Article Text

Abstract
Little is known about the impact of chronic breathlessness (modified Medical Research Council (mMRC) score ≥2 for most days, at least three of the last six months) on health-related quality of life (Short Form-12 (SF-12)). 3005 adults from randomly selected households were interviewed face-to-face in South Australia. mMRC ≥2 community prevalence was 2.9%. Adjusted analyses showed clinically meaningful and statistically significant decrements of physical and mental components of SF-12 (mean SF-12 summary scores in physical (−13.0 (−16.0 to −10.2)) and mental (−10.7 (−13.7 to −7.8)) components compared with people with mMRC=0) as chronic breathlessness severity increased, across five age groupings.
Statistics from Altmetric.com
Introduction
Chronic breathlessness is a distinct clinical syndrome1 most frequently attributed to respiratory disease. Chronic breathlessness has a profound impact on people's day-to-day function, emotional well-being, their families and correlates with poorer prognosis. As chronic breathlessness worsens, people limit their function to avoid breathlessness and ultimately may become housebound.
Data are lacking on the impact of increasingly severe chronic breathlessness in the general population on health-related quality of life (HrQoL)2 although there is a consistent relationship between increasing severity of chronic breathlessness and worsening (HrQoL) by
disease (COPD; chronic heart failure; interstitial lung disease; cystic fibrosis; lung cancer)
age (the elderly)
prognosis (the end of life).
The aim was to explore the impact of chronic breathlessness on people's self-reported HrQoL across the population. The null hypotheses were that there would be no relationship between intensity of chronic breathlessness (modified Medical Research Council (mMRC))3 scores and physical component score (PCS) and mental component score (MCS) of the Short Form-12 (SF-12).4
Methods
Data were collected in the 2015 South Australian Health Omnibus Survey (HOS), a multistage, systematic, clustered area sample of households in which face-to-face interviews were held only with the occupant who most recently had a birthday. Data were weighted to national normative data (5-year age group, sex, rurality and household size).
Health-related quality of life
The SF-12 is a 12-item questionnaire. Higher scores reflect better HrQoL.5 A clinically meaningful worsening may be as little as 3 points (PCS) or 3.5 points (MCS) in people with cardiorespiratory diseases.5
Breathlessness
mMRC breathlessness scale is validated in this population.3 Participants were asked if such breathlessness ‘affected them most days for at least three of the last six months’. A higher score reflects worse breathlessness (see online supplementary table S1). Data were grouped into mMRC 0, 1 or ≥2.
supplementary data
Socio-demographics
Demographic variables (9-year age groups, sex, educational attainment, rurality, employment and current smoking status) were used in the analyses.
Statistical analyses
After analysis of univariable relationships, three multivariable linear regression models were created: unadjusted, adjusted for all available factors and one excluding smoking status given its high correlation with chronic breathlessness. Data were also examined for the relationship between the two SF-12 subscales, increasing severity of breathlessness and age in five subgroups (15–44; 45–54; 55–64; 65–74; ≥75 (see online supplementary data).
Ethics
Participants gave informed verbal consent. This paper's reporting accords with Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.6
Results
Three thousand and five people participated (participation rate of 66.1%); 1466 were male (49.2%), 618 (20.7%) were aged ≥65 years and 2239 (75.1%) lived in the metropolitan area; 460 (15.4%) were current smokers (see online supplementary table S2). Two hundred and sixty respondents had mMRC grade 1 breathlessness (8.7%) and 88 (2.9%) had grades 2–4.
