Article Text

Abstract
Background Second-hand smoke (SHS) exposure has been linked to the development of and morbidity from lung disease. We sought to advance understanding of the impact of SHS on health-related outcomes in individuals with COPD.
Methods Among the participants with COPD in SPIROMICS, recent SHS exposure was quantified as (1) hours of reported exposure in the past week or (2) reported living with a smoker. We performed adjusted regression for SHS with outcomes, testing for interactions with gender, race, smoking and obesity.
Results Of the 1580 participants with COPD, 20% reported living with a smoker and 27% reported exposure in the past week. Living with a smoker was associated with worse St George's Respiratory Questionnaire score (SGRQ, β 3.10; 95% CI 0.99 to 5.21), COPD Assessment Test score (β 1.43; 95% CI 0.52 to 2.35) and increased risk for severe exacerbations (OR 1.51, 95% CI 1.04 to 2.17). SHS exposure in the past week was associated with worse SGRQ (β 2.52; 95% CI 0.47 to 4.58), nocturnal symptoms (OR 1.58; 95% CI 1.19 to 2.10), wheezing (OR 1.34; 95% CI 1.02 to 1.77), chronic productive cough (OR 1.77; 95% CI 1.33 to 2.35) and difficulty with cough and sputum (Ease of Cough and Sputum scale, β 0.84; 95% CI 0.42 to 1.25). SHS was associated with increased airway wall thickness on CT but not emphysema. Active smokers, obese individuals and individuals with less severe airflow obstruction also had higher susceptibility to SHS for some outcomes.
Conclusion Individuals with COPD, including active smokers, have significant SHS exposure, associated with worse outcomes and airway wall thickness. Active smokers and obese individuals may have worse outcomes associated with SHS.
Trial registration number NCT01969344 (clinicaltrials.gov).
- COPD epidemiology
- Tobacco and the lung
Statistics from Altmetric.com
Key message
What is the key question?
“Do individuals with COPD and exposure to secondhand smoke have worse outcomes compared to individuals with COPD not having exposure to secondhand smoke, and are there subgroups of COPD with higher susceptibility to such adverse outcomes?”
What is the bottom line?
Individuals with COPD who are exposed to second-hand smoke have higher risk of worse outcomes including dyspnoea, lower exercise capacity and respiratory symptoms, and also have more airway wall thickness on CT.
Why read on?
To the best of our knowledge, this is the first study that shows that second-hand smoke exposure is associated with adverse outcomes in current as well as former smokers with COPD, and the first to demonstrate distinct subgroups (current smokers, obese individuals, less severe airflow obstruction) that have a heightened susceptibility to adverse outcomes associated with second-hand smoke.
Introduction
Since the Surgeon General's report in 1964 linking tobacco smoke to lung cancer, the recognition of tobacco's impact on health has grown.1 There is increasing awareness of the role of second-hand smoke (SHS) exposure in contributing to adverse health outcomes,1 ,2 including development of COPD.3–6 Moreover, the chemistry of SHS differs from that of primary smoke, creating the possibility of SHS being an additional risk factor even for active smokers.7 Among those with COPD, a few studies suggest that SHS exposure adversely impacts quality of life, dyspnoea and risk of COPD exacerbation, but these studies are limited to former smokers.8–10 It is not fully known whether SHS is detrimental to health outcomes in COPD, and specifically it has not been shown whether SHS is detrimental in active smokers with COPD. Further highlighting the lack of evidence in this realm, the Global initiative for Obstructive Lung Disease (GOLD) consensus report, though noting the possible contribution of SHS to COPD incidence, does not mention SHS as a contributor to COPD morbidity.11 Additionally, whether there are subgroups of COPD at heightened susceptibility to SHS has not been elucidated, particularly in current smokers with heavy smoke exposure history.
We sought to determine the independent contribution of SHS to clinical characteristics using validated exposure instruments, CT measures and validated COPD outcomes in a large study of former and current smokers with COPD having a high personal level of primary smoking history. We analysed the large, well-characterised COPD cohort in SPIROMICS12 in order to understand if important subgroups of individuals with COPD could be identified who might have heightened susceptibility to the negative impacts of SHS exposure, such as race and gender, given evidence in the literature of heightened susceptibility of African Americans and women13 ,14 to the effects of smoking, as well as obesity, given evidence of heightened susceptibility of obese individuals to indoor air pollution.15 Additionally, of interest was the potential heightened susceptibility of former smokers (compared with current active smokers) to the adverse effects of SHS.
