Article Text

Abstract
Background Hospitalisation due to acute exacerbations of COPD (AECOPD) is common, and subsequent mortality high. The DECAF score was derived for accurate prediction of mortality and risk stratification to inform patient care. We aimed to validate the DECAF score, internally and externally, and to compare its performance to other predictive tools.
Methods The study took place in the two hospitals within the derivation study (internal validation) and in four additional hospitals (external validation) between January 2012 and May 2014. Consecutive admissions were identified by screening admissions and searching coding records. Admission clinical data, including DECAF indices, and mortality were recorded. The prognostic value of DECAF and other scores were assessed by the area under the receiver operator characteristic (AUROC) curve.
Results In the internal and external validation cohorts, 880 and 845 patients were recruited. Mean age was 73.1 (SD 10.3) years, 54.3% were female, and mean (SD) FEV1 45.5 (18.3) per cent predicted. Overall mortality was 7.7%. The DECAF AUROC curve for inhospital mortality was 0.83 (95% CI 0.78 to 0.87) in the internal cohort and 0.82 (95% CI 0.77 to 0.87) in the external cohort, and was superior to other prognostic scores for inhospital or 30-day mortality.
Conclusions DECAF is a robust predictor of mortality, using indices routinely available on admission. Its generalisability is supported by consistent strong performance; it can identify low-risk patients (DECAF 0–1) potentially suitable for Hospital at Home or early supported discharge services, and high-risk patients (DECAF 3–6) for escalation planning or appropriate early palliation.
Trial registration number UKCRN ID 14214.
- COPD Exacerbations
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is the key question?
Does the DECAF score predict inhospital mortality in patients admitted to hospital with an acute exacerbation of COPD?
What is the bottom line?
In both internal and external validation cohorts, DECAF is a robust predictor of inhospital mortality using indices that are routinely available at the time of admission, and can be easily applied at the bedside.
Why read on?
Accurate risk stratification may be used to inform clinical decision-making, although further research is required to quantify the impact on clinical and financial outcomes.
Introduction
Acute exacerbations of COPD (AECOPD) account for one in eight hospital admissions,1 and are associated with worsening symptoms, lung function, health-related quality of life, and mortality risk.2–6 Inhospital mortality is reported to be between 4.4% and 7.7%.7–10 Clinicians are unable accurately to predict prognosis in patients hospitalised with AECOPD.11 A robust prediction tool, which stratifies patients according to mortality risk, may help inform management, including Hospital at Home (HAH) or early supported discharge (ESD) for low-risk groups, and early escalation or appropriate palliation for high-risk groups.
The Dyspnoea, Eosinopenia, Consolidation, Acidaemia, and atrial Fibrillation (DECAF) score was derived in a large cohort of consecutive patients hospitalised with AECOPD, is simple to apply at the bedside and predicts inhospital mortality using indices routinely available on admission.12 The score comprises five predictors, the strongest of which is stable state dyspnoea, as measured by the extended Medical Research Council Dyspnoea score (eMRCD; table 1).13
eMRCD score, guidance note for eMRCD and DECAF score
In the derivation study (the original study, in which the DECAF score was developed), DECAF showed strong performance and was superior to other tools designed or proposed for patients with AECOPD,12 namely APACHE II,14 BAP-65,15 CAPS16 and CURB-65.17
The 2014 UK National COPD audit recommended that the DECAF score be documented on all patients admitted with an AECOPD but noted that validation was required,7 which is essential to prove the generalisability of a prognostic score.18 We present temporal and geographical validation of the DECAF score and re-examine its predictive performance for short and medium term mortality in a large multicentre cohort of patients hospitalised with AECOPD. Two cohorts are presented: the internal validation cohort assesses performance of DECAF in both hospitals from the original derivation study, but over a different time period; the external validation study assesses the performance and generalisability of DECAF in four hospitals from different geographical areas. Since the DECAF score could identify low-risk patients (DECAF 0–1) who might benefit from HAH or ESD schemes, we report a detailed analysis of this subgroup.
