Article Text

Abstract
Background Rapid postnatal weight gain has been associated with wheezing and asthma in children, but it remains unclear whether it acts independently of overweight. We aimed to disentangle the roles of infant's size and weight gain velocity in the development of wheezing in early childhood using a novel method that allows for mutual adjustment for different aspects of growth.
Methods Data were obtained from the NINFEA questionnaires where weight measurements from birth up to 18 months of age were assessed in 4492 term singletons. Wheezing was defined as at least one episode of wheezing/whistling in the chest occurring between 6 and 18 months of age. The SuperImposition by Translation And Rotation model was used to estimate individual weight trajectories defined by three child-specific parameters: size, velocity and tempo, that is age at peak weight velocity. These parameters were standardised and related to wheezing using logistic regression with effects expressed as an increase of one SD.
Results A median of five weight measurements per child were obtained. Infant size (OR=1.28; 95% CI 1.12 to 1.46) and weight gain velocity (OR=1.30; 95% CI 1.15 to 1.48) were independently positively associated with wheezing. We found no evidence of an effect of tempo on infant wheezing. The estimates were changed only minimally after adjustment for potential confounders.
Conclusions Faster growth and larger size in the first 18 months of life are both independently associated with an increased risk of wheezing. These findings suggest that early growth patterns play a role in shaping the occurrence of wheezing.
- Paediatric asthma
- Asthma Epidemiology
- Asthma Mechanisms
Statistics from Altmetric.com
Key messages
What is the key question?
Do infant size and weight gain velocity act independently on the development of wheezing in early childhood?
What is the bottom line?
Larger size and postnatal weight gain velocity are independent risk factors for the development of wheezing in children aged ≤18 months.
Why read on?
This study provides evidence, obtained using a novel growth modelling approach, that fast weight gain and large size in infancy increase the risk of early childhood wheezing independently.
Introduction
Early-life exposures have been found to play an important role in the development of respiratory morbidity in children and adults.1 ,2 In recent years, a number of studies reported positive associations between early rapid weight gain and the development of childhood wheezing and asthma.3–11 However, other studies did not replicate these findings,12–14 and the association between rapid weight gain and lung function was inconsistent.6 ,9 ,15 ,16 In addition to overweight and obesity,17 postnatal growth velocity is therefore considered to be a potential, yet unconfirmed, important factor in the development of respiratory diseases in children.
The increased risk of wheezing in overweight children could be explained by a direct mechanical effect on the lungs and/or by a low-grade systemic inflammation caused by abnormal circulating levels of pro-inflammatory factors, such as leptin and adiponectin, associated with overweight.17 Conversely, the mechanisms underlying the association between early rapid growth and respiratory disorders are less clear and might reflect confounding by fetal exposures or a direct adverse effect of an unbalanced somatic versus lung growth.
As different growth features are entangled aspects of the overall growth pattern, it remains unclear whether child's size and its changes over time act as independent risk factors for the development of wheezing or are just two correlated indicators. Many studies addressing this issue were based on rather simple growth modelling,3 ,5 ,6 ,8 ,12 ,14 ,15 evaluating the difference in two growth measurements, usually expressed as change in weight/weight for length or body mass index (BMI) SD z scores. Some other studies used more complex growth models considering different patterns of early growth trajectories.4 ,7 ,9 ,10 ,11 ,13 ,16 In order to assess whether the effect of early growth on the occurrence of asthma-like conditions was mediated through current weight/BMI status, some studies accounted for weight/BMI at the age of outcome assessment. However, weight measured at one time point represents only a snapshot of the individual's overall size and might not capture its full effect on the relationship between early weight gain and respiratory outcomes.
The aim of the present study was to examine the effects of child's size and velocity of weight gain over the first 18 months of life on the development of wheezing between 6 and 18 months of age. We addressed this by modelling weight data with the SuperImposition by Translation And Rotation (SITAR) method18–20 that estimates individual weight trajectories through three biologically interpretable subject-specific parameters—child's size, and velocity and tempo of weight growth.
