Article Text

Statistics from Altmetric.com
We have taken keen interest in the current discussion on the meaning of the lung clearance index (LCI) in patients with primary ciliary dyskinesia (PCD). In patients with cystic fibrosis (CF), LCI from the nitrogen multiple-breath gas washout (N2-MBW) test has become a sensitive marker for detection of ventilation inhomogeneity with a good correlation between LCI and FEV1.1 However, in patients with PCD, two studies failed to find a correlation for the FEV1 and LCI.1 ,2 This difference in functional measures between CF and PCD was recently challenged by Boon et al,3 showing a robust correlation between LCI and FEV1 in patients with PCD. In the carefully written accompanying editorial, several factors were given to explain, among others these, differences between studies.4
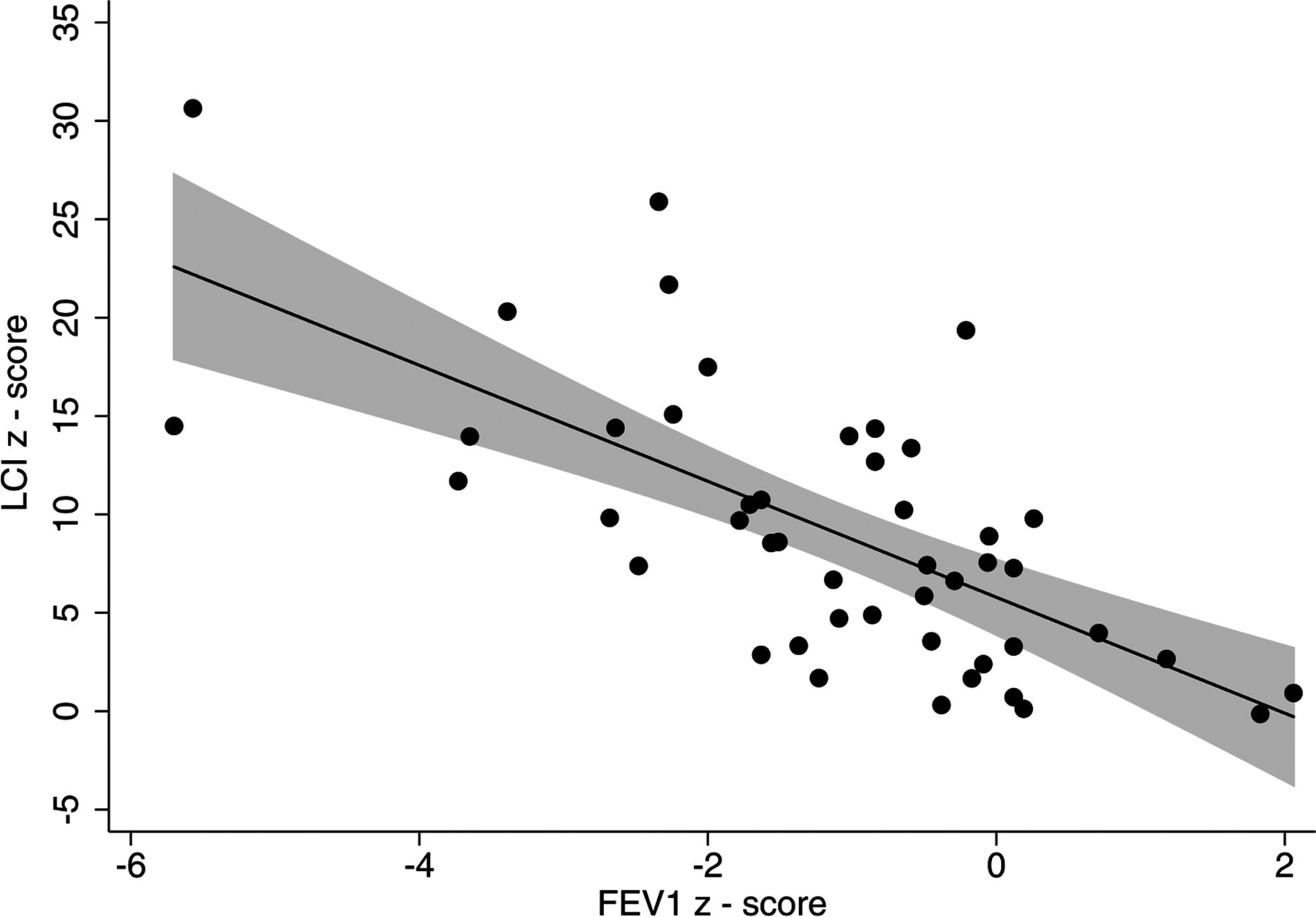
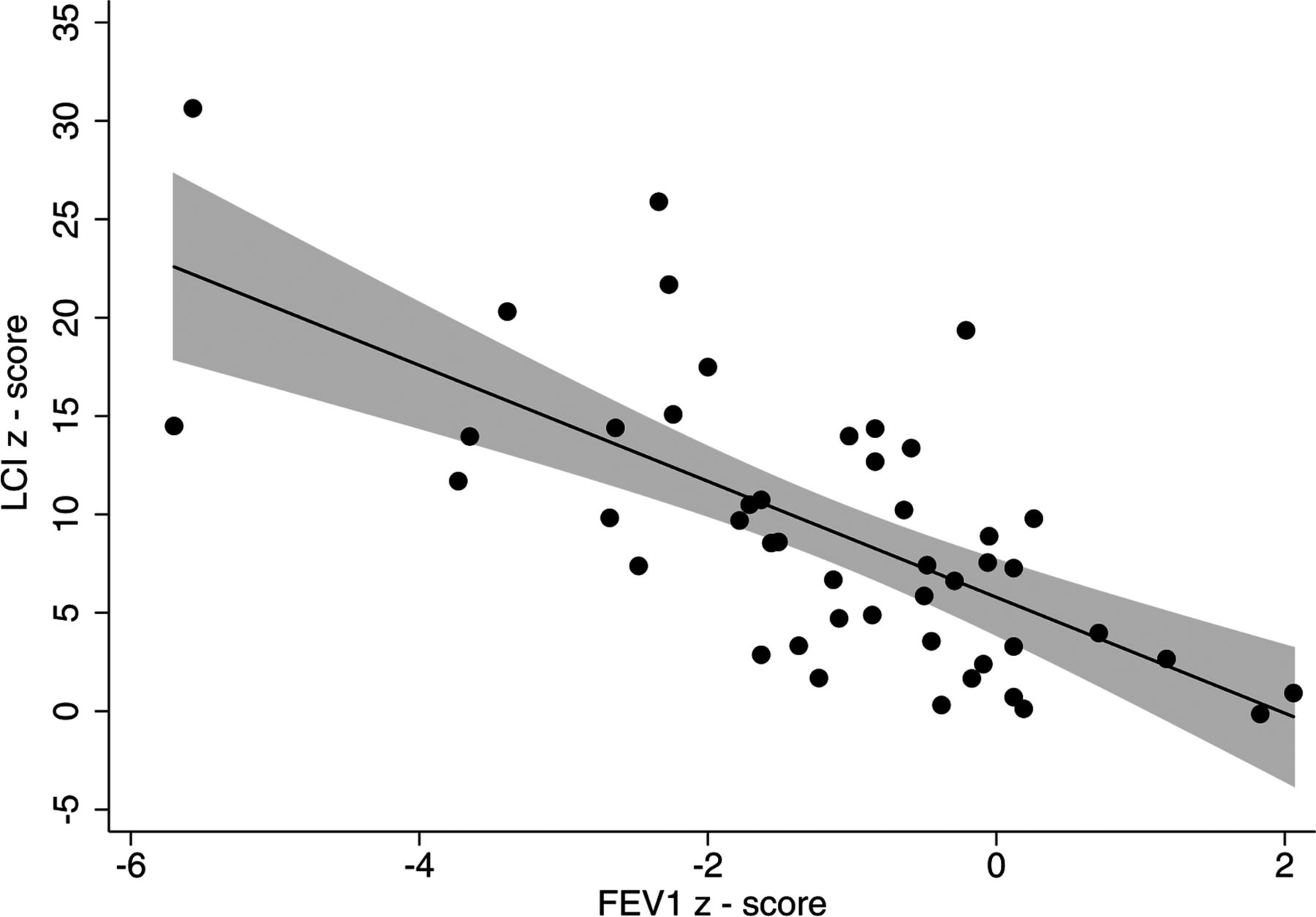
Our aim is now to add further data to this discussion. We performed N2-MBW measurements and spirometry in 47 patients with PCD at a mean (SD; range) age of 14.7 (6.9; 4.0–42.3) years, using an Exhalyzer D (EcoMedics, Duernten, Switzerland) and Jaeger MasterScreen body plethysmograph (CareFusion, Höchberg, Germany) on the same day. z-Scores were defined of a healthy reference population for FEV15 and from an in-house healthy population (n=46) measured with the same equipment for LCI. We found a good correlation between LCI and FEV1 z-scores (coefficient: −2.95, 95% CI −3.92 to −1.97, p<0.001, R2 0.45, r −0.67, see figure 1). Using absolute values adjusted for age, gender and height, the correlation between LCI and FEV1 remained significant in a robust way (coefficient: −3.24, 95% CI −4.51 to −1.97, p<0.001, R2 