Methods
SPIROMICS12 is a multicentre study of current and former smokers (≥20 pack-years) with and without COPD and non-smokers without COPD aged 40–80 years. The original goals of the study were to determine intermediate outcomes and end points in the population with COPD in order to identify subgroups of individuals with COPD who could be targeted for future specific therapeutic strategies and treatments. Current and former smokers with (strata 3–4) and without COPD (stratum 2) were recruited, as were healthy, lifelong non-smokers (stratum 1). We studied all individuals with COPD (post-bronchodilator FEV1/FVC of <70%) including subjects in strata 3 (FEV1 ≥50% predicted) and 4 (FEV1 <50% predicted) in primary analysis.11 Secondary analyses incorporated individuals from strata 1–2. Further details on the study population can be found in the online supplementary material.
Supplemental material
SHS characterisation
Participants were asked about smokers in the household. SHS exposure over the past week was quantified in hours using a validated questionnaire for the assessment of exposure in multiple locations including within and outside of the home (including other person's home, workplace, car or other location while travelling, place of entertainment and other location).9 ,16 Additional questions quantified lifetime SHS exposure in the home in years, as previously used by Eisner et al.4
CT measures
Participants underwent whole-lung multidetector helical CT at full inspiration and expiration. Measurements of interest included percentage emphysema, percentage gas-trapping, Pi10 (a measure of airway wall thickness) and airway dimensions including area and diameter of walls and lumens of airways in generations 1–6. Details are provided in the online supplementary material.
Outcomes
Outcomes of interest were respiratory-specific quality of life (St George's Respiratory Questionnaire (SGRQ)),17 general quality of life (short-form 12-item questionnaire, SF12),18 exercise capacity (6 min walk distance in metres (6 MWD)),19 dyspnoea (modified Medical Research Council questionnaire)20 and COPD health status (COPD assessment test, CAT) (see online supplementary e-table 1).21 Cough and phlegm over the past day were measured using the total score from the Ease of Cough and Sputum questionnaire.22 Respiratory symptoms (cough, phlegm, bronchitis, wheezing and nocturnal symptoms) were measured using the American Thoracic Society Division of Lung Diseases of the National Heart and Lung Institute Questionnaire (ATS/DLD-78-adult).23 Chronic cough and phlegm status was determined as an affirmative response to the question “Do you usually…?” for the individual symptom, and chronic productive cough was determined as an affirmative response to both questions, as described previously.24 Participants were asked about medication changes or dose adjustments, unscheduled doctor visits, emergency room visits, days hospitalised and intensive care unit admissions for COPD exacerbations and frequency of these instances over the past year. Severe exacerbations were defined as events requiring emergency room visit or hospitalisation. All information was collected at baseline; however, additionally we analysed available data regarding exacerbations noted by participants from the time of study enrolment to most recent follow-up contact.
Statistical methods
Recent SHS exposure was determined by two exposure metrics including (1) report of living with a smoker (yes/no), referred to as ‘living with a smoker’, and (2) SHS exposure reported in any location over the past week, dichotomised as 0–1 h of exposure (non-exposed) or ≥2 h of exposure (exposed) as in previous publications,9 referred to as ‘recent SHS exposure’. Years of lifetime SHS exposure were also studied and modelled as quartiles of exposure, to evaluate possible dose response.4 Participant characteristics were compared based on SHS exposure using t tests and χ2 tests.
We analysed the relationship between SHS exposures and outcomes using linear and logistic regressions, adjusting for age, gender, race (African American vs other), education (high school education or less vs more than high school), current smoking and pack-years smoked. Cross-sectional data were analysed using linear or logistic regression models (in which coefficients and log odds were the modelled effects) with the exception of analyses of longitudinal exacerbations over follow-up, which were analysed as count data using adjusted Poisson regression (in which relative risk was the modelled effect) and analysis of mean differences in airway wall and lumen area and diameter as well as wall area percentage for generation 1–6 airways, for which we used generalised estimating equations.25 Further detail on statistical methods can be found in online supplementary material.
Of interest was possible effect modification of current smoking, such that non-smokers might have relatively higher susceptibility to SHS. In sensitivity analyses, we additionally adjusted these models for the daily number of cigarettes actively smoked to further isolate the effects of SHS over active smoking. We also tested for interactions between SHS exposure and race, gender, severity of airflow obstruction (GOLD 1,2 as less severe vs GOLD 3,4 as more severe) and obesity (defined dichotomously as body mass index (BMI) >30 kg/m2).
All analyses were conducted with Stata 12 (Stata Statistical Software: Release 12 (program). College Station, Texas: StataCorp., 2011). p Value <0.05 was the threshold for significance for main effects and 0.10 for interactions.15 ,26 ,27 SPIROMICS was approved by institutional review boards at each centre and all participants provided written informed consent (ClinicalTrials.gov: NCT01969344).