Methods
Study population
The NINFEA study is an ongoing internet-based birth cohort established in 2005 in Italy (http://www.progettoninfea.it).21 ,22 The cohort consists of children born to mothers who have access to the internet and enough knowledge of Italian to complete online questionnaires. The recruitment is conducted actively, through obstetrics clinics, and passively, via internet and the media.23 Approximately 75% of participants are recruited actively, 20% passively and 5% comprise both modes. A baseline questionnaire on general health and exposures before and during pregnancy is completed by mothers at enrolment, which may occur at any time during pregnancy. Further follow-up information is obtained with repeated questionnaires completed 6 and 18 months after delivery and when children turn 4 and 7 years. For the present study, we retrieved weight measurements, information on the occurrence of wheezing and potential confounding factors from the first three questionnaires using the 2016.02 version of the NINFEA database. The response rate at the 18-month questionnaire is 82.5%.
The study population consisted of 4492 term singletons with at least one weight measurement within the first 18 months of life and information on the occurrence of wheezing in the 18-month questionnaire. We examined only infants born at term (at least 37 weeks of gestation) as wheezing and postnatal growth patterns related to prematurity likely have different mechanisms compared with those of full-term infants.8
The study was approved by the Ethical Committee of the San Giovanni Battista Hospital and CTO/CRF/Maria Adelaide Hospital of Turin (approval N.0048362 and following amendments) and all the participants gave informed consent at enrolment.
Anthropometric measurements
Child's birth weight and weights at 3 and 6 months of age were ascertained from the 6-month questionnaire, while weights at 12 and 18 months of age were obtained from the 18-month questionnaire. After the enrolment of the first 1500 mothers, the NINFEA questionnaires were revised and additional questions on child's weight at the exact time of the completion of each questionnaire were included. This led to a median of five measurements per child (range 1–6).
Although childhood growth is usually assessed by both weight and height/length measurements, in this study we focused on weight only due to its rapid change in the first years of life.24 Moreover, in the NINFEA cohort the response rate for weight was higher compared with the length/height measurements.
Children in Italy are measured regularly by health professionals who, in most of the Regions, record weights in children's personal health booklets. Mothers enrolled after the revision of the questionnaires also reported how weight measurements were recalled. The percentage of mothers who used booklets to report child's weight varied from 85.0% for the measurement at 3 months of age to 62.1% for the measurement at 18 months of age.
An internal validation study comparing self-reported birth weight from the NINFEA cohort and information from the Piedmont Birth Registry available for 1160 children showed good agreement across all the levels of birth weight.25
Outcome and confounding factors
Wheezing was assessed from the 18-month questionnaire and was defined as at least one episode of wheezing or whistling in the chest that occurred between 6 and 12 months of age. As we used parent-reported wheezing, mothers were additionally asked if a paediatrician confirmed the symptoms, with 90.1% of mothers confirming a doctor's diagnosis of wheezing.
For the subset of children enrolled after the revision of the questionnaires (N=3006), information on the medications used to treat wheezing, reported by mothers as free text, was also available. Medications were coded as bronchodilators, corticosteroids and other medications, and only children who had wheezing treated with inhaled bronchodilators, corticosteroids or both were coded as cases (9.8%).
The following potential confounding factors were pre-selected and included in the final models: maternal age at delivery, maternal educational level (low—primary school or less, medium—secondary school, and high—university degree), maternal nationality (Italian or other), maternal history of asthma, maternal pre-pregnancy body mass index (BMI), maternal smoking during pregnancy, child's sex, gestational age, siblings, lower respiratory tract infections (bronchitis, bronchiolitis and pneumonia) between 6 and 18 months of age and maternal smoking in the first 18 months after delivery as a proxy of child's exposure to passive smoking.
Statistical analyses
Statistical analyses comprised two stages. The first stage involved growth modelling by using the SITAR method,18–20 while the associations between growth parameters and infant wheezing were estimated in the second stage using standard methods.
