Article Text

Abstract
Introduction In the UK, over a third of asthma patients are treated at BTS step 4 or 51 with similar suggestions of over use of high dose inhaled corticosteroids (ICS), equivalent to ≥1000 micrograms beclomethasone dipropionate, in patients with COPD.2 This has resulted in the highest dose ICS (HDICS-licensed daily dose equivalent to 2000micrograms beclomethasone dipropionate) with long-acting Beta2-agonist combination inhalers consistently appearing in the top five costliest drugs to the NHS. The London Respiratory Team have shared their concerns regarding the potential harm and waste associated with this practice; hence, many prescribing initiatives have been implemented to optimise ICS use through appropriate step down or ICS withdrawal. However cost-saving interventions such as generic prescribing have also been implemented.
Aims To ascertain whether any reduction in spend on HDICS combinations is due to treatment optimisation or generic switches.
Methods Monthly prescription cost analysis data available from the NHSBSA website (http://www.nhsbsa.nhs.uk) for the latest 15 months were analysed for the quantities prescribed and associated cost (Net Ingredient Cost) of all of the HDICS combination inhalers currently available.
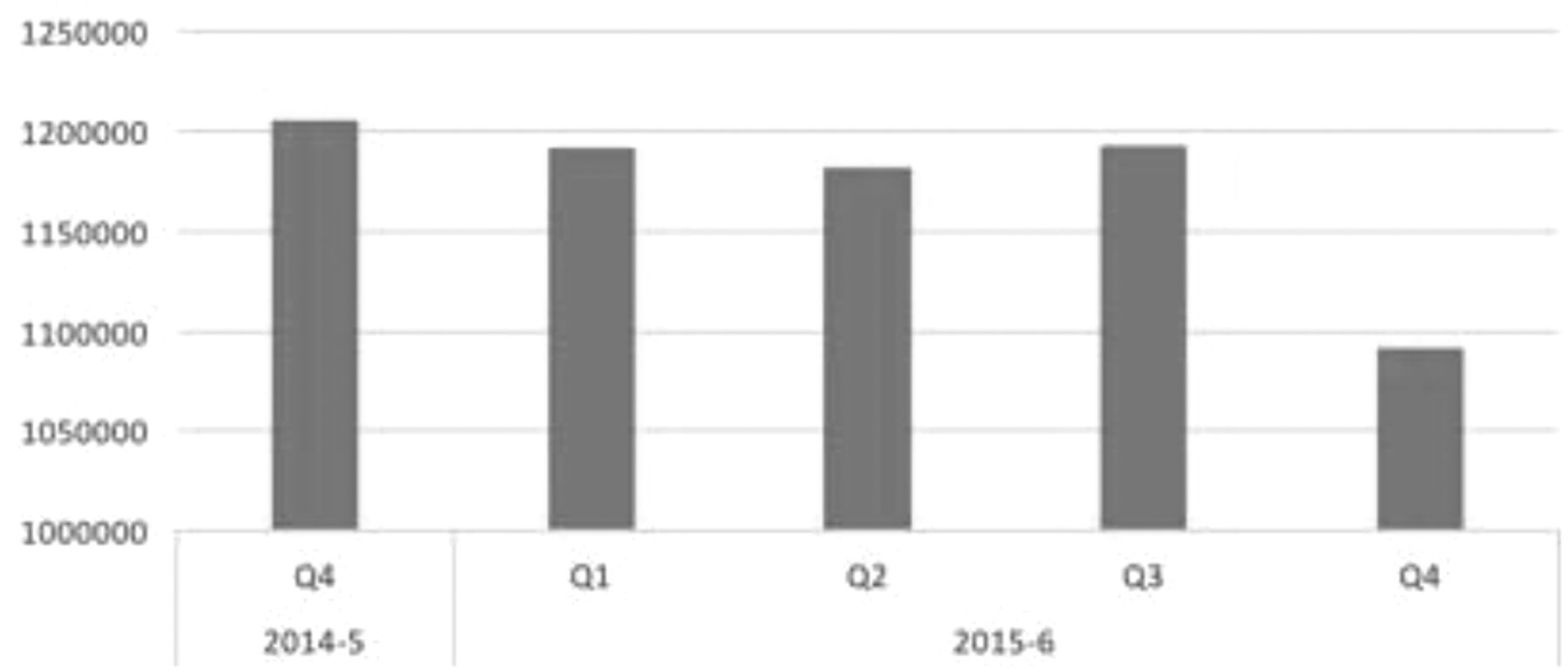
Results In 2015–16, the monthly spend on all HDICS combination inhalers fell from around £20million/month to £18million/month, and number of items fell from around 400,000/month to 365,000/month. By the last quarter, the switch from high cost HDICS combinations to lower cost ones accounted for 15% of all HDICS combinations, saving around £0.75million/month.
Conclusion The message around inappropriate use of high dose ICS is beginning to filter through. Savings have been made from both switching to lower cost HDICS combination products and reduction in total numbers prescribed. Some of these saving will be offset by some patients being prescribed lower cost, lowerz’ dose ICS combinations.
However the reduction in high dose prescribing is less than 10% of the total number prescribed. Given the extent of overuse, further harm and waste reduction can be made by reviewing the appropriateness of high dose ICS combinations prescribing in asthma and COPD with can lead to significant cost savings and improve value.
References
Covvey J, et al. Is the BTS/SIGN guideline confusing? A retrospective database analysis of asthma therapy. Prim Care Respir J 2013;22(3):290–5.
White P, et al. Overtreatment of COPD with inhaled corticosteroids-implications for safety and costs: cross-sectional observational study. PLoS One 2013;8(10):e75221.

{kind=link}
High dose ICS combinations – Quarterly Quantiities