Methods
Study design and participation
Six UK hospitals participated between January 2012 and May 2014. Sites A and B formed the internal validation cohort and sites C–F formed the external validation cohort (table 2). The latter were selected to ensure wide variation in structures of care and population characteristics (COPD prevalence, socioeconomic factors and rurality). In participating hospitals, consecutive patients admitted with AECOPD were identified. In the internal validation cohort hospitals, the DECAF indices are recorded as part of routine practice. This allowed the period of the study to be extended retrospectively to enhance recruitment; patients were primarily identified from a broad coding records search (discharge codes). However this was cross-referenced with existing records of patients identified by respiratory specialist nursing and physiotherapy teams. In the external validation cohort to identify consecutive admissions of patients with AECOPD, all medical admissions were screened prospectively. This involved dedicated staff attending the medical admissions unit and base wards. Coding records were also reviewed to maximise patient capture.
Baseline characteristics of patients by site
Inclusion criteria were: a primary diagnosis of pneumonic or non-pneumonic exacerbation of COPD; preadmission spirometric evidence of airflow obstruction; age ≥35 years and smoking history of ≥10 cigarette pack-years. Exclusion criteria were: previous inclusion in the present study and any illness, other than COPD, likely to limit survival to less than 1 year (principally metastatic malignancy). Spirometry showing airflow obstruction performed at any time point prior to admission was accepted, and both primary and secondary care records were searched.
Treatment was at the discretion of attending clinicians, and not influenced by the research team. Antibiotic therapy was informed by the prescribing policy of individual sites. Ethical approval was granted by the local research ethics committee.
Data collection
Clinical indices on admission, and demographic and survival data were collected.12 In our derivation study,12 118 patients had oxygen saturation (SpO2) >92% while breathing room air, of whom none had an arterial pH of <7.30 (DECAF acidaemia score=1). In the present study, therefore, if the attending physician deemed that arterial blood gas (ABG) sampling was unnecessary and SpO2 was >92% without supplementary oxygen, it was presumed that the arterial pH was ≥7.30.19
Outcome
The primary outcome was inhospital mortality prediction, with comparison of DECAF risk groups between the derivation and validation cohorts. Secondary outcomes included assessment of the optimal thresholds for pH and eosinopenia, prediction of 30-day mortality by DECAF and comparison with other prognostic scores (APACHE II,14 BAP-65,15 CAPS16 and CURB-6517). Length of stay (LOS) was compared across DECAF scores.
Statistical methods
Based on an expected sensitivity of 70%, an SE of the estimate of sensitivity of 5% required a minimum of 840 patients in both the internal and external validation cohorts.20 For indices with <20% missing values, data were imputed using the Markov Chain Monte Carlo method on IBM SPSS Statistics 22, with linear and logistic regression for continuous and categorical variables.21 A large number of variables (n=67) were used as predictors for variables with missing data to create five datasets.
Baseline population characteristics and outcome were described using proportions, means with SDs or medians with IQRs, and compared using Fisher's exact test, analysis of variance or Welch, and Kruskal–Wallis test. Clinical scores’ performance was assessed by the area under the receiver operator characteristic (AUROC) curve and compared with each other by the method of DeLong with and without multiple imputation;22 results were pooled using Rubin's method.21 Logistic regression was used to model DECAF indices to provide ORs, 95% CIs and coefficients to assess the weighting of indices. Calibration was assessed with the Hosmer–Lemeshow statistic.23 The optimal thresholds for pH and eosinophil count were reassessed by visual inspection of the ROC curve. Subgroup analyses assessed outcome in patients at low risk according to DECAF, with (a) coexisting consolidation or (b) acidaemia.