Individual weight trajectories were identified using the SITAR method,18 ,19 which has already been applied to the NINFEA cohort data.20 ,26 This is a shape invariant random-effects model that estimates a population growth curve using a spline function and a set of three subject-specific growth parameters: size, tempo and velocity. These three parameters transform the average growth curve to match each individual’s growth trajectory. In order to meet the distributional assumptions of the model, weight was log transformed, and thus, size is expressed in the units of log-grams. Tempo is expressed in months, while velocity is a fractional multiplier and therefore is scale free. Briefly, size represents an up/down shift of each curve and takes positive values for children heavier than the population ‘average child’; tempo is a left/right shift of the curve and corresponds to earlier or later timing of the peak weight velocity; while velocity is a shrinking/stretching of the age scale that alters the slope and is positive for children with faster growth across the entire period.19
Due to the lack of measurements between birth and 3 months of age in the NINFEA cohort, the model that included size, tempo and velocity did not lead to estimation convergence. To adapt the SITAR method to the NINFEA weight data, we had to introduce a constraint on the fixed effect of the tempo parameter by setting it to be equal to zero, as previously described.20 ,26 The estimated individual growth trajectories were adjusted for child's sex and the natural cubic spline function of age (with B-spline basis) was fitted by placing three internal knots at tertiles of the age distribution. For each child the estimated size, tempo and velocity random effects were then extracted, standardised and used as explanatory variables for the second stage of the analysis.
In the second stage of the analysis, we used logistic regression to estimate the associations between the derived growth parameters and infant wheezing. Since mothers could participate in the NINFEA cohort with more than one pregnancy, robust variance was estimated using clustered sandwich estimators to allow for intra-group correlation. To account for the uncertainty arising from the two-stage analysis, ORs and corresponding 95% CIs were calculated by using the mean and SD of 1000 bootstrap replications. Two models were fitted: the minimally adjusted model (the growth parameters mutually adjusted and adjusted for child's sex in the first stage analysis); and the fully adjusted model (the minimally adjusted model additionally adjusted for the pre-selected confounding factors). The growth-wheezing effects estimated in the second stage of the analysis are expressed as an increase of one SD.
To test the performance of the SITAR model with richer data, the analyses were also performed on subjects for whom at least five weight measurements were available (N=3196). A possible nonlinear relationship between the growth parameters and the risk of wheezing was modelled using restricted cubic splines (with three knots). Interactions between size, tempo and velocity were assessed by introducing the interaction term into the regression models. To test whether being born small for gestational age had an impact on the relationship between growth parameters and infant wheezing, we performed a sensitivity analysis by excluding 481 children born small for gestational age (birth weight <10th percentile for gestational age).
