Article Text

Abstract
Rationale Asthma exacerbations are commonly precipitated by viral upper respiratory infections (URIs). Vitamin D insufficiency associates with susceptibility to URI in patients with asthma. Trials of vitamin D in adults with asthma with incidence of exacerbation and URI as primary outcome are lacking.
Objective To conduct a randomised controlled trial of vitamin D3 supplementation for the prevention of asthma exacerbation and URI (coprimary outcomes).
Measurements and methods 250 adults with asthma in London, UK were allocated to receive six 2-monthly oral doses of 3 mg vitamin D3 (n=125) or placebo (n=125) over 1 year. Secondary outcomes included asthma control test and St George's Respiratory Questionnaire scores, fractional exhaled nitric oxide and concentrations of inflammatory markers in induced sputum. Subgroup analyses were performed to determine whether effects of supplementation were modified by baseline vitamin D status or genotype for 34 single nucleotide polymorphisms in 11 vitamin D pathway genes.
Main results 206/250 participants (82%) were vitamin D insufficient at baseline. Vitamin D3 did not influence time to first severe exacerbation (adjusted HR 1.02, 95% CI 0.69 to 1.53, p=0.91) or first URI (adjusted HR 0.87, 95% CI 0.64 to 1.16, p=0.34). No clinically important effect of vitamin D3 was seen on any of the secondary outcomes listed above. The influence of vitamin D3 on coprimary outcomes was not modified by baseline vitamin D status or genotype.
Conclusions Bolus-dose vitamin D3 supplementation did not influence time to exacerbation or URI in a population of adults with asthma with a high prevalence of baseline vitamin D insufficiency.
Trial registration number NCT00978315 (ClinicalTrials.gov).
- Asthma
- Respiratory Infection
- Viral infection
Statistics from Altmetric.com
Key messages
What is the key question?
Does vitamin D3 supplementation prevent asthma exacerbation or upper respiratory infection (URI) in adults with inhaled corticosteroid-treated asthma?
What is the bottom line?
In patients with a high prevalence of vitamin D insufficiency at baseline, vitamin D3 supplementation did not influence time to exacerbation or URI or concentrations of inflammatory markers in induced sputum; effects of the intervention were not modified by baseline vitamin D status or by polymorphisms in the vitamin D pathway.
Why read on?
This is the first clinical trial in adults to investigate the effects of vitamin D3 supplementation on incidence of asthma exacerbation and URI as primary outcomes.
Introduction
Acute exacerbations are the major cause of morbidity and mortality in patients with asthma. Viral upper respiratory infections (URIs) are major precipitants, but interventions to prevent these are lacking.1 Numerous observational studies have reported associations between inadequate vitamin D status (serum 25-hydroxyvitamin D (25(OH)D) concentration <75 nmol/L) and susceptibility to URI2: these are particularly strong in patients with asthma.3 In vitro, vitamin D metabolites favourably modulate the immune response to respiratory viruses4 and enhance responsiveness to corticosteroids for production of the anti-inflammatory cytokine interleukin-10.5 Two small trials of vitamin D supplementation in children with asthma treated with inhaled corticosteroids (ICS) have reported reduced rates of exacerbation among participants randomised to the intervention arm.6 ,7
Recently, a trial of vitamin D supplementation conducted in adults reported a trend towards protection against asthma exacerbation in the intervention arm as a secondary outcome (adjusted HR 0.63, 95% CI 0.39 to 1.01).8 Trials of vitamin D in adults with asthma with incidence of exacerbation and URI as primary outcome are still lacking however. Moreover, no studies have been conducted to determine the influence of vitamin D on FENO or concentrations of inflammatory mediators in induced sputum, or to investigate whether genetic factors influence responses to vitamin D supplementation in asthma, as suggested by an observational study.9 We therefore conducted a double-blind randomised placebo-controlled trial of vitamin D3 supplementation in adults with ICS-treated asthma to test the hypothesis that this intervention reduces incidence of URI and severe exacerbations in this population, including measures of lower airway inflammation as secondary outcomes. Prespecified subgroup analyses were performed to investigate whether 34 single nucleotide polymorphisms in 11 vitamin D pathway genes modified the effects of vitamin D supplementation on clinical outcomes. In the absence of a consensus on 25(OH)D thresholds required for protection against disease, we deliberately enrolled patients with a broad range of baseline 25(OH)D values so that prespecified interaction analyses could be conducted to determine whether the effects of supplementation varied according to baseline vitamin D status. A bolus dosing regimen was used to achieve rapid correction of vitamin D deficiency among participants in the intervention arm, and to allow supervised administration of trial medication to maximise adherence.