Results
At the time of analysis, 1580 participants had spirometric evidence of COPD. Of these participants, 20% (n=313) reported living with a smoker, 54% (n=170) of whom were current smokers and 46% (n=143) were former smokers. A total of 428 participants with COPD (27%) reported recent SHS exposure (ie, ≥2 hours of exposure within the past week), while 1152 (73%) reported 0–1 h of exposure. Participants reporting recent SHS exposure had a median of 7 h of SHS exposure (25th percentile 3, 75th percentile 21, online supplementary e-figure 1). Participants reporting recent SHS exposure were younger (mean age 61.9 vs 66.8 years), more likely to be African American (23% vs 12%), had less education and lower household income (table 1). Although there were minimal differences in pack-years smoked, there were more current smokers in the recent SHS exposure group (64% vs 20%). Individuals reporting recent SHS had significantly better lung function (FEV1% predicted 63.5 vs 60.2) and less emphysema and gas-trapping on CT (4.8% vs 8.1%, and 63.5% vs 66.9%, respectively). SHS exposure data was missing in only 38 of the 1580 participants, who were excluded from analyses. There were strong correlations between metrics of recent SHS exposure (see online supplementary e-table 2), such that individuals with more reported hours of SHS exposure in the past 7 days were more likely to live with a smoker. Additionally, mean years of SHS exposure reported before and after the age of 18 were significantly higher in the groups reporting more hours of SHS exposure in the past week and living with a smoker. Median follow-up time for exacerbation data was 594 days (25th percentile 292, 75th percentile 995) in the cohort with COPD (strata 3–4).
Characteristics of GOLD 1–4 participants, by hours of second-hand smoke exposure per week
Association of living with a smoker and outcomes
After adjustment, living with a smoker was associated with worse outcomes (table 2) including SGRQ, SF12, CAT and higher ease of cough and sputum scores (ie, more impaired). Living with a smoker was also associated with severe exacerbations in the past year and chronic productive cough. Additionally, living with a smoker was associated with increased airway wall thickness measured by Pi10, but not with emphysema or gas-trapping.
Associations of living with a smoker and COPD outcomes in SPIROMICS
Association of recent SHS exposure (≥2 h of SHS exposure in the past week) and outcomes
Recent SHS exposure was associated with worse short-term outcomes after adjustment (table 3 and figure 1). Recent SHS was associated with worse SGRQ score, nocturnal symptoms, wheezing, worse ease of cough and phlegm and less exercise capacity. To account for possible influences from occupational exposures,28 models were additionally adjusted for report of exposure to vapours, dusts, gases or fumes in the longest-held job, and results were similar. Measures of recent SHS exposure (hours of SHS exposure in the past 7 days and living with a smoker) were associated with differences in airway dimensions (tables 2 and 3). In generation 5 airways, wall area and lumen area and diameter were smaller in those with SHS exposure compared with those without, the wall area was thicker relative to lumen size, as indicated by significantly higher wall area percentage. Results for other airway generations (1–4, 6) did not have significant results (data not shown).
