Article Text

Abstract
Introduction There is increasing evidence of an association between Idiopathic Pulmonary Arterial Hypertension (IPAH) and immune dysregulation. Amongst other evidence, autoantibodies are detected in IPAH and there is a high prevalence of autoimmune conditions associated with group 1 pulmonary arterial hypertension.1 Previous work has focussed on a role for T-regulatory cells in IPAH, however, we have noted a more profound general lymphopaenia clinically, which we set out to define and investigate.
Objectives To phenotype circulating leucocytes in patients with IPAH.
Methods Fresh peripheral blood leucocytes from patients with IPAH were compared to age and sex-matched healthy controls. A standardised flow cytometry panel for cell surface markers of leucocyte sub-populations was adapted from the Human Immunology Project.2 Additionally Ig subclasses in serum were analysed by PEG enhanced immunoturbidometric assay and nephelometry. Peripheral lung tissue from explants in patients with IPAH was compared to control tissue from lung tumour resection (distant to the tumour margin). Tissue was immunostained for complement fragments C3d and C4d by streptABC peroxidase technique and visualised with 3,39-DAB hydrochloride and imaged by light microscopy.
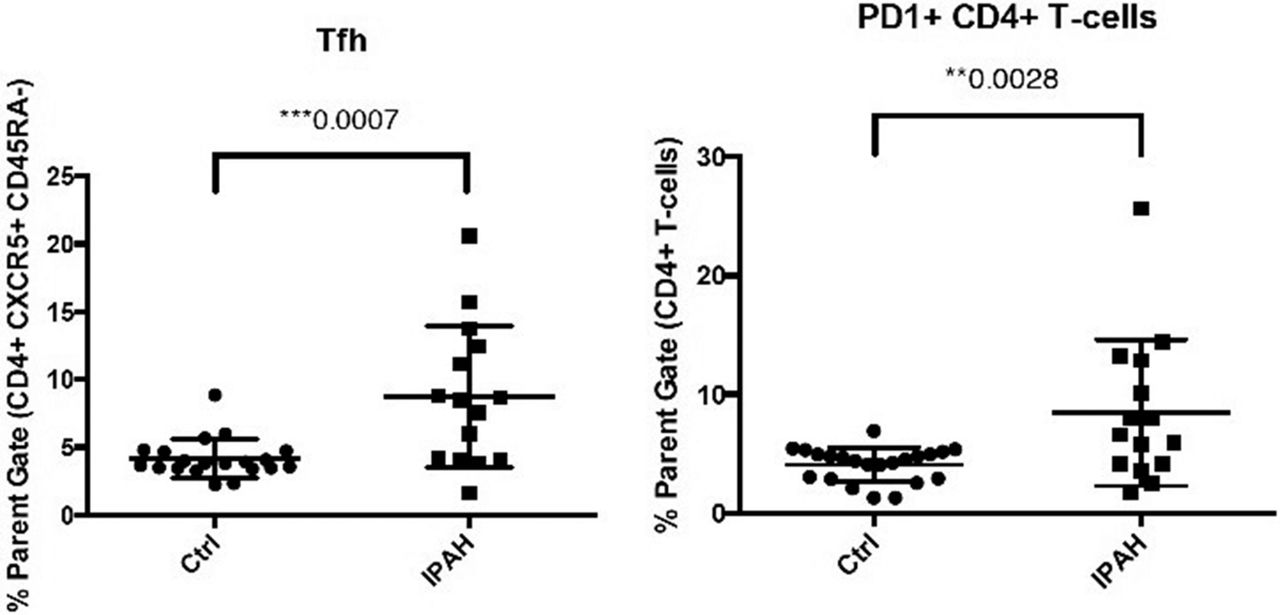
Results Overall lymphocyte counts were significantly reduced in IPAH compared to controls (p = 0.0187). Despite this, IPAH patients demonstrated significantly increased populations of T follicular helper (Tfh) cells (p = 0.0007) and PD1+CD4+ T-cells (p = 0.0028), associated with T-cell exhaustion and control of Tfh mediated humoral immunity. There was evidence of altered B-cell differentiation with increased transitional cells (p = 0.01) and decreased non-switched memory cells (p = 0.001). Ig subclasses were not statistically different between IPAH and control and complement deposition was not significantly different between disease and control in precapillary lung vessels.
Conclusions There is evidence of immune dysfunction in IPAH, notably consistent with previous reports in autoimmunity. Dysregulated immunity is emerging as a potentially important factor in IPAH pathogenesis.

{kind=link}
IPAH patients demonstrated significantly increased populations of T follicular helper (Tfh) cells and PD1+CD4+ T-cells compared to healthy controls
References 1 Mouthon L, Guillevin L, Humbert M. Pulmonary arterial hypertension: an autoimmune disease? Eur. Respir. J. 2005;26(6):986–8
2 Maecker HT, McCoy JP, Nussenblatt R. Standardizing immunophenotyping for the Human Immunology Project. Nat. Rev. Immunol. 2012;12(3):191–200