Article Text

Statistics from Altmetric.com
Happy 70th birthday Thorax
March 1946 saw the appearance of new journal, from the Association for the study of Diseases of the Chest, edited by Norman Barrett and J G Scadding. Thorax was born. In 1946, a year's subscription cost 25 shillings and each edition contained 4–5 original manuscripts. Seventy years and 603 issues later, Thorax publishes around 10 original manuscripts per issue (along with editorials, reviews and education pieces) and costs rather more for a year's subscription. This month in the journal, we celebrate the 70th birthday of Thorax and the contribution of the exceptional clinicians and scientists who have published in the journal over the years. In this issue, former editors Anne Tattersfield (1987–91) and Anthony Seaton (1977–82), aided by an ensemble of previous editors, recount the history of Thorax through a selection its most influential papers (see page 203, Editors' choice). The last 70 years have seen huge advances in the treatment of tuberculosis, the prevention of occupational and smoking related lung disease and significant steps in improving the care of people with asthma, COPD and cystic fibrosis. We believe Thorax has played an important part in these achievements and we thank the previous editors, editorial teams and contributors to the journal.
Blood gases without tears?
Having arterial blood sampling is one of the more unpleasant aspects of a hospital admission for an exacerbation of COPD. On page 210 of the journal, Tricia McKeever and colleagues commit the heresy of asking if this unpleasant and painful procedure adds additional information. They conclude that venous samples are significantly less painful and perform well in comparison with arterial samples for pH and bicarbonate measurement. In a linked editorial, Andrew Hitchings and Emma Baker applaud the approach but suggest that venous sampling is not yet ready to take the place of the arterial stab and that a randomised trial of treatment directed by venous sampling is needed (see page 208).
What is the point of intravenous antibiotics in CF?
To paraphrase Jane Austen: “It is a truth universally acknowledged, that a cystic fibrosis patient in possession of a pulmonary exacerbation must be in want of a two week course of intravenous antibiotics.” The two week course of “IVs” is another sacred ritual of chest medicine and one under pinned by little evidence. On page 223 of the Journal, Sonya Heltshe and colleagues describe the discordant clinical outcomes from intravenous antibiotic courses in 123 CF patients. Smaller improvements in FEV1 were associated with failure to recover baseline lung function but, paradoxically, were also associated with a longer interval before the next IV treatment. Symptomatic improvement was not associated with either increment in lung function or time to next IV treatment!
“Prediction is very difficult, especially if it's about the future”
Niels Bohr may or may not have made this absurdist statement about prognostication. However, predicting pulmonary exacerbations in CF might lead to earlier treatment and better outcome (retarding long term deterioration in lung function). On page 216 of this month's Thorax, Bradley Quon and colleagues describe novel plasma protein biomarkers which can predict exacerbations in CF. They use a combination of discovery and replication cohorts (104 patients in total) to identify a panel of 6 biomarkers which have 90% sensitivity and 45% specificity for predicting exacerbations within 4 months. However, this is only slightly better than CRP (a more familiar biomarker) that has a sensitivity of 90% and specificity of 35%. As well as further replication and validation, the authors propose a future clinical utility study.
More prognostication from British Colombia – on page 267 of the Journal, Wenjia Chen and colleagues report findings from an administrative database of over 13,000 individuals, classified as having severe asthma. What happened next? Improvement was seen in 83% of patients (transitioning to moderate or mild status) 10 years after incident severe asthma. Poor prognostic factors were low socioeconomic status, co-morbidity and adherence. What? The latter is likely to be confounding by reverse causation.
Lung cancer – an Italian job?
