Article Text

Abstract
Introduction and objectives Patients undergoing treatment for heroin addiction die on average 15 years earlier than the general population (Smyth et al., 2006). Opioid-related deaths in England and Wales have increased by two-thirds since 2012 (Office for National Statistics 2015). Although smoking-related respiratory disease contributes to the excess mortality in drug and alcohol addiction, screening for lung disease is not routinely offered in community drug and alcohol treatment services (CDATs). We have established a “Lung Health Clinic” in our local CDAT (Brixton, Lambeth, SE London). Through this clinic we aimed to document the respiratory symptom burden, and COPD prevalence, in addicts accessing our local CDAT.
Methods Assessments: handheld spirometry (FEV1, FVC, FEV1/FVC ratio) and pulse oximetry (SpO2%). We recorded breathlessness (mMRC Dyspnoea Scale), chronic cough and cigarette smoking status.
Results 112 patients (88 male, mean(SD) age 46 (9) years) attended Jan–Dec 2015. Current/previous addictions included: smoked heroin 66.3%, intravenous heroin 32.5%, crack cocaine 68.2%, cannabis 60.0%. 81.3% were current cigarette smokers. Only 41% had accessed smoking cessation services despite these being offered in-house.
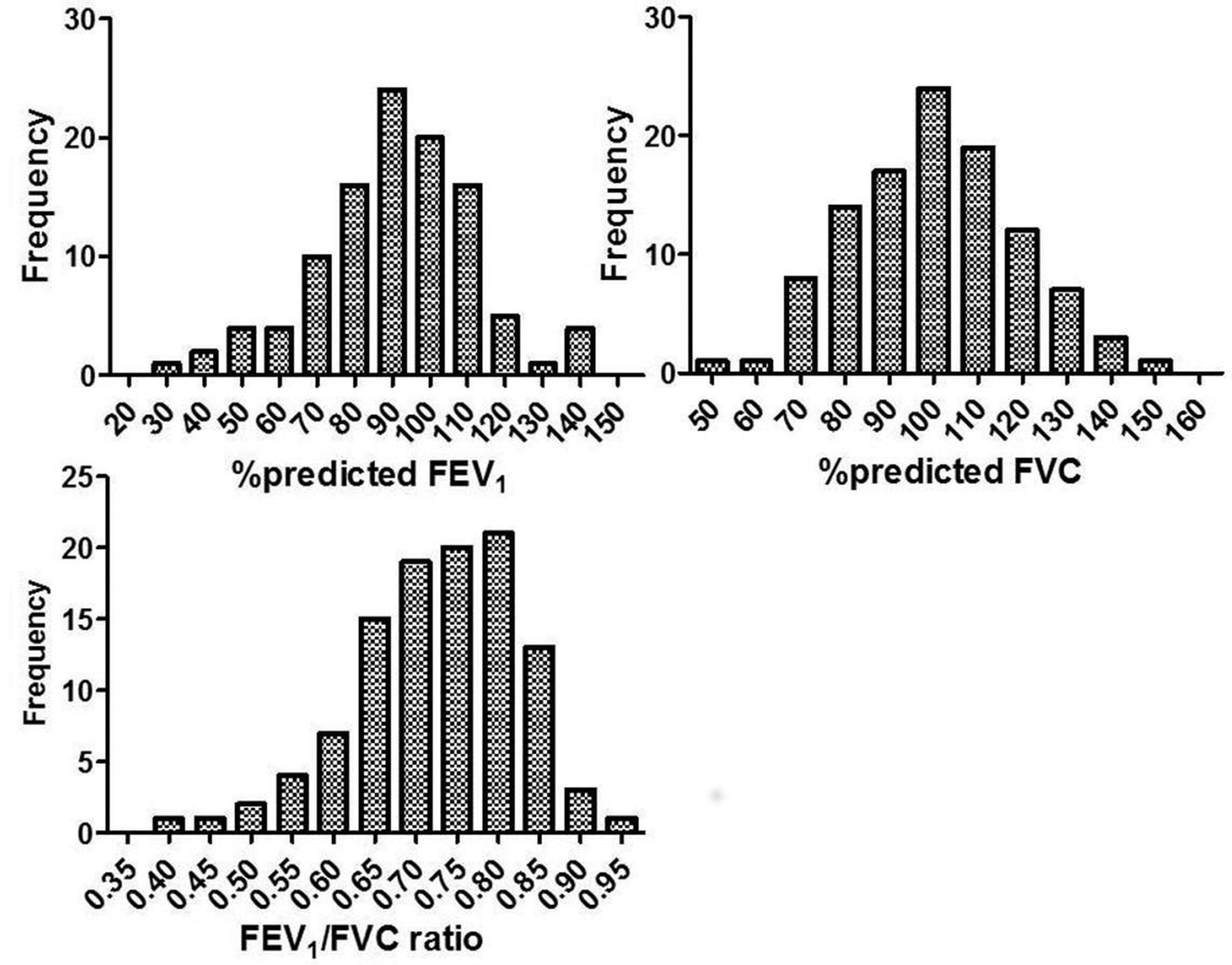
61.5% reported chronic cough. 20% reported significant breathlessness (mMRC Dyspnoea ≥ 2). 5% had a pre-existing COPD diagnosis, whereas spirometry [Figure 1] and clinical history were consistent with COPD in 36.4%. SpO2 ≤ 95% in 12.8%.
Conclusions There is a significant unmet burden of undiagnosed chronic lung disease, and respiratory symptoms, in our local CDAT, and a need to improve uptake of smoking cessation services. An economic model of expected gain in life expectancy and Quality Adjusted Life Expectancy (QALYs) from quitting is in development.

{kind=link}
Frequency distribution of %predicted FEV1/FVC ration in clients attending the Lung Health Clinic