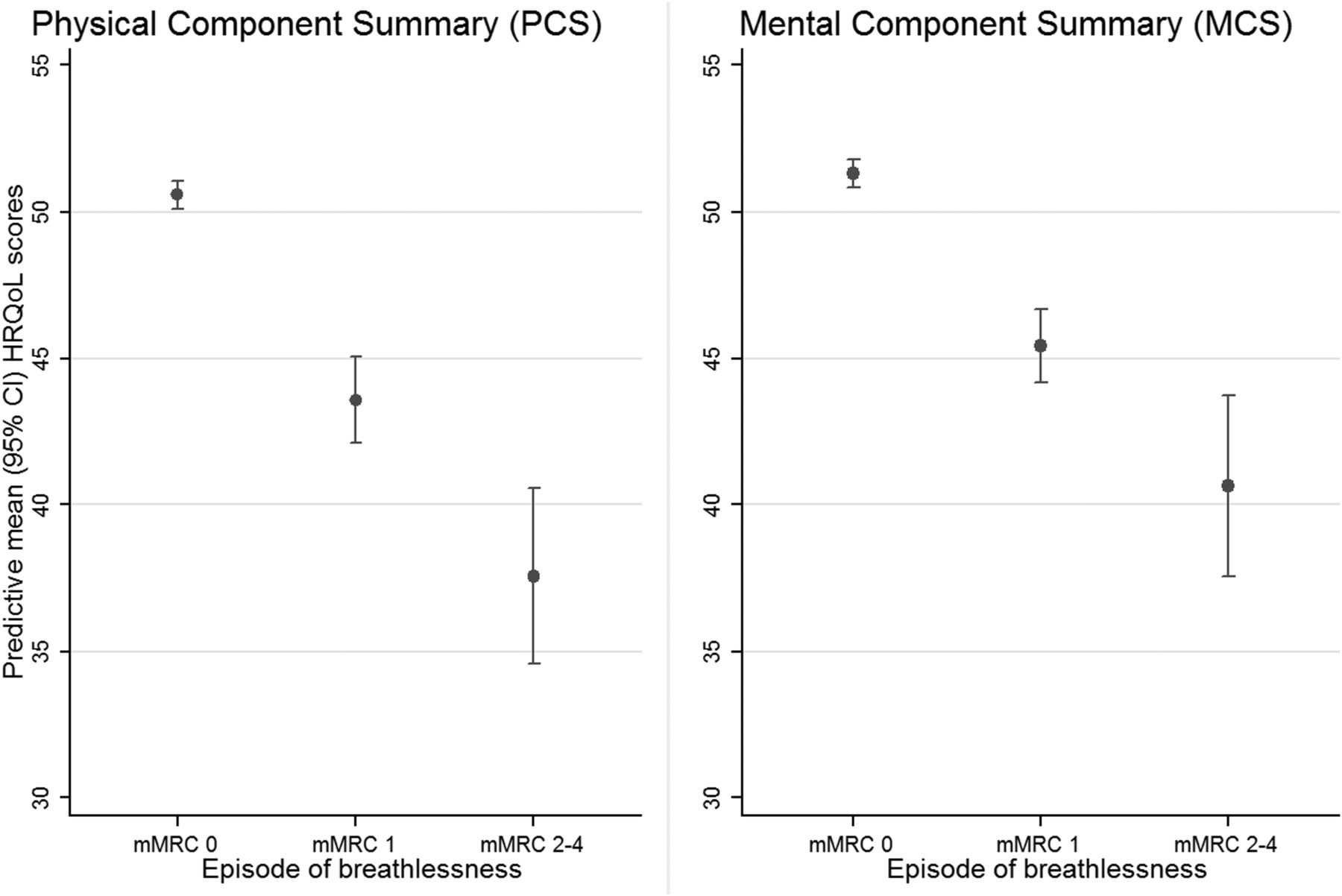
When compared with those who did not experience chronic breathlessness and adjusting for age, sex, socioeconomic factors and smoking status, people with mMRC of 1 or ≥2 breathlessness had reduced predicted mean physical (−7.2; 95% CI −8.4 to −5.7; −13.0; 95% CI −16.0 to −10.2, respectively) and mental (−6.0; 95% CI −7.3 to −4.8; −10.7 95% CI −13.7 to −7.8, respectively) SF-12 component summary scores (figure 1; see online supplementary tables S2 and S3).