The analyses were conducted with the statistical programmes R package 3.1.1 (R Foundation for Statistical Computing, Vienna) and STATA V.13.
Results
A complete case approach was used with 4254 subjects included in the analyses. The percentage of missing data was below 5% for all the explanatory variables (table 1). The children excluded from the analyses because of missing data were more likely to be born from mothers with an asthma diagnosis (p<0.001) compared with the rest of the study population.
Characteristics of the study population
The main characteristics of the study population are summarised in table 1. The prevalence of early childhood wheezing was 17.3%.
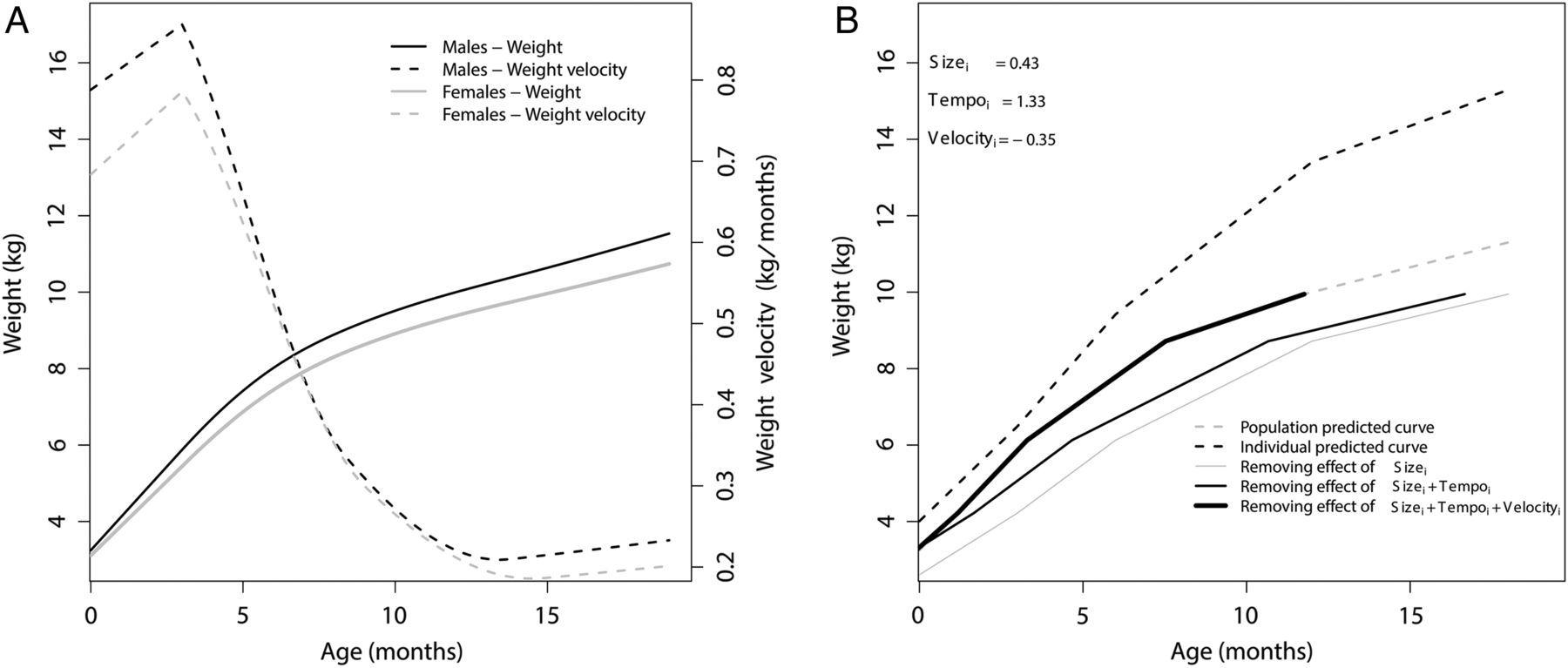
The estimated population weight and velocity curves modelled with the SITAR method and stratified by gender are shown in figure 1A. These curves represent the fixed effects, that is, when all the random effects are zero. To simplify the understanding of the subject-specific random effects, in panel B of figure 1 we present the growth parameters for a selected male participant whose overall weight was high (positive size parameter), who reached the peak weight velocity considerably late (positive tempo parameter) and whose growth velocity was negative, indicating slower weight gain compared with the population average. It can be seen that when removing the positive size parameter, the individual weight curve (dotted thick line) shifts downward (solid thin line), then, after removing the positive tempo parameter, it shifts to the left (solid medium thick line) and, after removing the negative velocity parameter, it finally shrinks (solid thick line) matching the population predicted growth curve (dotted thin line).

{kind=link}
Weight and velocity curves modelled with the SuperImposition by Translation And Rotation (SITAR) method. (A) The NINFEA population weight and velocity curves stratified by gender. (B) Transformation of the subject-specific weight curve to a population weight curve for a selected male participant. By removing the positive effect of size parameter the individual weight curve (dotted thick line) shifts downward (solid thin line); after removing the positive effect of tempo parameter, it shifts to the left (solid medium thick line); and after removing the negative effect of velocity parameter, it shrinks (solid thick line), matching the population-predicted curve (dotted thin line).
The SD and correlations of the three growth parameters' random effects estimated by the SITAR method are presented in table 2. There was a positive correlation between size and tempo, implying that heavier infants have a later peak in weight gain velocity. On the contrary, the estimated correlations between size and velocity and between velocity and tempo were both negative, suggesting that heavier infants experience slower weight gain velocity, while those with faster growth reach their peak weight gain velocity at an earlier age.
