Article Text

Abstract
Lung cancer diagnosis during emergency hospital admission has been associated with higher early secondary-care costs and lower longer-term costs than outpatient diagnoses. This retrospective cohort study analyses the secondary-care costs of 3274 consecutive patients with lung cancer. Patients diagnosed during emergency admissions incurred greater costs during the first month and had a worse prognosis compared with outpatient diagnoses. In patients who remained alive, costs after the first month were comparable between diagnostic routes. In addition to improving patient experience and outcome, strategies to increase earlier diagnosis may reduce the additional healthcare costs associated with this route to diagnosis.
- Health Economist
- Lung Cancer
Statistics from Altmetric.com
Introduction
In the UK, 35% of new lung cancers are diagnosed during an emergency presentation.1 This is associated with poor outcomes.2 Hospital admissions are a poor patient experience.3 Reducing the proportion of patients diagnosed by this route has been identified as a priority by policy makers.
Inpatient admissions are the greatest contributor to secondary-care costs in patients with lung cancer.4–7 Only one small study has previously examined costs by route to diagnosis.5 This identified that early costs were higher in patients diagnosed during an acute admission than those diagnosed following outpatient referral. Our data also previously identified that diagnosis during an acute hospital admission was associated with higher 90-day costs, although costs were lower at 1 year. We hypothesised that this was due to the excess mortality in this poor prognosis group.7
The full health-economic impact of this route to diagnosis is not known. The aim of this study was to further analyse the effect of lung cancer diagnosis during emergency admission on secondary-care costs.
Methods
This was a retrospective cohort study. All patients first diagnosed with lung cancer at Leeds Teaching Hospitals NHS Trust between January 2008 and October 2013 were included.
Costs were based on the recorded hospital income, based on human resource group coding and national payment by results tariff. This represents the cost to the local National Health Service (NHS) commissioners for inpatient, outpatient and emergency department care. Community and palliative care costs were not available. All costs were adjusted to 2013–2014 prices. Day zero was defined as the date first seen by the lung cancer team.
Patients diagnosed during an emergency admission were compared with those diagnosed in outpatient clinics. Patient characteristics were compared using t-test (age) and χ2 analyses (all other characteristics). Survival was compared using Cox proportional hazard analysis. Ordinary least squares regression analyses of both 90-day and 1-year log-costs were performed. Covariates included in each analysis were age, performance status, route to diagnosis, diagnosis year, stage, histology, epidermal growth factor receptor (EGFR) gene mutation status and treatment received. Monthly costs were calculated for each patient.
Results
There were 3289 consecutively diagnosed patients. After exclusion of 15 patients (13 second or recurrent lung cancers and 2 corrupted data), 3274 patients were included for analysis. All patients had a minimum of 1 year follow-up.
There were 1027 (31.4%) patients diagnosed during an emergency admission and 2247 (68.6%) as outpatients.
Compared with outpatients, patients diagnosed during emergency admissions were older (mean age 73.9 vs 71.9 years, p<0.001), with a higher proportion with performance status 3–4 (61.7% vs 24.4%, p<0.001) and stage IIIB–IV disease (80.1% vs 50.4%, p<0.001). They were less likely to have a histologically confirmed diagnosis (54.1% vs 78.2%, p<0.001) or to receive radical treatment (5.8% vs 35.4%, p<0.001) and more likely to receive best supportive care (62.7% vs 25.7%, p<0.001). One-year survival was significantly worse (13.7% (95% CI 11.7% to 15.9%) vs 50.2% (95% CI 48.2% to 52.3%), HR 0.294 (95% CI 0.268 to 0.321), p<0.001). Median length of stay for those diagnosed during emergency admission was 12 days (IQR 6–22 days). The mean cost per bed-day during these initial admissions was £203.
The mean 1-month and 1-year costs for all cases were £2400 (95% CI £2313 to £2493) and £10 009 (95% CI £9725 to £10 285), respectively.
Univariate regression analysis shows that diagnosis during emergency admission is associated with increased 90-day (p=0.013) and reduced 1-year (p<0.001) costs. Multivariate regression, however, shows this to increase both costs (p<0.001).
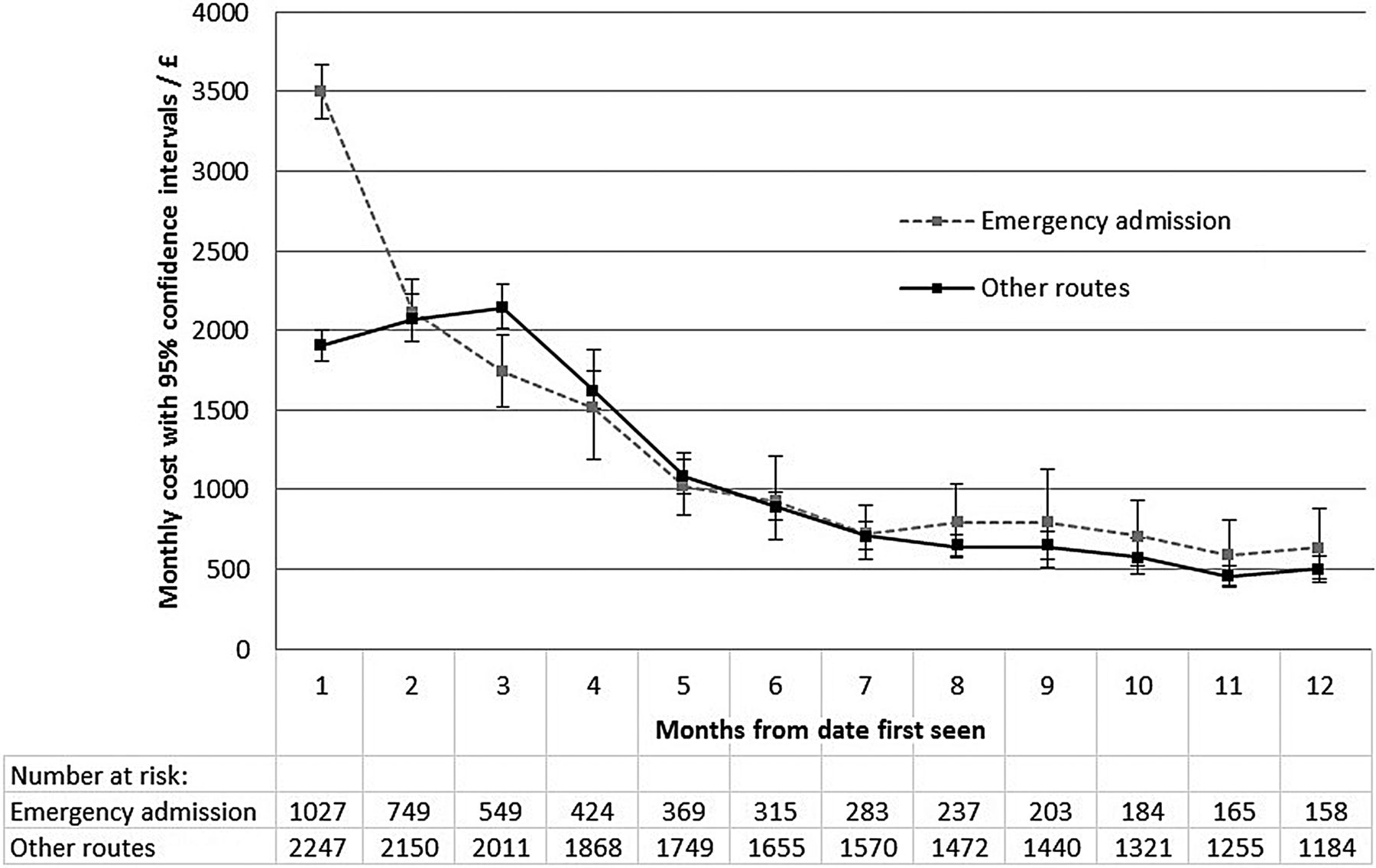
Figure 1 shows the mean monthly costs for all patients by route to diagnosis. Compared with outpatient diagnoses, diagnosis during emergency admission was associated with higher costs over the first month (£3499 (95% CI £3332 to £3667) vs £1899 (95% CI £1810 to £1999)), but lower costs over 1 year (£8123 (95% CI £7704 to £8552) vs £10 870 (95% CI £10 511 to £11 211)). This is likely to have been heavily influenced by excess mortality in this group.