Adjusted (age, sex, educational attainment, dwelling status, work status and smoking status) predicted mean health-related quality of life (HrQoL) (physical and mental health components) scores (possible range 0–70) of the Short Form-12 by intensity of breathlessness (none—modified Medical Research Council (mMRC) breathlessness scale 0; 1 and ≥2).
Across the population, there was a consistent clinically important and statistically significant worsening of physical and mental HrQoL with increasing severity of chronic breathlessness. In the sensitivity analysis, omitting smoking status did not change the magnitude or direction of findings.
This pattern of decreasing PCS and MCS of the SF-12 with increasing severity of breathlessness was seen in each of the five age subgroups examined (figure 2; see online supplementary table S5). For the same severity of breathlessness, the older the respondent was, the greater the impact that chronic breathlessness had on both components of HrQoL.

{kind=link}
{kind=link}
Comparison of level of chronic breathlessness (modified Medical Research Council (mMRC) scale) by age group by the health-related quality of life (Short Form-12) mental component score (MCS) and physical component score (PCS) in the general population of South Australia.
Discussion
For the first time in a whole adult population sample, this study shows that increasing severity of chronic breathlessness is associated with clinically important and statistically significant decrements in the PCS and MCS of the SF-12. Importantly, recruitment was independent of health service contact, diagnoses or age.
In subgroups previously studied, similar patterns were seen.7 ,8 One longitudinal population study which accounted for comorbidities and had correlation of physical findings at 12 years (n=3786; age 15–70) reported on moderate-to-severe persistent or incident breathlessness and impaired physical and mental HrQoL (SF-12) of the same magnitude.8 To complement these findings, the current HOS study had no upper age limit, a definition for ‘chronicity’ and covered all levels of mMRC.
Worsening breathlessness and clinically and statistically worsening HrQoL (MCS SF-36) has been confirmed (n=1169; age ≥70). As age increased, so did prevalence and severity of breathlessness, likelihood of anxiety or depression and poorer physical function.7
Using the EQ-5D-3L, HrQoL in 5944 (56.8% response) patients registered with two general practices showed a strong relationship between COPD and worsening HrQoL. With breathlessness, all domains of the EQ-5D-3L (mobility, self-care, usual activities, pain/discomfort, anxiety/ depression, health status) were worse.9
Limitations
No health information about breathlessness' aetiologies or their severity was collected nor were data on comorbidities, nor respondents' physical or social functioning. The real community prevalence of chronic breathlessness will be higher than the figures outlined in this study, given that residential care facilities were not included in the survey and chronic breathlessness is likely to be a significant symptom in those settings.
Strengths
Tools validated in this population were used to measure outcomes of interest: HrQoL and breathlessness. A standardised definition of chronicity was used. Enrolling adults regardless of age adds to previous work.
Implications for clinical practice/policy
The high prevalence, impact on people's daily lives and the strong association between increasing severity of chronic breathlessness and worsening HrQoL in the general population require a fundamental re-evaluation of the way that chronic breathlessness is sought in clinical histories. Clinicians need to develop skills to enquire systematically about things that patients forego to avoid breathlessness in order to ‘see’ its true impact, especially as the evidence base improves for safe, currently available interventions to reduce chronic breathlessness.10 Incorporating this evidence base into clinical practice will lessen the burden of chronic breathlessness in the community.
Implications for future research
Although mMRC is useful for defining breathlessness at a population level, there needs to be international consensus on a tool that can measure chronic breathlessness and is sensitive to change in routine clinical practice. To improve regression models, future research needs to account for other factors related to HrQoL including anxiety, depression, comorbidities and physiological measures including lung function.
Footnotes
Contributors All authors contributed equally.
Funding Funding for this study was derived from discretionary funds held by the Discipline, Palliative and Supportive Services, Flinders University, Adelaide, Australia.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The Ethics Committee of the South Australian Department of Health.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All available data can be obtained by contacting the corresponding author.