggested a dose-dependent association between BMI and the risk of asthma incidence and control,14–16 indicating that obesity is a likely mediator in the diet–asthma association. The traditional BMI-adjusted method could over adjust the association and lead to biased results. Mediation analysis in the counterfactual framework allows taking into account BMI correctly in such an association. Moreover, it provides a quantitative measure of the proportion mediated through a given mediator, which could help us to better understand the observed association. To the best of our knowledge, this is the first application of newly developed methods for mediation analysis to estimate the association between cured meat intake and asthma.
Accounting for BMI as a mediator, we reported an overall positive association between high cured meat intake and worsening asthma symptoms. The indirect effect mediated through BMI accounted for only 14% of the total effect, supporting the hypothesis that the cured meat–asthma association is related to other mechanisms. Several potential mechanisms were proposed by previous studies involving biological markers. First, cured meats are rich in nitrite, which may lead to nitrosative stress13 and oxidative stress37 related lung damage and asthma. Second, the positive relation between cured meat intake and C-reactive protein38 indicated that cured meat might increase the systemic inflammation, which may have an influence on asthma. In addition, the high content of salt and saturated fat in cured meat might also contribute in part to the association with asthma, though existing evidence has been mainly for childhood-onset asthma.39 Further studies need to be carried out to improve our understanding regarding potential mechanistic processes.
Besides the BMI issue (mediator vs confounder), we have used, unlike the previous studies,10 ,11 an asthma symptom score instead of incident doctor-diagnosed adult-onset asthma. Studies on incidence assume that the disease is a true dichotomous entity, which might be inappropriate in asthma for several reasons: (1) asthma is a complex disease, with strong clinical phenotypic heterogeneity and temporal phenotypic variability in both adults and children;40 ,41 (2) asthma develops over a long period of time with preclinical status difficult to define; and (3) asthma has a low incidence in adults and different epidemiological definitions of asthma exist. These characteristics of asthma might lead to misclassification and biased association estimates.22 Without making the dichotomous assumption of the asthma status, the asthma symptom score captures temporal variability of asthma and allows assessment of the disease progression in longitudinal studies,23 and it is a more powerful tool to investigate risk factors for asthma. Furthermore, the asthma symptom score was shown to have increased specificity and positive predictive value compared with self-report ever asthma or bronchial hyperresponsiveness;23 and the asthma symptom score at baseline has been associated with markers of asthma but not those of COPD at follow-up.24 In participants with asthma, worsening symptoms capture relapse or exacerbation of the disease, and in participants without asthma, worsening symptoms coincide with the asthma incidence and activity. While the asthma symptom score was developed and validated in a general population,23 ,24 our results were obtained in a population among which 42% had ever asthma. Although previous research has suggested that diet could be a modifier of asthma control rather than an aetiological risk factor for incidence of asthma,26 we did not observe interaction between cured meat intake and asthma status at EGEA2 on the association with worsening symptoms. The stratified analysis according to asthma status at EGEA2 showed similar effects in participants with ever asthma. Further studies are needed to clarify potential differences related to asthma status in the effect of cured meat intake on worsening asthma symptoms.
Because people consume complex meals rather than isolated food/nutrients that might interact with each other, the association between cured meat intake itself and the asthma symptom score is difficult to assess and may be partly due to the confounding by other food groups.25 Therefore we adjusted the associations for scores of dietary patterns. The total, direct and indirect effects remained after adjustment for these dietary scores. We acknowledge that findings might not be generalisable to populations with completely different diet habits, such as infrequent cured meat intake and very different food consumptions. The association between cured meat intake and the asthma symptom score may also be due, in part, to a residual confounding by cigarette smoking.42 To minimise this possibility, we performed a stratified analysis according to smoking status and yielded comparable results in never smokers, although we faced a statistical power issue. Additionally, since cured meat intake has been suggested as a risk factor for COPD,10 ,11 the potential overlap between COPD and asthma might contribute to the association between high cured meat intake and asthma. Nevertheless, the overlap between COPD and asthma is less likely in the current study because (1) comparable results were obtained among never smokers; (2) the EGEA study was initiated as a case-control study of asthma with cases recruited in hospital, with childhood asthma and adult-onset asthma;27 ,28 and (3) the use of the asthma symptom score reduces the possibility of this overlap.24 We acknowledge that our definition of ‘non-exposed’ group (<1 serving/week) was not ideal. Due to the limited number of non-eaters of cured meat in the EGEA study, we faced a statistical power issue in subgroup analyses. We acknowledge that 15% of the participants were lost to follow-up. However, most of the characteristics were similar among included and lost to follow-up participants, except for sex and smoking status (as expected, more men and more smokers were lost to follow-up). We also acknowledge that a deterministic approach was used to deal with missing data for asthma symptom score (7% participants). Similar to any other observational study, however, we were able to adjust for many potential confounders due to the extended information available in our study; the validity of the results relies on the assumption of no unmeasured confounding.43 Besides, we acknowledge that recall bias could exist as data from questionnaires were used.
