Article Text

Abstract
Background and objectives Many respiratory patients have deranged physiology and can deteriorate rapidly during acute episodes. Consequently, early decision-making is vital to improve outcomes and to ensure patient’s wishes are respected.
We aim to improve the care of inpatients who acutely deteriorate through clinical leadership, as part of a quality improvement (QI) collaboration, by improving early decision-making and clinical response.
As a pilot project we retrospectively (January 2012–September 2014) analysed all 2222 calls from three respiratory wards (84 beds). Fewer events occurred at the weekend (9.4% per day) compared to weekdays (16.2% per day). More events occurred between0900–1700 (41.1%) compared to out of hours (58.9%). Decision-making was found to be poor with 12.2% patients having cardiopulmonary resuscitation (CPR) decisions in place.
Methods Following initial data analysis, one ward participated in a QI project to identify areas for improvement and target these through small tests of change. The interventions implemented by the ward team included a staff survey, “deteriorating patient stamp”, post-2222 call debriefing and “safety huddles”. The effectiveness of these interventions was measured through analysis of on-going arrest calls and documentation of decision-making in case-notes.
Results Reduction in number of 2222 calls on pilot ward between pre-intervention and post-intervention time periods (mean 1.44 vs. 0.56) as shown in Figure 1.
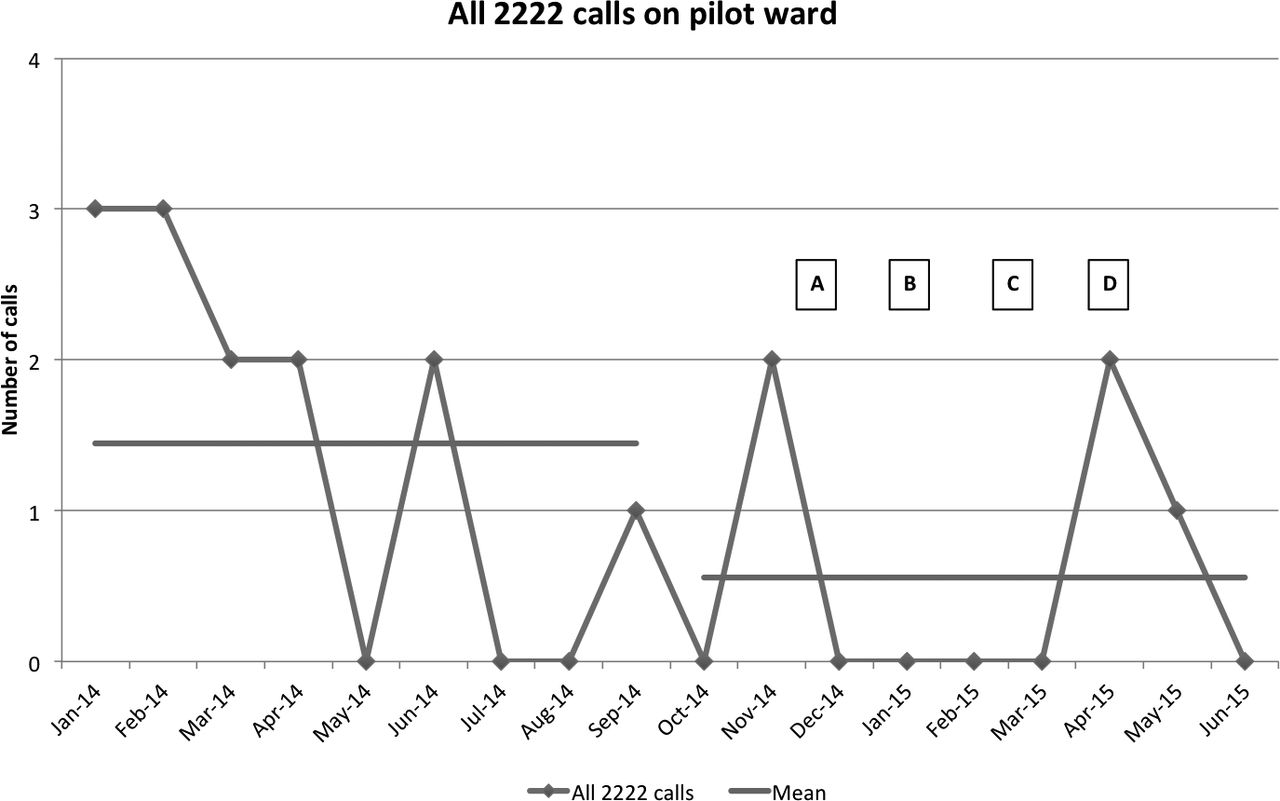
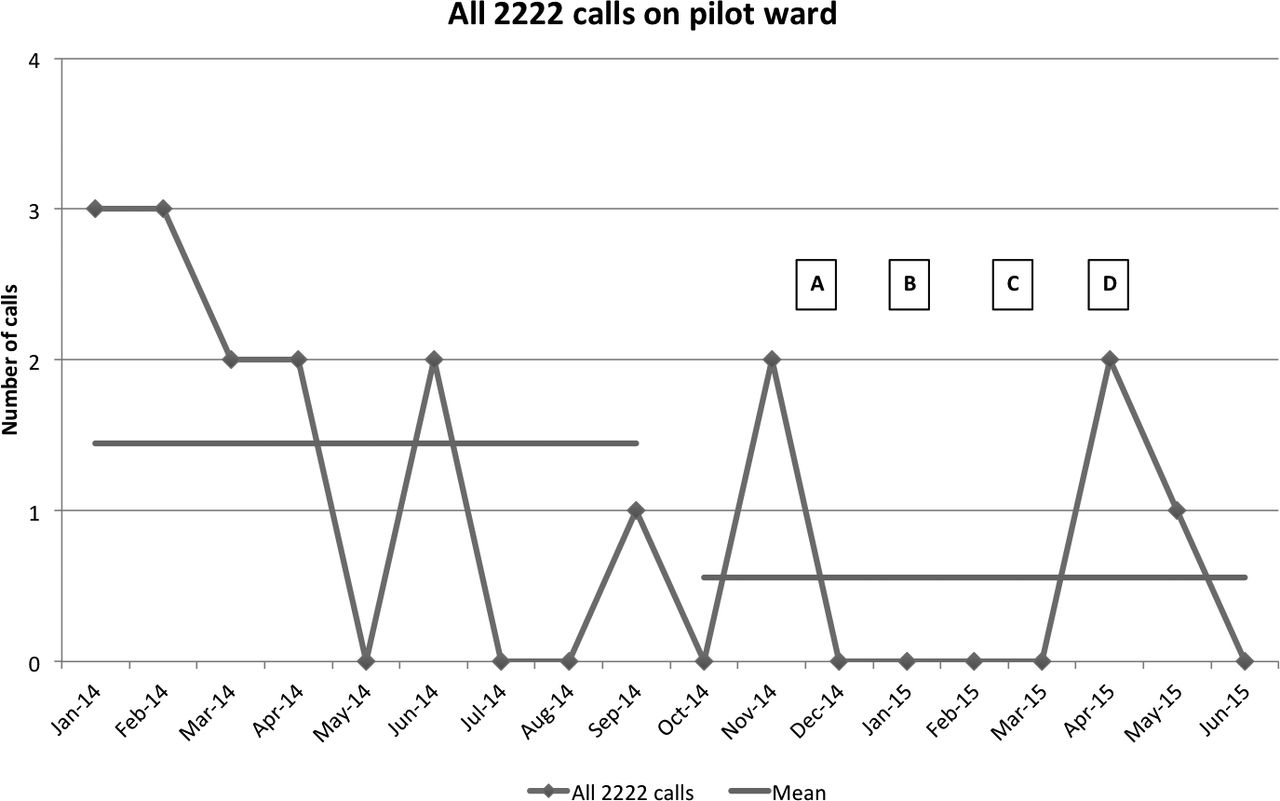{kind=link}
Total number of 2222 calls on pilot ward. Interventions indicated by lettering (A): Staff survey, (B): Introduction of “deteriorating patient stamp”, (C): Debriefing following any arrests, (D): Introduction of “Safety huddle”. Mean of pre-intervention and intervention data, 1.44 and 0.56 respectively
Total 2222 calls per bed reduced for the pilot ward (63.6% reduction) compared to non-pilot wards (9.68% increase) during the pre and post-intervention phases. Similar results were shown for cardiac arrests alone (62.5% reduction compared to 26.7% increase). Decision-making was improved through the intervention phase with 75% of inpatients having DNACPR decisions and 46% escalation plans documented. Safety huddles helped improve ward culture and spread lessons learnt from debriefing of the last 3 events.
Conclusion Early results show there has been a reduction in total 2222 calls in the pilot ward compared to the other wards. We believe this is through improved decision making and empowering frontline staff. This could be scaled-up in other wards to have greater impact on patient care.