Methods
Participants
Adult patients with a medical record diagnosis of asthma treated with ICS were identified by searching databases at 60 general practices and at asthma clinics in two Acute National Health Service Trusts in London, UK, and invited for screening. Principal exclusion criteria were age <16 years or >80 years; tobacco smoking history >15 pack-years; medical record diagnosis of COPD; and failure to exhibit significant variability/reversibility in airway obstruction. Written informed consent was obtained from all participants before enrolment.
Procedures
Participants attending screening visits completed the St George's Respiratory Questionnaire (SGRQ),10 the EuroQoL-5D questionnaire11 and the Asthma Control Test (ACT)12 and underwent a baseline clinical assessment incorporating spirometry, measurement of FENO and collection of a blood sample. A subset of 50 participants was invited to undergo sputum induction with hypertonic saline. Participants fulfilling eligibility criteria entered a run-in period of at least 2 weeks, during which they were asked to complete a symptom diary on a daily basis (see online figure E1). Eligible patients were randomly assigned to receive six 2-monthly oral doses of 6 mL Vigantol oil (Merck Serono, Darmstadt, Germany) containing 3 mg (120 000 IU) vitamin D3, or 6 mL organoleptically identical placebo (Miglyol oil, Caesar and Loretz, Hilden, Germany) with allocation ratio 1:1. Randomisation was assigned by permuted blocks of 10 and stratified according to (A) British Thoracic Society treatment step (2–3 vs 4–5) and (B) inclusion in versus exclusion from the induced sputum substudy.
Participants completed study diaries daily for 12 months. Five further doses of study medication were administered at 2-monthly intervals following the first dose. Face-to-face follow-up visits were performed at 2 months, 6 months and 12 months of follow-up.
Coprimary end points for the trial were time to first severe asthma exacerbation and time to first URI. Severe asthma exacerbation was defined as deterioration in asthma resulting in (A) treatment with oral corticosteroids, or (B) hospital admission or emergency department treatment, or (C) decrease in the morning peak expiratory flow rate (PEFR) to more than 25% below the mean run-in value on two or more consecutive days.13 URI was defined as influenza-like illness14 or as a cold with symptom scores meeting modified Jackson criteria.15
Secondary end points were peak values and areas under the curve for symptom scores during severe exacerbation/URI; proportion of days with poor asthma control; proportion of nights with awakenings due to asthma symptoms; time to unscheduled healthcare attendance and use of antibiotics for exacerbation/URI; ACT and SGRQ scores, FENO concentration, daily ICS doses, % predicted FEV1, PEFR, use of inhaled relief medication and induced sputum differential cell count and supernatant inflammatory profiles at 2 months, 6 months and 12 months; trough serum concentrations of 25(OH)D and parathyroid hormone (PTH) at 2 months and 12 months; and health economic outcomes (costs of exacerbations and URI, quality-adjusted life years and incremental net benefit over 1 year).
Sample size and statistical analysis
Assuming a median time to event of 120 days16 we calculated that 200 participants (100 in each group) would need to be randomised in order to detect a 60 day difference in median time to event between intervention and control groups with 80% power using a two-sided test at the 5% significance level.17 A total of 250 participants were recruited in order to allow for 20% loss to follow-up.
Analysis was by intention-to-treat: all participants who took at least one dose of study medication were included in efficacy and safety analyses. Significance was tested at the 5% level. Time-to-event outcomes were analysed using Cox regression adjusted for stratification factors. Subgroup analyses were conducted to determine whether the effect of vitamin D3 supplementation on coprimary outcomes was modified by baseline vitamin D status (using serum 25(OH)D thresholds of 50 nmol/L and 75 nmol/L) or genotype.
Further details of Methods are presented in online supplementary information.
Results
Five hundred and ninety adults with a medical record diagnosis of asthma were invited to participate in the trial. Of these, 297 attended a screening visit and were assessed for eligibility between 27 August 2009 and 25 June 2012: 37 were ineligible to participate and 10 were eligible but declined randomisation. The remaining 250 participants were randomised to intervention versus control arms of the trial in equal numbers: all received at least one dose of study medication, and were included in the intention-to-treat analysis (figure 1). Clinical and demographic characteristics of randomised participants were comparable for intervention versus control groups (table 1). The majority (206/250, 82%) had inadequate vitamin D status (serum 25(OH)D<75 nmol/L) at baseline, and participants had a high rate of events requiring oral corticosteroids and/or an increase in ICS dose in the year preceding enrolment (median 2.0 episodes, IQR 1.0 to 3.0). The trial ended on the date of the final study visit of the final participant undergoing follow-up.
Baseline characteristics by allocation

Trial profile.
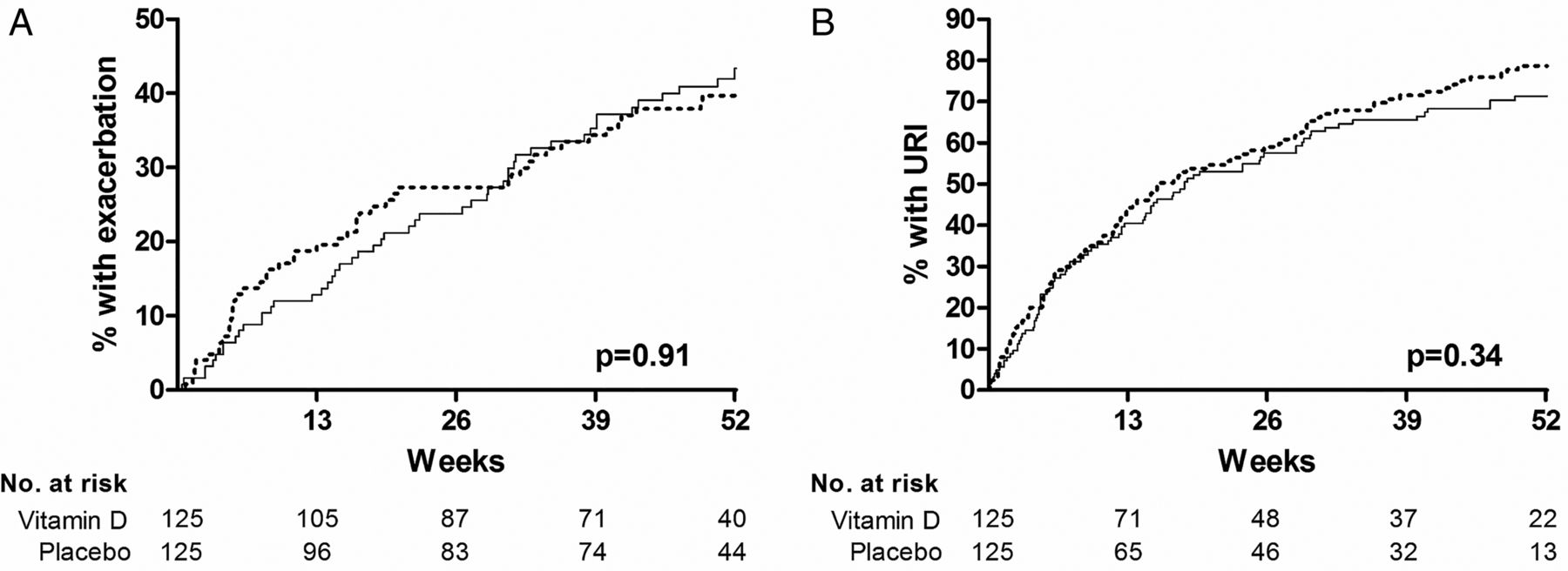
Allocation to vitamin D3 versus placebo did not influence time to first severe asthma exacerbation (adjusted HR 1.02, 95% CI 0.69 to 1.53, p=0.91) or time to first URI (adjusted HR 0.87, 95% CI 0.64 to 1.16, p=0.34; figure 2, table 2). Neither did it influence the annual rate of severe exacerbations or URI; the proportion of participants experiencing either outcome; or the peak severity or symptom score area under the curve for either event (table 2, see online figure E2, supplementary information). No effect of the intervention was seen on ACT scores, other measures of asthma symptom control, FEV1, PEFR or FENO (table 2). Allocation to the intervention arm of the trial resulted in a significant increase in serum 25(OH)D concentration (mean 23.0 nmol/L increase at 12 months, p<0.001, table 2). This was associated with suppressed serum PTH concentration (mean 0.89 pmol/L decrease at 12 months, p=0.02), but not with a difference in serum corrected calcium concentration (see online table E5, supplementary information).
Outcomes by allocation
{kind=link}
{kind=link}
Coprimary outcomes by allocation. Time to first severe asthma exacerbation (A) and first upper respiratory infection (URI, B) by allocation. Numbers of participants yet to experience each outcome (number at risk) at 0 weeks, 13 weeks, 26 weeks, 39 weeks and 52 weeks are shown. Solid line, vitamin D3; dotted line, placebo.
Administration of vitamin D3 modestly improved respiratory quality of life as evidenced by adjusted interarm differences in total SGRQ score of −3.9 points at 2 months (p=0.005), −3.7 points at 6 months (p=0.038) and −3.3 points at 12 months (p=0.060; p for allocation-time interaction=0.026; table 2, see online figure E3, supplementary information). These reductions were associated with statistically significant decreases in component scores for the impacts dimension of the SGRQ at 2 months (p=0.05) and 6 months (p=0.005; p for allocation-time interaction=0.030, see online table E2, figure E3, supplementary information). No differences in EQ5D scores were observed between arms (see online table E3, supplementary information). Allocation to vitamin D3 versus placebo did not influence differential white cell counts or inflammatory profile in induced sputum (see online table E4, supplementary information).
Day-to-day values for PEFR, asthma symptom score, short-acting bronchodilator use or the percentage of participants woken at night or experiencing poor asthma control days did not fluctuate in relation to the timing of administration of intermittent bolus doses of study medication (see online figure E4, supplementary information). Allocation to vitamin D3 versus placebo did not influence use of asthma medications or antimicrobials (see online table E6, supplementary information) or health service uptake (see online table E7, supplementary information). Neither did it influence work absence due to asthma symptoms or respiratory infections (see online table E8, supplementary information) or health economic outcomes (see online table E9, supplementary information). The cost-effectiveness acceptability curve displayed in online figure E5, supplementary information, shows that the probability that vitamin D3 versus placebo is cost-effective is around 70% at a realistic willingness to pay (£20 000) for a quality-adjusted life year gain. Prespecified subgroup analyses revealed no evidence of effect modification on coprimary outcomes according to baseline vitamin D status (see online table E10, supplementary information). After correction for multiple analyses, none of the single nucleotide polymorphism investigated were found to modify the effect of supplementation on risk of severe exacerbation or URI (see online table E11, supplementary information).
Twenty-three serious adverse events were reported in 20/250 participants receiving at least one dose of study medication; one participant died during the study, following a road traffic accident (see online table E12, supplementary information). No serious adverse event was attributed to study medication. A total of 1283 non-serious adverse events were reported in 240/250 participants: these were equally distributed between study arms (see online table E13, supplementary information). No hypercalcaemia was seen.
Discussion
We report findings of the first trial of bolus dose vitamin D supplementation for the prevention of exacerbation and URI in adult patients with asthma. No effect of the intervention was seen on either coprimary outcome, despite a high prevalence of vitamin D insufficiency at baseline. Of 16 secondary outcomes investigated, only one—respiratory quality of life, as measured by the SGRQ—showed a statistically significant difference between arms, but this was just less than the 4-point minimum clinically important difference for this instrument.18 Prespecified subgroup analyses demonstrated no statistically significant evidence of effect modification by clinical or genetic characteristics after correction for multiple analyses.
The results of our trial support and extend the findings of the VIDA trial, recently reported by Castro et al.8 These investigators studied a population of patients with asthma with baseline 25(OH)D <75 nmol/L and reported no effect of vitamin D supplementation on a primary outcome of treatment failure. Subgroup analysis restricted to the 82% of vitamin D3 supplementation in adults with asthma trial participants with baseline 25(OH)D <75 nmol/L revealed no effect of the intervention on either of our coprimary outcomes. Our trial may therefore be regarded as confirming the findings of the VIDA study.
Although primary outcomes for our trial were null, we did observe a modest but statistically significant improvement in respiratory quality of life among participants in the intervention arm, as measured by the total SGRQ score; this was associated with decreases in the impacts scores component of the SGRQ. One of the correlates of the impacts component of the SGRQ is exercise performance, and the favourable effects of vitamin D supplementation on muscle function in deficient subjects are well documented:19 it may be, therefore, that positive effects of vitamin D3 supplementation on participants’ quality of life were mediated by enhancing muscle function; they were not mediated via improved control of asthma symptoms, as the intervention did not influence days in which asthma was poorly controlled, nights with awakenings or ACT scores. However, the possibility of a positive finding arising from type 1 error cannot be ruled out, given the large number of prespecified secondary outcomes in this study. This finding should therefore be regarded as exploratory.
Our trial has several strengths. Inadequate vitamin D status was highly prevalent among the study population at baseline, and participants had significant potential for improvement in asthma control at enrolment as evidenced by high FENO at baseline. We gave a generous dose of vitamin D3, equivalent to 2000 IU (50 μg) per day—more than three times the recommended dietary allowance for adults proposed by the US Institute of Medicine.20 The intermittent bolus dosing regimen we employed allowed us to achieve a high degree of compliance with the intervention (3/6 doses were directly observed and 3/6 were supervised telephonically), while the use of daily symptom diaries allowed us to characterise participants’ symptoms in fine detail. Our trial complements the VIDA trial8 by providing new data on efficacy of a bolus dosing regimen administered for a year to patients with a wide range of baseline serum 25(OH)D concentrations on additional outcomes including incidence of URI, other measures of airway inflammation (exhaled nitric oxide and induced sputum supernatant inflammatory profiles), potential genetic effect modifiers and health economic outcomes.
Our trial also has some limitations. Patients with URI symptoms were not sampled for detection of pathogens; we have previously validated the symptomatic definition of URI employed in this study against PCR in another trial however.21 A minority (32%) of asthma exacerbations in our trial were associated with URI—a somewhat lower proportion than the 44% reported elsewhere.22 Our trial was conducted in an urban setting, and participants had a relatively high prevalence of allergic rhinitis and eczema at baseline. Allergens and particulates may therefore have precipitated a significant number of exacerbations in our study population: if vitamin D only prevents exacerbation precipitated by URI, then this phenomenon could have contributed to our negative findings. Although 77% of participants in our trial experienced a URI, only 44% experienced a severe exacerbation; our study may therefore have lacked power to detect small or moderate effects of the intervention on exacerbation risk.
Another potential limitation relates to the intermittent bolus dosing regimen that we employed. Although this was reasonably effective in correcting vitamin D deficiency (80% of participants in the intervention arm had 25(OH)D levels ≥50 nmol/L at 12 months, as compared with 39% of those in the placebo arm, p<0.001), the interarm difference in serum 25(OH)D concentrations at 12 months was modest (22 nmol/L). It should be noted, however, that serum 25(OH)D concentrations at this time point represent ‘trough levels’: pharmacokinetic studies of the 25(OH)D response to bolus-dose vitamin D supplementation indicate that concentrations peak at 1 week post dose and remain high for several weeks thereafter;23 the difference in vitamin D status between arms in our trial will therefore have been significantly higher than 22 nmol/L for much of the interdosing period. This is reflected in the fact that serum PTH concentrations were significantly lower in the intervention versus the control arm of the trial at 1 year.
While intermittent bolus-dosing with vitamin D can prevent bone fractures,24 some have proposed that it may be less effective than daily dosing for inducing non-classical actions of vitamin D.25 ,26 However, we27 ,28 and others29 have previously shown favourable effects of bolus-dose vitamin D supplementation on outcomes relating to respiratory infection. Nevertheless, we cannot exclude the possibility that results of the vitamin D3 supplementation in adults with asthma trial might have been different if vitamin D had been administered on a daily basis, and trials comparing the effects of daily versus intermittent dosing are needed to address this issue. Pending the conduct of such studies, pooling of existing trial data for individual patient data meta-analysis has potential to increase power to detect effects of vitamin D supplementation on exacerbation risk, and thereby to advance the field.
Acknowledgments
The authors thank the members of the Data Monitoring Committee, Guy E Thwaites (Chair), Brenda E Jones and Tuan Q Phung. The authors also thank clinical and administrative staff at all General Practices acting as participant identification centres; pharmacy staff at the Royal London Hospital for overseeing dispensing of study medication; and all the patients who participated in the trial.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Contributors ARM had the original idea for the study. ARM, BDM, NCB, DAJ, RW, PMT, CJC, CMH and CJG contributed to study design. ARM, BDM, NCB, DAJ, KK, GF, JG, RKR, AB, ABC, DES, CJC and CJG participated in implementation of the trial. DAJ, CLG, CAM, MH, RW, PMT, MR, TRV and WRM developed and performed laboratory assays. DM validated diary records of health economic outcomes. ARM, RLH and DAJ contributed to clinical data analysis. ZS performed health economic analysis. ARM wrote the first draft of the manuscript; all other authors critically reviewed it and approved the final version.
Funding This is a summary of independent research funded by the National Institute for Health Research (NIHR)'s Programme Grants for Applied Research Programme (ref RP-PG-0407-10398).
Competing interests None.
Ethics approval East London and The City Research Ethics Committee 1 (ref 09/H0703/67).
Provenance and peer review Not commissioned; internally peer reviewed.
Data sharing statement Data from the study will be made publicly available in a data repository on publication of this trial report.
Linked Articles
- Airwaves