In summary, correctly accounting for BMI as a potential mediator in the diet–asthma association, higher cured meat intake was associated with worsening asthma symptoms over time, not only through an indirect effect mediated by BMI but also a greater direct effect. This research extends the deleterious effect of cured meat in health, and the effect of diet on asthma in adults, and provides a novel analytic approach regarding the role of BMI in the diet–asthma association.
Acknowledgments
We thank Professor Serge Hercberg who provided the nutrients database from the SU.VI.MAX survey; Katelle Joly, Anne Forhan and Peggy Drouillet for computation of the nutrients in the EGEA2 survey. We also thank all those who participated in the study setting, the EGEA cooperative group. They are as follows. Coordination: V Siroux (epidemiology, PI since 2013); F Demenais (genetics); I Pin (clinical aspects); R Nadif (biology); F Kauffmann (PI 1992–2012). Respiratory epidemiology: Inserm U700, Paris: M Korobaeff (EGEA1), F Neukirch (EGEA1); Inserm U707, Paris: I Annesi-Maesano (EGEA1–2); Inserm CESP/U1018, Villejuif: F Kauffmann, N Le Moual, R Nadif, MP Oryszczyn (EGEA1–2), R Varraso; Inserm U823, Grenoble: V Siroux. Genetics: Inserm U393, Paris: J Feingold; Inserm U946, Paris: E Bouzigon, F Demenais, MH Dizier; CNG, Evry: I Gut (now CNAG, Barcelona, Spain), M Lathrop (now University McGill, Montreal, Canada). Clinical centres: Grenoble: I Pin, C Pison; Lyon: D Ecochard (EGEA1), F Gormand, Y Pacheco; Marseille: D Charpin (Egea1), D Vervloet (Egea1-2); Montpellier: J Bousquet; Paris Cochin: A Lockhart (EGEA1), R Matran (now in Lille); Paris Necker: E Paty (EGEA1–2), P Scheinmann (EGEA1–2); Paris-Trousseau: A Grimfeld (EGEA1–2), J Just. Data and quality management: Inserm ex-U155 (EGEA1): J Hochez; Inserm CESP/U1018, Villejuif: N Le Moual; Inserm ex-U780: C Ravault (EGEA1–2); Inserm ex-U794: N Chateigner (EGEA1–2); Grenoble: J Quentin-Ferran (EGEA1–2).
References
Supplementary materials
Press release
Press release
Files in this Data Supplement:
Footnotes
RN and RV contributed equally.
Contributors ZL, RN and RV: designed and conducted the research; BL, NLM, CP, VS, RN and RV: provided essential reagents or provided essential materials; ZL, MR, AB, OD, JG-A, VS, CAC, RN and RV: analysed data or performed statistical analysis; ZL, RN and RV: wrote the manuscript and had primary responsibility for final content; all authors read, edited and approved the final manuscript.
Funding This research was funded in part by Merck Sharp & Dohme (MSD), the GA2LEN project, Global Allergy and Asthma European Network, and Conseil scientifique AGIR pour les maladies chroniques, National Hospital program of clinical research (PHRC-national).
Competing interests None declared.
Ethics approval Ethical approval was obtained from the relevant institutional review board committees (Cochin Port-Royal Hospital and Necker-Enfants Malades Hospital, Paris).
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves