Article Text

Statistics from Altmetric.com
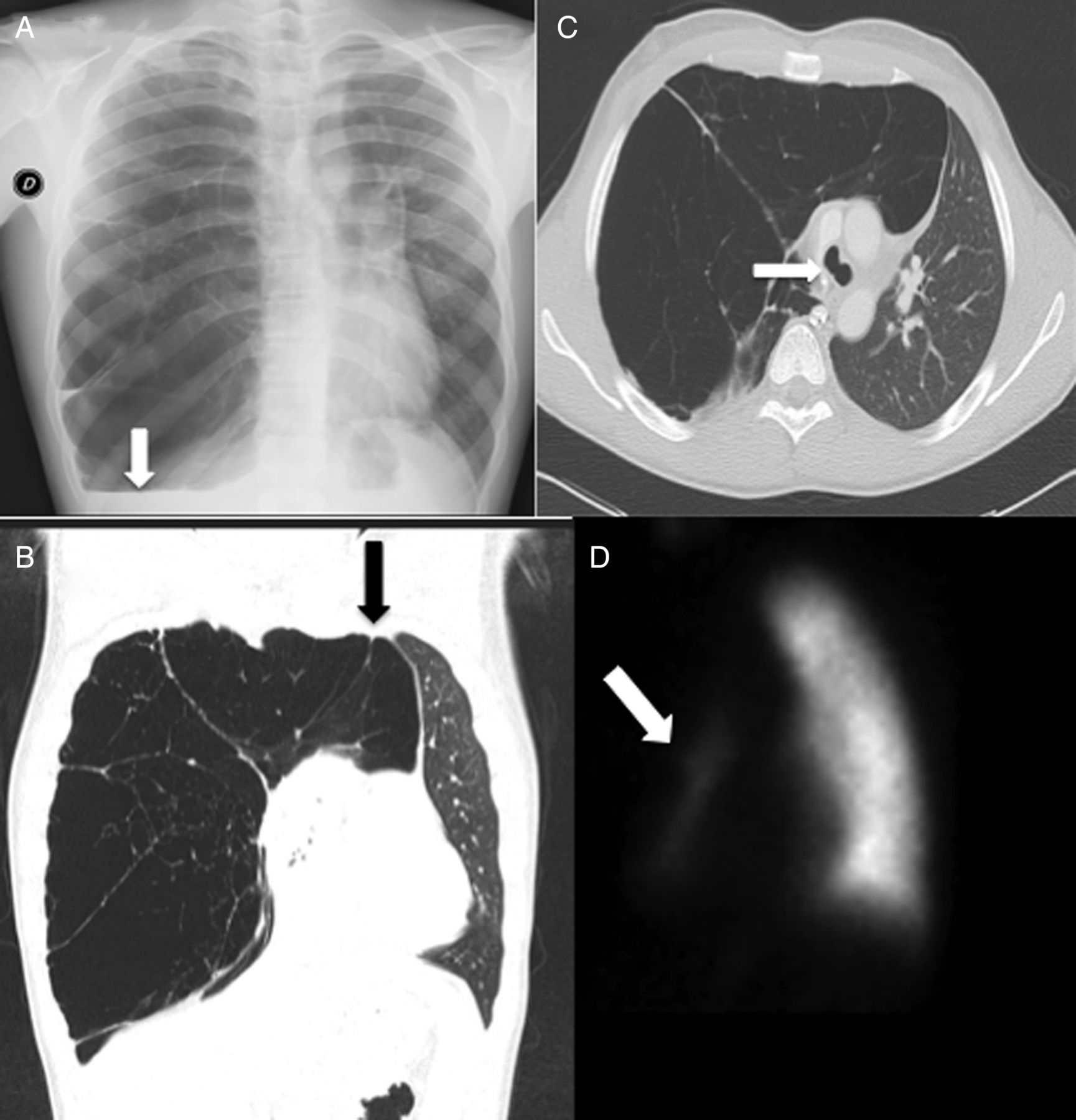
A 14-year-old boy was admitted with mild right chest pain, exercise dyspnoea and occasional palpitations. There was no smoking history. There was no past medical history of recurrent chest infections. The physical examination revealed an absence of breath sounds and hyper-resonance of the right hemithorax. A chest X-ray showed unilateral massive bullous disease with radiolucency of right lung and flattening of the right hemidiaphragm (figure 1A). The high-resolution chest CT scan confirmed air herniation towards left side with mediastinal shift resulting in airway displacement (figure 1B, C). A significant reduction of right lung perfusion was detected at radioisotope perfusion scan exclusively remaining in the lower lobe (figure 1D). Pulmonary function tests, arterial blood gas analysis and α-1 antitrypsin levels were normal. The patient underwent lung volume reduction surgery with extensive resection of right upper lobe through a minithoracotomy. The postoperative course was uneventful and he was discharged on the 7th day following his operation. He made a complete and full recovery within 2 years.
{kind=link}
(A) Chest X-ray showing a right lung rarefaction with flattening of ipsilateral diaphragm (white arrow). (B) Coronal view of CT scan (lung window) showing the right lung herniation towards left side (black arrow). (C) Axial view of CT scan (bone window) showing airway rotation due to mediastinal shift (white arrow). (D) Lung perfusion scan showing the impressive reduction of right lung perfusion (white arrow).
Giant bullous disease, known as the vanishing lung syndrome, is a very rare condition in children where one or more bullae can enlarge and fill more than one-third of the hemithorax compressing the surrounding normal lung parenchyma causing mediastinal shift. This disease usually has a strong association with COPD with bilateral disease in patients with significant smoking history or affected by α-1 antitrypsin deficiency.1 Bullectomy or lung volume reduction surgery is considered the definitive treatment of choice.
Footnotes
Contributors All authors have equally contributed to plan, conduct and report the work described in the article. MA and FV are the contributors responsible for the overall content as guarantors.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Ethical Committee of Department Paride Stefanini University of Rome Sapienza.
Provenance and peer review Not commissioned; externally peer reviewed.