Summary statistics of the growth parameters’ random effects estimated by the SITAR method
The associations between the three estimated growth parameters and infant wheezing are presented in table 3. Both size (OR=1.28; 95% CI 1.12 to 1.46) and weight gain velocity (OR=1.30; 95% CI 1.15 to 1.48) were positively associated with the occurrence of wheezing. There was no effect of the tempo parameter on early childhood wheezing (OR=1.03; 95% CI 0.91 to 1.16). Adjustment for multiple confounding factors led to minimal changes in the estimates (table 3) and the associations remained robust even after exclusion of children born small for gestational age (data not shown). The results were similar when only subjects with a minimum of five weight measurements were analysed (see online supplementary table S1). The three-knot restricted cubic splines analysis revealed a linear relationship between the three growth parameters and the risk of early childhood wheezing (see online supplementary figure S1) and there was no evidence of interaction between size, tempo and velocity on their effect on wheezing (p values for interaction >0.47).
Estimated ORs and 95% CIs for the association between growth parameters and wheezing
Supplementary table
Estimated odds ratios (OR) and 95% confidence intervals (CI) for the association between growth parameters and wheezing in children with at least five weight measurements between birth and 18 months of age.
Supplementary figure
Restricted cubic spline curves showing the model-predicted probability of early childhood wheezing against size (A), tempo (B) and velocity (C) of growth. The solid lines represent the model-predicted probability of wheezing (log [OR]) for a standard deviation (SD) increase in size, tempo and velocity, adjusted for child’s sex, gestational age, lower respiratory tract infections (bronchitis, bronchiolitis and pneumonia), maternal asthma, child’s siblings, maternal pre-pregnancy BMI, maternal smoking during and after pregnancy and maternal nationality, age and education at delivery. Dashed lines represent 95% confidence intervals.
A sensitivity analysis where wheezing treated with bronchodilators and/or corticosteroids was used as an outcome revealed stronger effects of infant size and weight gain velocity (for size, adjusted OR=1.41; 95% CI 1.13 to 1.75; for velocity, adjusted OR=1.46; 95% CI 1.19 to 1.80; for tempo, adjusted OR=1.14; 95% CI 0.91 to 1.43).
Discussion
We evaluated whether growth patterns are associated with the occurrence of wheezing in 18-month-old infants using the SITAR method to model infant weight trajectories. This model enabled us to investigate the independent contributions of specific growth features to the development of wheezing, namely the child's average size (size parameter), weight gain velocity (velocity parameter) and the age at peak weight velocity (tempo parameter). A larger weight over the first 18 months of life was associated with a greater risk of wheezing, and this association remained unchanged after controlling for weight gain velocity, age at peak weight velocity and the potential confounding factors. Furthermore, weight gain velocity was positively associated with wheezing, independently of child's relative size. We found no evidence of an effect of the age at peak weight velocity on infant wheezing.
Several previous studies reported effects of rapid weight gain and larger weight on the development of wheezing in children,3–11 ,27 ,28 but other studies have failed to replicate these findings.12–14 Discrepancies between studies could be partially due to methodological issues, such as different outcome definitions, growth modelling methods and periods of exposure and outcome assessment. Difference in weight/BMI between two time points, as used in many studies, show only partial aspects of growth and might not sufficiently capture different growth trajectories over infancy. In fact, previous studies have not settled the remaining question; that is, whether the increased risk of wheezing and asthma in children is driven by infant size (being big), growing fast or both. In this study, we were able to differentiate three distinct, biologically interpretable features of the overall growth pattern, and to demonstrate their independent effects that might act through different mechanisms on the development of wheezing in children.