Results
Patient characteristics
Data were obtained for 880 and 845 patients in the internal and external validation cohorts, respectively. Across both cohorts, mean (SD) age was 73.1 (10.3) years, 54.3% were female and most had severe airflow limitation; mean (SD) FEV1 45.5 (18.3) per cent predicted. The median DECAF score was 2 (IQR 1–3), 28.3% had radiographic consolidation and 18.9% had an acidaemic exacerbation (pH<7.35). In keeping with the UK national audit,7 rates of comorbidity were high, notably ischaemic heart disease and diabetes (table 2).
Significant differences between sites included: the proportion requiring institutional care, radiographic consolidation, age, gender, DECAF score, severity of airflow limitation, the number of previous hospital admissions and the proportion with significant weight loss. Sites were broadly similar for comorbidity, though the proportions with left ventricular dysfunction, anxiety or depression differed. All of these factors were also significantly different between internal and external validation cohorts, except for DECAF score and left ventricular dysfunction.
Missing data
There were no missing mortality or DECAF data. The percentage of complete data for each risk score was: BAP-65 97.2%, CURB-65 96.5%, CAPS 85.9% and APACHE II 73.2%. For individual variables, missing data were PaO2 12.6%, albumin 12.2%, pH 12.1%, GCS 11.7%, potassium 3.3%, confusion 2.6%, temperature 2.6%, mean arterial blood pressure 1.8%, respiratory rate 1.8%, systolic BP 1.7%, diastolic BP 1.7%, heart rate 1.4%, haematocrit 1.2%, creatinine 0.5%, white blood cell count 0.2%, urea 0.1% and sodium 0.1%.
Validation of the DECAF score
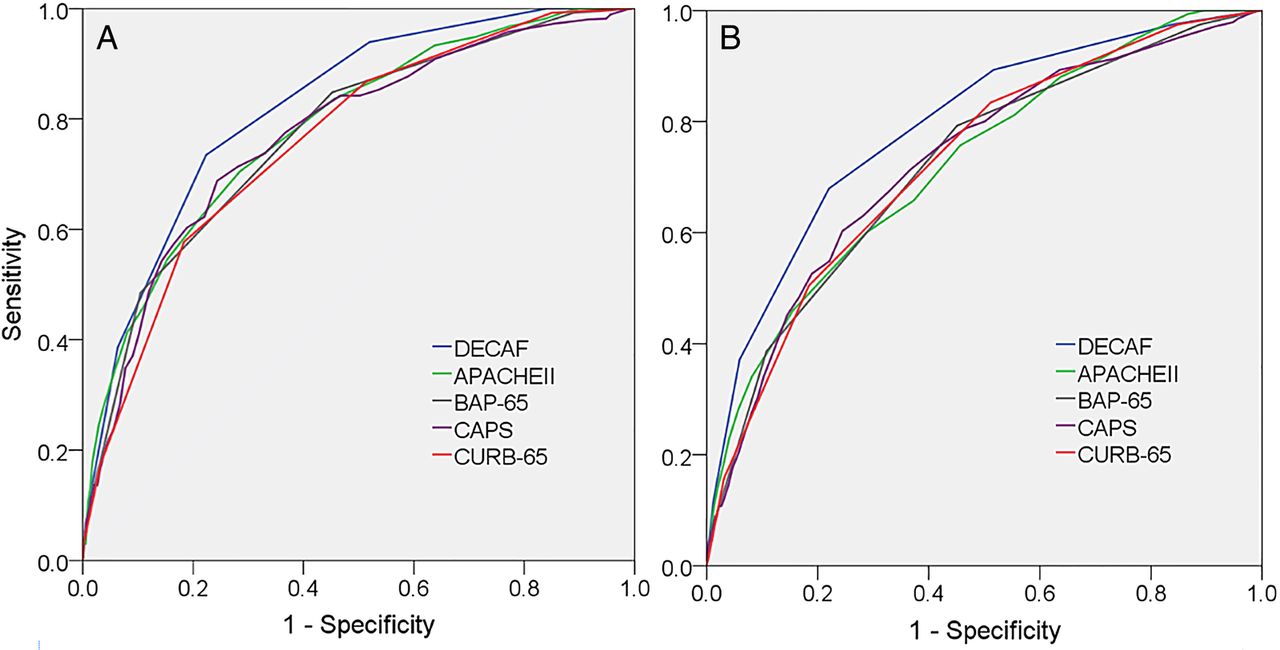
The AUROCDECAF curve for inhospital mortality was: internal validation=0.83 (95% CI 0.78 to 0.87), external validation=0.82 (95% CI 0.77 to 0.87) and overall=0.82 (95% CI 0.79 to 0.85). The discrimination of the DECAF score was significantly stronger than CURB-65, CAPS, APACHE II and BAP-65 for 30-day mortality. For inhospital mortality, the DECAF score was again superior, except in comparison with APACHE II where the higher discriminatory strength of DECAF was not significant (table 3 and figure 1).