There are a number of reasons why one might want to live in Varese (Northern Italy), rather than the UK: the climate, the food, and the quite extraordinary number of professional cyclists who live there (including the veteran Stefano Zanini)–to name but a few. However, a comparative study, performed in 2000, showed that earlier treatment on lung cancer was a further advantage (compared with Teeside in the UK). In this month's Thorax this comparison is revisited (see page 230). In both the UK and Varese, emergency resections have declined and performance status has improved. However the resection rate in Teeside (whilst improving from 7% to 11%) has still not reached the 24% rate in Varese and fewer cancers in Teeside are early stage.
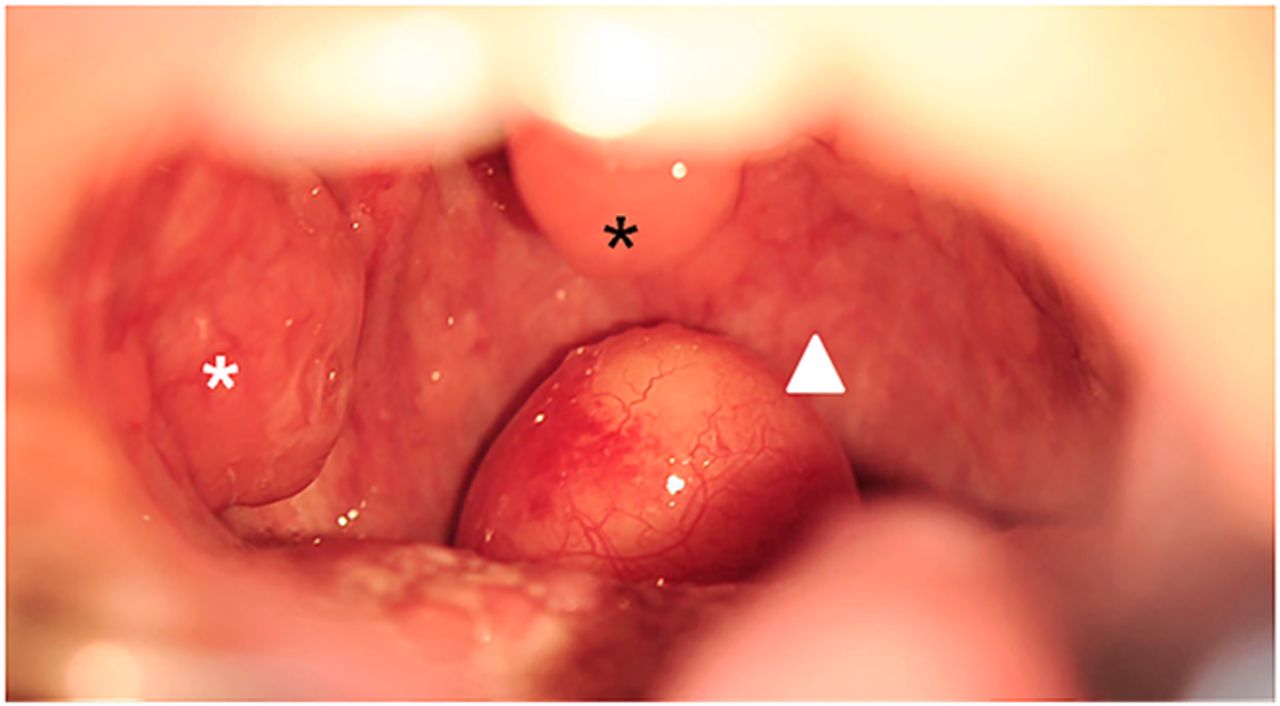
Stick out your tongue and say aaahhh…
Traditional teaching is that respiratory examination should include examination of the airway from mouth (or anterior nares) to alveolus. So having a good look in the throat may avoid missing an important diagnosis. See this month's image and test your diagnostic skills when faced with something nasty in the posterior pharynx (see page 294).⇓

{kind=link}
Linked Articles
- Cystic fibrosis
- Cystic fibrosis
- Chest clinic
- Lung cancer
- Editorial
- Chronic obstructive pulmonary disease
- Editorial
- Respiratory epidemiology