Several potential mechanisms may underlie the link between early growth and respiratory diseases in children. An increased weight could favour the development of asthma-like conditions through direct mechanical effects and change in the lung pressures that decrease retractile forces of the lung tissue on the airways, resulting in reduced airway smooth muscles stretching and greater muscle stiffness and narrowing.17 ,29 ,30 Additionally, adiposity-related inflammation and an effect of energy-regulating hormones such as leptin and adiponectin might cause tissue-specific immunological and inflammatory effects with lung and airway remodelling.31 ,32
Our findings indicate that, in addition to increased weight, early weight gain per se is associated with early wheezing in full-term infants, even after exclusion of children born small for gestational age. The biological mechanisms behind this association are less clear. Apart from inflammatory effects caused by adipose tissue accumulation that is associated with fast weight gain and childhood respiratory disorders, it has been suggested that early mismatch between somatic growth and lung development might play an important role.33
Our longitudinal study has an advantage of using a novel approach in growth data modelling. Weight was modelled with a method that estimates three growth parameters: size, tempo and velocity that can be introduced in the mutually adjusted models, providing their individual and independent effects on the occurrence of wheezing. In addition, being a random effects model, the SITAR allows modelling individual weight trajectories for subjects with at least one measurement by ‘borrowing’ information from a nearby subject with similar characteristics under the missing at random assumption. This enabled us to use all available data to model weight trajectories. Furthermore, we took into account strong determinants of an infant's somatic growth and wheezing, including gestational age, maternal BMI, smoking during and after pregnancy, and maternal educational level as a proxy for socioeconomic status, and we found very limited evidence of confounding. Since breastfeeding practice likely acts as an intermediate between early growth and wheezing (ie, mothers may discontinue breastfeeding because of impaired infant growth),34 we did not adjust for this variable in the main analyses. However, breastfeeding could also act as a confounding factor and has been adjusted for in many studies on infant growth. It is reassuring that when we checked whether the assumptions on the role of breastfeeding affected our estimates, we found no differences between the unadjusted and adjusted model (data not shown).
Our study has some limitations. Weight measurements from the NINFEA cohort, like in most of the other previous studies, are concentrated around pre-defined time points, indicating a lack of information from shorter and possibly important intervals, like the first weeks of life. Due to the lack of measurements between birth and 3 months of age, we had to set a constraint on the fixed effect of the tempo parameter that might result in a less precise estimate for this parameter. We did not find that age at peak weight velocity is associated with early childhood wheezing. Although some studies suggested that fast weight gain in the first 3 months of life might be particularly relevant for the development of childhood wheezing/asthma,5 ,6 ,9 other studies also found the same effect when assessing different periods of growth, mostly over the first 2 years of life.3 ,4 ,7 ,8 ,10 ,11
We relied on self-reported data when defining infant wheezing, an approach that is not free from criticism but is widely and consistently used in the context of large epidemiological studies. Although it is reliable in determining asthma symptoms in the past 12 months,35 this approach might introduce an over-reporting of the outcome as parents might label other respiratory symptoms as wheezing. It is reassuring that in the NINFEA cohort most of the cases of wheezing were confirmed by a physician. Moreover, analyses restricted to children who had wheezing treated with inhaled bronchodilators and/or corticosteroids strengthen the results for infant size and weight gain velocity.
Child's weight and the occurrence of wheezing were in part measured concurrently so there is, at least in theory, the possibility of reverse causation. However, the size and weight velocity are estimated over the whole period and it is unlikely that wheezing occurring between 6 and 18 months of age could affect child's growth to the extent that would change its overall trajectory for the first 18 months of life.
Finally, in our cohort, as in many other cohort studies, participants mainly originate from a population with high education and socioeconomic status. However, it has been extensively shown that baseline selection does not imply biased associational estimates in cohort studies.22 ,36 ,37
In conclusion, our findings suggest that both child's size and early weight gain velocity are independently associated with early childhood wheezing. Although from a biological perspective overweight and rapid weight gain are strongly related and may act concurrently in the development of wheezing, these findings might offer new insights into possibly different mechanisms underlying these associations. As overweight and fast weight gain in the first years of life are modifiable risk factors, adequate early interventions could considerably contribute to the reduction of the burden of respiratory diseases in children yielding important long-term health benefits.
Acknowledgments
The authors are grateful to all the participants of the NINFEA cohort.
References
Footnotes
Contributors All authors made substantial contributions to the conception and design of the study, acquisition, analysis and interpretation of data. All authors were involved in drafting the manuscript and revising it critically for important intellectual content and all have approved the version to be published.
Funding The NINFEA study was partially funded by the Compagnia San Paolo Foundation. MP was funded by the Erasmus Mundus for Western Balkans (ERAWEB) programme (reference number: M2.12.012) and the present work was a part of her Master thesis.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The NINFEA study was approved by the Ethical Committee of the San Giovanni Battista Hospital and CTO/CRF/Maria Adelaide Hospital of Turin (approval N.0048362 and following amendments).
Provenance and peer review Not commissioned; externally peer reviewed.