Comparison of AUROC curves for DECAF and other scores (with imputation)

Receiver operator characteristic curves of prognostic scores for inhospital (A) and 30-day mortality (B).
In a complete case analysis (without imputation), the conclusions were unchanged for 30-day mortality; for inhospital mortality, AUROCDECAF curve was again the highest, but was not statistically superior to CAPS (p=0.068) or BAP-65 (p=0.060).
Table 4 shows mortality rates, sensitivity and specificity by DECAF score in the overall validation cohort, and mortality by DECAF risk group compared with our derivation cohort.12
DECAF score, inhospital mortality, sensitivity and specificity
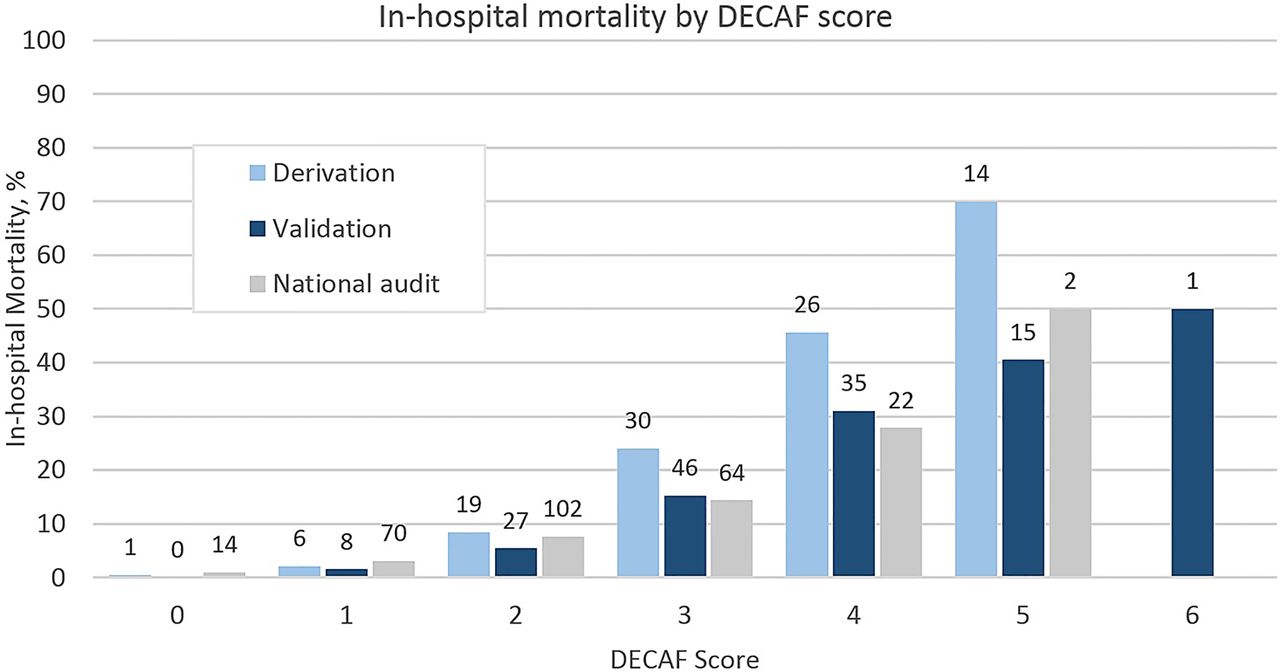
Compared with the derivation study, mortality overall and in the high-risk group was lower. Higher DECAF scores were again associated with higher mortality, though absolute numbers were small for DECAF 5 and 6 groups. The model was a satisfactory fit to the data (Hosmer–Lemeshow statistic=0.48, Nagelkerke R2=24%). The previously assigned weightings of the DECAF score were confirmed on logistic regression (see online supplementary table S1), and eMRCD score remained the strongest predictor.
Compared with the traditional MRCD scale,24 eMRCD had superior prognostic strength for inhospital mortality: AUROCeMRCD=0.74 (95% CI 0.70 to 0.78) versus AUROCtraditional MRCD=0.68 (95% CI 0.64 to 0.72); p<0.0001. In the subpopulation with a pneumonic exacerbation (n=485), eMRCD was again superior to the MRCD scale: AUROCeMRCD=0.67 (95% CI 0.60 to 0.73) versus AUROCMRCD=0.62 (95% CI 0.56 to 0.69); p=0.0070.
CURB-65 predicts 30-day mortality in patients with community acquired pneumonia, and is commonly applied to patients with a pneumonic exacerbation of COPD (pAECOPD). In the validation cohort, for the subgroup of patients with pAECOPD (n=489), the DECAF score was a non-significantly stronger predictor of 30-day mortality than CURB-65: AUROCDECAF=0.76 (95% CI 0.70 to 0.81) versus AUROCCURB-65=0.68 (95% CI 0.62 to 0.74); p=0.057 (figure 2; online supplementary table S2 shows sensitivity and specificity for DECAF scores).

Receiver operator characteristic curves of prognostic scores for 30-day mortality in patients with pneumonic exacerbations (n=489).
When patients with pAECOPD were pooled across the derivation and validation cohort (n=788), DECAF was superior for 30-day (AUROCDECAF=0.75 (95% CI 0.71 to 0.79) vs AUROCCURB-65=0.66 (95% CI 0.62 to 0.71); p<0.0001) and inpatient mortality (AUROCDECAF=0.76 (95% CI 0.71 to 0.80) vs AUROCCURB-65=0.70 (95% CI 0.65 to 0.75); p=0.024). The superior performance of DECAF is of particular importance for patients deemed at low risk by each score, who may be considered suitable for home treatment. Patients with a low-risk DECAF score had a lower inhospital mortality compared with those with a low-risk CURB-65 score: DECAF=1.6% (2/122) versus CURB-65=7.2% (17/237); p=0.026. There were similar differences for 30-day mortality: DECAF 0–1=3.3% (4/122) versus CURB-65 0–1=10.1% (24/237); p=0.022 (see online supplementary table S3).
The optimal thresholds for eosinophil count and pH were reassessed. On visual inspection of the ROC curve, the optimal cut-off for eosinopenia was unchanged (0.05×109/L).12 For pH threshold, both 7.30 and 7.35 offered similar discrimination. The 7.30 threshold identified in the derivation study was retained for consistency, and because no deaths occurred among 58 patients with a low-risk DECAF score and non-scoring acidaemia (7.30-7.34). Only three patients had a DECAF score of 1 due to a pH<7.30, all of whom survived.
Patients with SpO2 >92% without supplemental oxygen in whom ABG sampling was deemed unnecessary were assigned a score of 0 for the pH component of DECAF. Of the 209 such patients overall, only 6 died (2.9%); this total included 0/52 with a DECAF score of 0 and 2/67 with a DECAF score of 1.
Time to death in those who died during the index admission and LOS in those who survived to discharge, by DECAF score, are shown in table 5. Among survivors, higher DECAF scores were associated with longer LOS.
Time to death in patients who died during the index admission and median length of stay in those who survived to discharge, by DECAF score
Discussion
In a large, multicentre study of patients admitted with AECOPD, we have confirmed that the DECAF score is a robust predictor of mortality that can be easily scored at the bedside using indices routinely available on admission. As in our earlier study, DECAF was superior to other scores (BAP-65, CAPS, APACHE II, CURB-65) sometimes used to predict short-term mortality of patients with AECOPD.
We went to considerable lengths to capture consecutive patients, but a small number of patients who died or who were discharged shortly after admission may have been missed. In order to minimise any resulting bias and to maximise capture of all eligible patients, admission units were screened and a broad coding records search was performed. In the 2014 UK national audit,7 mean site recruitment of patients with spirometric confirmation of COPD was 0.36 per day. In our study, recruitment was substantially higher at all sites (table 2), which supports high case ascertainment rates. Investigators in site E reported problems obtaining spirometry results, which may in part explain their comparatively lower recruitment rate.
The CHARMS checklist provides guidance on the appraisal of prediction model studies (see online supplementary material).18 The main limitation of this study is that the internal validation study was, in part, performed retrospectively. Although retrospective collection of data may bias results, this risk was mitigated as the DECAF indices were collected as part of routine clinical practice in the participating hospitals, the researchers extracting data were blinded to outcome and case ascertainment and outcome were similar to the prospective external cohort. Of importance, the latter was individually adequately powered.
Data were only regarded as ‘missing’ once all data sources had been checked and rates of missing data were low. For key outcomes, analyses were repeated with and without multiple imputation. To improve data completeness for DECAF, patients with SaO2 >92% breathing room air, and judged by a clinician not to require ABG analysis, scored 0 for the acidaemia component of DECAF; this was justified by the low mortality in this group, and supports a similar pragmatic approach in the clinical application of the score, reducing burden for both patients and clinicians. However, we do not advise that this assumption is used to lower clinician's threshold for performing ABG sampling.
There were important differences between site populations, in particular the receipt of institutional care, coexistent consolidation, degree of airflow obstruction and severity of DECAF score. This may in part reflect our efforts to select diverse sites for participation in the study, and the strong and consistent performance of DECAF, despite such differences in baseline characteristics, emphasises the external validity of the score.
Mortality varied between sites (from 4.7% to 9.8%) and between cohorts (internal validation=8.9% vs external validation=6.4%; p=0.057). This largely reflects differences in baseline characteristics, notably the proportion of patients admitted from institutional care and with coexistent pneumonia. When these two subgroups were excluded, mortality was 4.8% in both cohorts. Overall mortality was 7.7%, which is in keeping with the 2003 (7.7%) and 2008 (7.8%) UK national audits. In the 2014 UK audit, mortality was 4.3% though the reason for the lower mortality rate is reported as unknown. In our study, case ascertainment, comorbidity and the proportion of patients with consolidation or an MRCD score of 5 was higher than in the 2014 UK national audit.
Since our 2012 DECAF derivation study, two further prognostic scores have been published.25 ,26 In one,25 patients with acute ECG features of ischaemia and radiographic pulmonary congestion were included. Such patients are unlikely to have met our inclusion criterion of a primary diagnosis of AECOPD.
In the second study, the derived score showed good discrimination, and validation is awaited.26 However, the score included subjective recognition of ‘use of inspiratory accessory muscles or paradoxical breathing’, reducing generalisability, especially in healthcare settings which lack specialist review within 24 h of admission.7 ,27 Recruitment was lower than equivalent audit data,27 because written patient consent was required, which disproportionately excludes the lowest and highest risk patients. Our methodology mirrored UK national audits; only routine data were collected, so patient consent was not required.
LOS for AECOPD is falling, and early discharge, both supported and unsupported, is commonplace, with patient selection based largely on clinical judgement. However, clinical judgement of prognosis is poor11 while the DECAF score has consistently shown a high sensitivity for identifying low-risk patients. ESD and HAH services for patients with AECOPD are expanding.7 National Institute for Health and Care Excellence (NICE) recommend that patient selection for these services be based on mortality risk,28 and also highlight the (previous) lack of a robust prognostic score to guide decision-making. In the present study, DECAF 0–1 patients (including those with pneumonia or acidaemia) had an acceptably low mortality risk and comprised 45% of patients. The effect of treating this group with HAH or ESD requires a randomised controlled trial (RCT) to assess clinical outcomes and associated costs. We are currently undertaking an RCT to address this question (ISRCTN 29082260). In our experience, the CURB-65 score is commonly applied in patients with pneumonic exacerbations of COPD to inform discharge planning and choice of antibiotics. Evidence from both the derivation and validation studies shows that clinicians should not be reassured by ‘low risk’ CURB-65 scores in patients with pneumonic AECOPD as the associated mortality is unacceptably high. We advise against its use in this population.
A high-risk DECAF score is associated with both a high risk of death and, in those who die, a short time to death. The latter is particularly true of patients scoring DECAF 5 or 6, in whom the median time to death was only 2 days. Such patients may be suitable for early escalation in care, or alternative palliative care, but the window for intervention is short. Among patients who survive to discharge, LOS increases incrementally with DECAF score.
In both the derivation and present study, dyspnoea severity measured by the eMRCD score was the strongest single predictor of mortality and a superior predictor to the traditional MRCD scale. In the 2014 UK national audit, ‘DECAF light’ was scored retrospectively using the traditional MRCD scale (see figure 3). However, ‘DECAF light’, as opposed to the full DECAF score, was calculated only because eMRCD data was unavailable. We support the recommendation of the UK national audit that DECAF indices, including the eMRCD score, be collected on all patients admitted with AECOPD. To allow hospitals to meet this recommendation, we have included a figure of the DECAF score which can be downloaded and incorporated into COPD bundles and admission documentation (online supplementary figure 1). Various versions of the traditional MRCD scale exist,24 ,29 ,30 which may lead to differences in scoring. We caution against such modifications to the eMRCD score unless supported by empirical evidence.

{kind=link}
{kind=link}
{kind=link}
Inhospital mortality (percentage and absolute number) in the DECAF derivation and validation study, and ‘DECAF light’ (see discussion) from the 2014 UK National COPD Audit.
In conclusion, we have shown that DECAF can be used in a variety of hospital settings in order accurately to stratify mortality risk in patients with AECOPD. Further research is required to quantify its impact on clinical practice, for example, in the identification of patients for HAH or ESD services.
Acknowledgments
We are grateful to Victoria Ferguson for her input with data management. We are thankful for the hard work of the research and clinical teams collecting data at each site, including Stephen Gundry, Maureen Armstrong, Peter Fenwick, Liz Norman and her team, Nicola Bateman, June Battram, Angela Scott-Johnson and Valerie O'Dwyer.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors SCB designed and obtained funding for the study. CE, GJG and JS contributed to trial design. CE collated the data, performed the statistical analysis and drafted the manuscript. Data analysis and interpretation was supported by SCB, GJG, JS and NS. The manuscript was redrafted by SCB, GJG, JS, AJS and CE. All authors reviewed the manuscript.
Funding This trial was funded by UK Department of Health, Breathe North appeal and Novartis pharmaceutical UK Limited (reference RES12-CO44) and supported by the NIHR Clinical Research Network. CE's salary was funded by the Northumbria NHS Foundation Trust Teaching and Research Fellowship programme.
Competing interests None declared.
Ethics approval NRES Committee North East—Sunderland.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The corresponding author should be contacted if anyone wishes to access unpublished data from the study.