0.49, r−0.70). In our cohort, the association was independent of age (coefficient: −2.88 for <14 years and −2.70 for >14 years) and disease severity (coefficient: −3.36 for those with FEV1 <−1 z-score and −3.42 for those with FEV1 >−1 z-score). This suggests that it is neither the use of z-scores nor the different age or disease severity that leads to the discrepant findings of previous studies.
{kind=link}
Association of lung clearance index (LCI) with FEV1 in 47 patients with primary ciliary dyskinesia (PCD). LCI z-scores from the nitrogen multiple breath washout (N2-MBW) versus FEV1 z-scores in 47 patients with primary ciliary dyskinesia (PCD). Fitted values denote the black line. The grey background denotes the 95% CI.
Taken together, we confirm results from Boon et al of a good correlation between LCI and FEV1 in patients with PCD. This association was independent of age or disease severity. Besides different pieces of equipment and tracer gases used,4 another reason for discrepancies between studies1 ,3 might still be the different genetic background leading to distinct PCD phenotypes between regions and centres.
Footnotes
Contributors SN, AS, SY, CC, PL and CK-R: Conceived and designed the experiments. SN, AS and SY: Performed the experiments. SN and AS: Analysed the data. SN and CK-R: Wrote the paper. CK-R: Qualified as the guarantor of the paper, took responsibility for the integrity of the work as a whole, from inception to published article.
Funding Fondation Botnar.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Ethics Committee of the Canton of Bern and Ethics Committee of the Ruhr University Bochum.
Provenance and peer review Not commissioned; internally peer reviewed.