Associations of ≥2 h of SHS exposure in past week with COPD outcomes in SPIROMICS
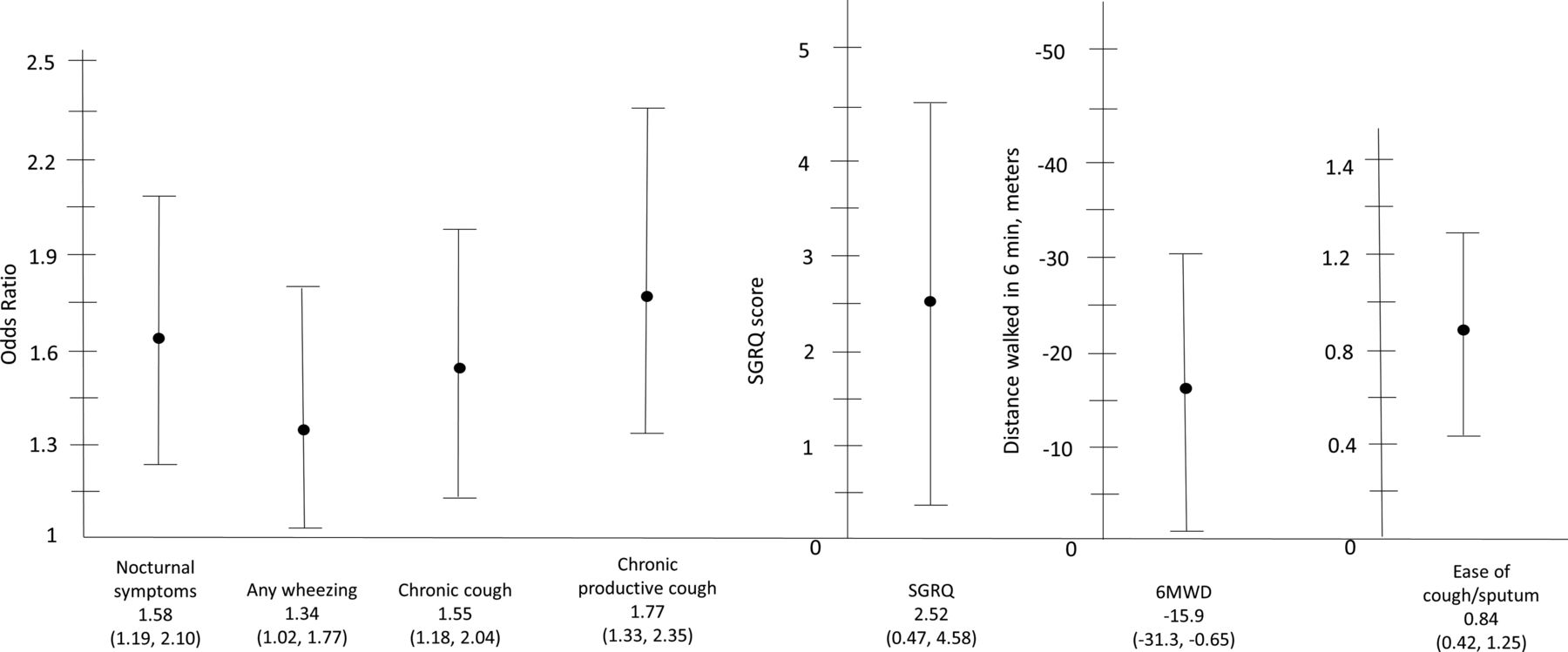
Impact of hours of second-hand smoke (SHS) exposure in the past week on health outcomes in all participants with COPD is shown. Modelled estimates shown are for ≥2 h of recent SHS exposure compared with participants with 0–1 h of exposure. 6MWD, 6 min walk distance in metres; SGRQ, St George's Respiratory Questionnaire.
Years of SHS exposure and outcomes
Lifetime exposure to SHS was highly prevalent, with 82.1% reporting home exposure before age 18, and 77.8% reporting home exposure after age 18. Participants were divided into quartiles based on years of home SHS exposure during their lifetime, (median (range): first quartile 18 years (0–18), second quartile 21 years (19–23), third quartile 33 years (24–40) and fourth quartile 52 years.(41–90)). We found minimal contribution of years of cumulative exposure reported with health outcomes in participants with COPD when testing the associations of quartiles 2–4 compared with the first quartile using disjoint categories for each quartile (see online supplementary e-table 3). When we tested the overall contribution of years of SHS exposure using likelihood ratio testing of nested models, only the model of SGRQ reached statistical significance (p=0.047) in its overall contribution to the model.
Subgroups with increased susceptibility to SHS
We found interactions between SHS metrics and smoking status, obesity and severity of airflow obstruction. Current smoking modified the effect of SHS exposure on several outcomes (figure 2 and table 4), such that in most cases current smokers appeared to have higher susceptibility to adverse outcomes than former smokers. Living with a smoker was linked to a higher risk of a severe COPD exacerbation in the past year in current smokers compared with former smokers (OR 2.33 vs 1.12, interaction p=0.055). Recent SHS exposure had a greater negative impact on 6 MWD in current smokers compared with former smokers (−27.41 vs −5.96, interaction p=0.071); however, only general quality of life was worse in former smokers compared with active smokers (SF12 −2.93 vs 0.68, interaction p=0.006). Models including adjustment for number of daily cigarettes smoked did not appreciably change the effect of SHS among those still smoking (data not shown).
Significant interactions between SHS exposure and smoking status, obesity, severity of airflow obstruction

Interactions between current smoking and second-hand smoke exposure in COPD. SF12, short-form 12-item questionnaire.
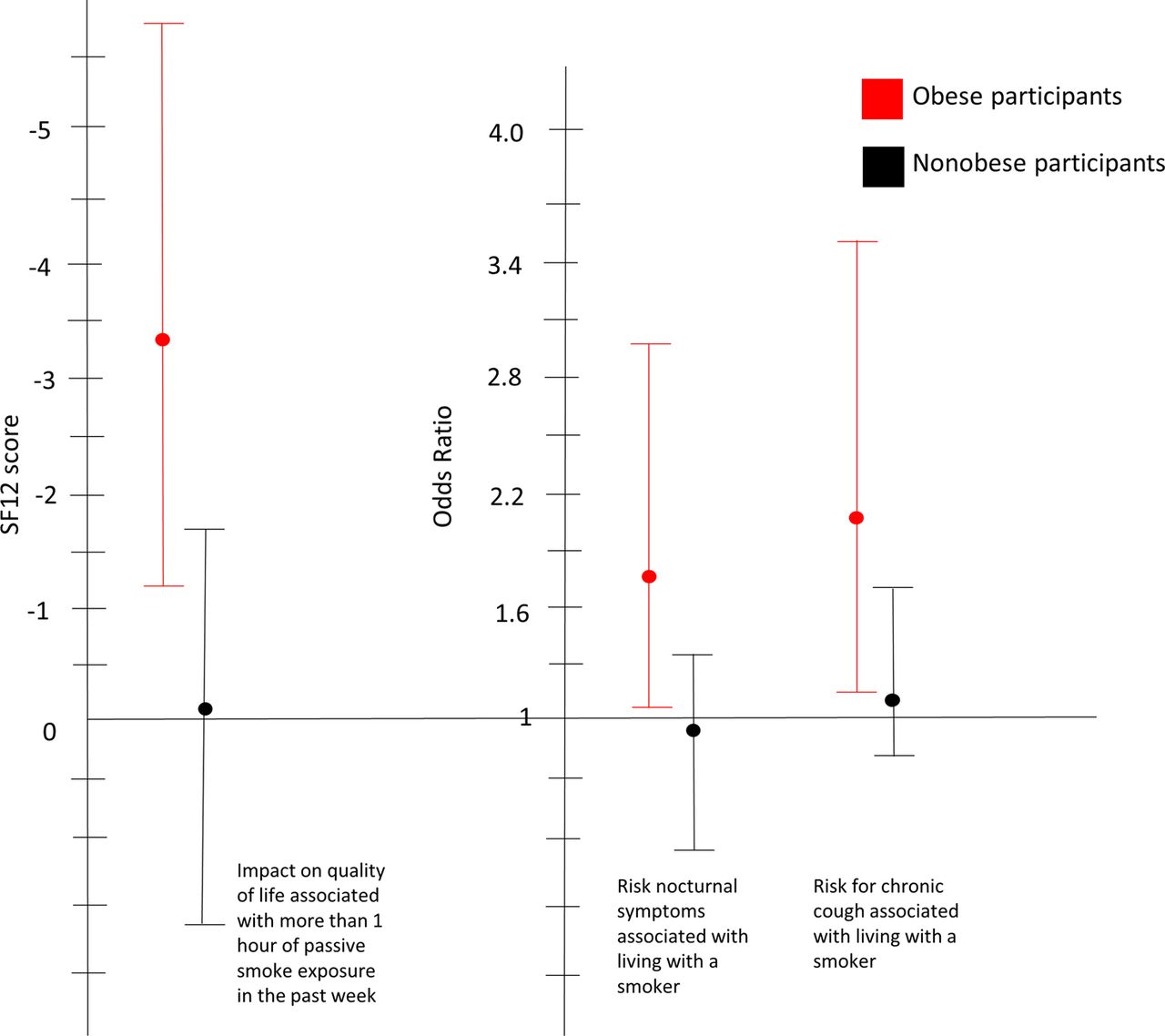
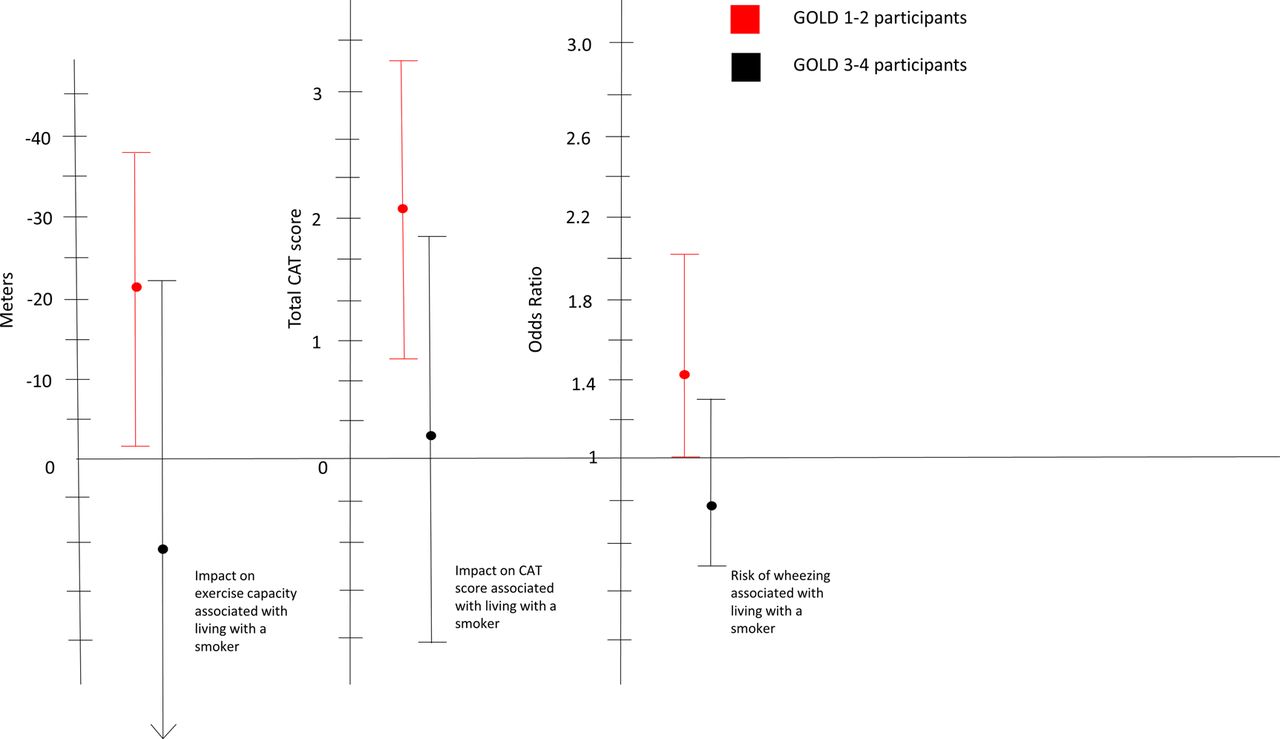
Those with milder airflow limitation and obese individuals had greater adverse effects associated with SHS exposure for some outcomes (figures 3 and 4, table 4). Living with a smoker was associated with worse outcomes among participants with less severe air flow obstruction (GOLD 1–2) compared with those with more severe obstruction (GOLD 3–4), including greater decrement in exercise capacity, worse CAT score and more wheezing. Among obese individuals, living with a smoker was linked with a higher risk of nocturnal symptoms and chronic cough compared with non-obese individuals. Additionally, recent SHS exposure was associated with worse quality of life among obese individuals compared with non-obese individuals, though no such association was noted for SGRQ. We found no significant interactions with gender or race.

Interactions between obesity and second-hand smoke exposure in COPD. SF12, short-form 12-item questionnaire.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Interactions between severity of COPD and second-hand smoke exposure in COPD.
Impact of SHS exposure on outcomes in non-smokers and current and former smokers without COPD
Analyses of recent SHS exposure and living with a smoker were also performed similarly in the cohort of healthy non-smokers (stratum 1, n=193) and the cohort of former and current smokers without COPD (stratum 2, n=803) and results are displayed in online supplementary e-tables 4 and 5. There were fewer statistically significant associations of recent SHS exposure and living with a smoker with outcomes in stratum 1, likely reflecting the small size of the cohort and relative low prevalence of reported SHS exposure (only in 12%); however, several significant associations were present within stratum 2, illustrating further the importance of SHS in influencing respiratory symptoms in the general population as well as those with COPD.
Discussion
SHS is an unfortunately common exposure among individuals with COPD. We have shown that SHS is a significant contributor to adverse outcomes in COPD, even among active smokers, in a large, well-characterised cohort of patients with a wide range of COPD severity. Recent SHS exposure and living with a smoker are associated with worse respiratory symptoms, quality of life and relative airway wall thickness in COPD. Living with a smoker is also associated with risk of severe exacerbations. Importantly, SHS is linked to worse outcomes even among active smokers. In addition, obese individuals and individuals with less severe COPD may be more susceptible to the adverse effects of SHS.
About 20% reported living with a smoker and 36% of participants with COPD reported ≥2 h of recent SHS exposure, significantly higher than the Centers for Disease Control and Prevention (CDC)'s estimates that 5.4% of non-smoking adults are exposed to SHS at home.29 Such findings highlight the extraordinary prevalence of SHS exposure in COPD. Recent SHS exposure was associated with higher risk of adverse outcomes in COPD, including lower exercise capacity, worse quality of life and more respiratory symptoms. Owing to the large size of SPIROMICS, our findings lend substantial weight to the findings of previous studies8 ,9 which have shown that higher levels of SHS exposure are associated with worse health status, quality of life, dyspnoea, exercise capacity and healthcare usage in former smokers with COPD. Further, we were able to test these associations in a well-characterised population with COPD with a high burden of smoke exposure (>20 pack-years) and also demonstrated that the associations between SHS and negative health outcomes were also present in former and current smokers without COPD, also lending weight to our findings that SHS is an important risk factor for adverse outcomes.
To our knowledge, our results are the first to show the association of SHS with greater relative airway wall thickness in COPD, a novel finding which correlates with chronic bronchitic symptoms.30 ,31 These findings were shown using two distinct techniques: Pi10 and using generation-specific airway lumen and wall data. Though these latter findings were only noted in generation 5 airways, previously, Smith et al reported significant changes in generation 4–6 airways in the population with COPD when compared with strata 1–2 individuals. It is likely that we were unable to see differences in generations other than 5 because of the smaller sample size studied (COPD participants only) and the limited variability in airway dimensions in the population with COPD when compared with studying the larger cohort. Experimental models of SHS exposure in rats have shown heightened pulmonary inflammation leading ultimately to airway and airspace remodelling.32 The mechanisms for airways and airspace injury due to SHS have not been clearly established among individuals or in animal models where COPD pre-exists, and would be the next step in order to better explain the findings of our study. Importantly, our findings are consistent with those of general population studies which have shown a higher risk of chronic bronchitis in non-smokers exposed to SHS.1 ,33
Finally, we have shown that there are possibly subgroups of individuals with COPD that experience higher susceptibility to the health effects of SHS exposure. We hypothesised that former smokers would be more sensitive to SHS than current smokers. This was not the case. For some outcomes such as quality of life, current smokers showed a greater impact of SHS compared with former smokers. One might intuit that SHS exposure would not greatly impact actively smoking individuals, given the small burden that SHS represents when compared with the extensive burden of primary smoking. However, our findings suggest that it is possible that current smokers experience worse outcomes related to SHS possibly because they have a longer duration (though no difference in pack-years smoked, there is a possibility of more hours of active and passive smoke exposure in any given day) or concentration of smoke exposure, as opposed to the quantity of exposure. Additionally, it is important to consider that the toxicity of SHS is qualitatively and quantitatively different from direct active smoke exposure and as such has different effects on outcomes in COPD. Though most of the compounds emitted in SHS are similar to those in mainstream smoke, the quantitative makeup of SHS and mainstream smoke has been shown to differ. In some cases, the concentration of certain compounds in SHS is greater than that of mainstream smoke, that is, nicotine, ammonia, formaldehyde, and in other cases, that is, N′-nitrosonornicotine, (methylnitrosamino)-1-(3-pyridyl)-1-butanone, the opposite is true. Additionally, the makeup of SHS is often greatly impacted by other environmental exposures.7 ,34 Such variation in the quantitative burden of certain compounds could potentially explain our paradoxical findings with regard to current and former smokers with COPD. It is also possible that active smokers have heightened airway inflammation and resulting damage to epithelial cells that alter susceptibility to further inflammation and damage due to SHS. It is possible that SHS is a marker for other behaviours such as medication adherence, exercise or other habits which are less favourable to overall health. The mechanism is an important target for further study, but it also highlights the clinical and public health importance of minimising SHS exposure in all individuals regardless of smoking status.
Obese individuals also showed heightened susceptibility to SHS, with a higher risk of nocturnal symptoms, chronic cough and poor quality of life as a result of SHS compared with lean individuals. These findings are consistent with recently published findings showing obesity as a susceptibility factor for adverse health outcomes related to indoor air pollution in both COPD15 and asthma.35 To our knowledge this is the first study showing that obesity may be a susceptibility factor for adverse outcomes associated with SHS. The increased inflammation associated with fat, specifically visceral adipose tissue, may lead to higher amounts of systemic and airway inflammation and may lead to alterations in immune defences in the lung leading to worse outcomes as a result of pollutant exposure.36 Additionally, obesity may be a reflection of more time spent at home (exposed to home SHS), or also a high fat, low antioxidant diet which has been shown to be proinflammatory.37 Whatever the mechanism, our findings lend weight to the necessity for further studies of obesity as a susceptibility factor for pollutant exposure in lung disease. We also found that individuals with less severe airflow limitation (GOLD stage 1–2 participants) had slightly more susceptibility to adverse outcomes due to SHS than participants with more severe airflow limitation (GOLD stage 3–4 participants). Though this finding is seemingly counterintuitive, it is plausible that individuals with worse COPD severity have such negative outcomes that detecting a further negative effect of SHS would be difficult. It is also possible that individuals with more severe COPD adopt avoidance behaviours that would attenuate the burden of SHS exposure despite having the same amount of exposure as gauged by our metrics of SHS exposure.
Our study is subject to some limitations. Our measures of SHS exposure rely on self-report, and there is a possibility of measurement error. We used a questionnaire that has been previously validated and shown to be associated with health outcomes. Additionally, our findings were consistent across two measures of SHS exposure (living with a smoker and SHS over the past week), further demonstrating their robustness. We were unable to find an association between years of previous SHS exposure and COPD health outcomes. We were similarly unable to find an association between SHS and percentage emphysema and gas trapping on CT. It is not clear why shorter-term exposures seemed to have more impact than longer-term exposures. It is possible that, in the short term, individuals with COPD including active smokers are susceptible to the acute inflammatory effects of SHS, but in the long term, primary smoking outweighs the effect of SHS on progression of COPD. It is also possible that longer-term measures are more subject to recall bias. In addition, this study is subject to the limitations of a cross-sectional study design including issues of temporality and causality. For example, perhaps individuals with more symptoms or more severe disease are more likely to live with a smoker or have a higher risk of SHS exposure. We used available longitudinal data on exacerbations experienced over follow-up but found no significant associations at this point. It will be important to reconsider this question once more complete follow-up data are available after the conclusion of the study to better understand the risk of longitudinal exacerbations associated with SHS exposure. Additionally, though we controlled our models for active smoking in multiple ways, we acknowledge the possibility of residual confounding. Finally, as with many observational studies with multiple clinical outcomes of interest, we are limited by the number of statistical comparisons made in that this can increase the possibility of a type I error. Despite this, the consistency of our findings for the comparisons made is notable. Limitations can be addressed as more longitudinal data become available in SPIROMICS. Our findings are relatively generalisable to the population with COPD in the USA, owing to the diversity and broad range of disease in SPIROMICS.
In summary, using the well-characterised COPD cohort in SPIROMICS, we have shown that SHS exposure is common, impacting over a quarter of the population with COPD. Such exposure is associated with higher risk of adverse outcomes in former smokers and in those currently smoking, and also with a distinct pattern on CT indicative of heightened airway inflammation. Finally, we have shown that SHS has important impacts on obese individuals and surprisingly also current active smokers, findings which challenge us to further understand the mechanisms responsible for adverse outcomes in COPD associated with SHS exposure.38
Acknowledgments
The authors thank the SPIROMICS participants and participating physicians, investigators and staff for making this research possible. More information about the study and how to access SPIROMICS data is at http://www.spiromics.org. They would like to acknowledge the following current and former investigators of the SPIROMICS sites and reading centres: Neil E Alexis, PhD; Wayne H Anderson, PhD; R Graham Barr, MD, DrPH; Eugene R Bleecker, MD; Richard C Boucher, MD; Russell P Bowler, MD, PhD; Elizabeth E Carretta, MPH; Stephanie A Christenson, MD; Alejandro P Comellas, MD; Christopher B Cooper, MD, PhD; David J Couper, PhD; Gerard J Criner, MD; Ronald G Crystal, MD; Jeffrey L Curtis, MD; Claire M Doerschuk, MD; Mark T Dransfield, MD; Christine M Freeman, PhD; MeiLan K Han, MD, MS; Nadia N Hansel, MD, MPH; Annette T Hastie, PhD; Eric A Hoffman, PhD; Robert J Kaner, MD; Richard E Kanner, MD; Eric C Kleerup, MD; Jerry A Krishnan, MD, PhD; Lisa M LaVange, PhD; Stephen C Lazarus, MD; Fernando J Martinez, MD, MS; Deborah A Meyers, PhD; John D Newell Jr, MD; Elizabeth C Oelsner, MD, MPH; Wanda K O'Neal, PhD; Robert Paine, III, MD; Nirupama Putcha, MD, MHS; Stephen I. Rennard, MD; Donald P Tashkin, MD; Mary Beth Scholand, MD; J Michael Wells, MD; Robert A Wise, MD and Prescott G Woodruff, MD, MPH. The project officers from the Lung Division of the National Heart, Lung, and Blood Institute were Lisa Postow, PhD, and Thomas Croxton, PhD, MD.
References
Footnotes
Contributors All authors contributed to data analysis and interpretation, critical revisions of intellectual contact, approval of the version to be published and all authors are accountable for all aspects of this work.
Funding NP was supported by the Johns Hopkins University Clinician Scientist Award, the Pearl M. Stetler Research Foundation Award during the conduct of this work and is currently supported by NIH/NHLBI 5K23HL123594-02. SPIROMICS is funded by the National Heart, Lung, and Blood Institute (NHLBI) of the NIH, contract and grant numbers: HHSN268200900013C, HHSN268200900014C, HHSN268200900015C, HHSN268200900016C, HHSN268200900017C, HHSN268200900018C, HHSN2682009000019C and HHSN268200900020C, which were supplemented by contributions made through the Foundation for the NIH from AstraZeneca; Bellerophon Pharmaceuticals; Boehringer-Ingelheim Pharmaceuticals; Chiesi Farmaceutici SpA; Forest Research Institute; GSK; Grifols Therapeutics; Ikaria; Nycomed GmbH; Takeda Pharmaceutical Co; Novartis Pharmaceuticals Corp; Regeneron Pharmaceuticals and Sanofi.
Competing interests DPT has provided consulting services for AstraZeneca, Sunovion, Mylan, Novartis, Glenmark, Theravance; has been a speaker for AstraZeneca, Sunovion and Boehringer-Ingelheim and has received research grants from Boehringer-Ingelheim, Sunovion and GlaxoSmithKline. The remainder of the authors report no significant interests to disclose.
Ethics approval Institutional review boards at all respective clinical sites for SPIROMICS: Johns Hopkins University, Columbia University, University of Utah, University of California San Diego, National Jewish Hospital, University of Alabama Birmingham, University of North Carolina, Wake Forest University, University of Michigan, Temple University, University of Illinois, University of Iowa and University of California Los Angeles.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data used in the present study are from an ongoing prospective cohort study of COPD. Persons interested in using data from this studies should contact the corresponding author or visit the study website.