Mean monthly costs.
Figure 2 shows the costs adjusted for survival, considering mean costs per patient alive in that month. Emergency admission was associated with increased cumulative mean alive costs over 1 year compared with outpatients (£15 059 (95% CI £14 235 to £15 966) vs £13 221 (95% CI £12 885 to £13 580)). The excess mean alive cost accumulated over the first year after diagnosis during emergency admission was £1838. Cumulative mean alive costs accrued between months 2 and 12 were similar between the two groups (£11 577 (95% CI £10 836 to £12 392) vs £11 321 (95% CI £10 979 to £11 663)).

{kind=link}
{kind=link}
Mean monthly cost of care while alive (censored for survival).
The proportion of cumulative 1 year costs that were attributable to inpatient and emergency department costs was greater for those diagnosed during an emergency admission (60.7% vs 35.4%).
Discussion
This is the largest analysis of direct hospital costs in the management of lung cancer according to route to diagnosis. This study used hospital income to reflect costs, which provides an electronic source of individualised costs that represent the true cost to commissioners. This may differ from the true cost to the hospital.
Emergency presentation was associated with a number of adverse parameters (worse performance status, more advanced disease, less radical treatment, shorter survival). These patients incur higher healthcare costs during the first month after diagnosis. Their low rate of histological confirmation and radical treatment, as well as the increased proportion of costs due to inpatient activity, suggest that this is due to the cost of the emergency admission rather than differing early investigations or cancer treatment. Lower costs after this time probably reflect excess mortality. In patients who remain alive, costs after the first month are comparable to outpatient diagnoses and the excess cost in the first month is the only measurable cost difference. Other studies have identified high hospital costs associated with the terminal phase of cancer care.8 A limitation of this study is not having access to primary-care, social-care and palliative-care costs, which are a significant contributor to cancer costs.9 ,10
The excess cost of diagnosis through emergency admission in this study was ∼£1800 per patient over the year after diagnosis. Healthcare systems with a higher cost per inpatient bed-day may find higher excess costs. In addition to improving patient experience and outcome, strategies to increase earlier diagnosis of lung cancer and reduce emergency diagnoses may reduce the additional healthcare costs associated with this route to diagnosis.
Footnotes
Contributors All authors contributed to the data analysis, manuscript preparation and manuscript review. The final research letter has been approved by all authors. The revised research letter has been approved by all authors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.