Article Text

Abstract
Objective To assess whether daily variations in three parameters recorded by non-invasive ventilation (NIV) software (respiratory rate (RR), percentage of respiratory cycles triggered by the patient (%Trigg) and NIV daily use) predict the risk of exacerbation in patients with chronic obstructive pulmonary disease (COPD) treated by home NIV.
Methods Patients completed the EXACT-Pro questionnaire daily to detect exacerbations. The 25th and 75th percentiles of each 24 h NIV parameter were calculated and updated daily. For a given day, when the value of any parameter was >75th or <25th percentile, the day was marked as ‘abnormal value’ (‘high value’ >75th, ‘low value’ <25th). Stratified conditional logistic regressions estimated the risk of exacerbation when ≥2 days (for RR and %Trigg) or ≥3 days (for NIV use) out of five had an ‘abnormal value’.
Results Sixty-four patients were included. Twenty-one exacerbations were detected and medically confirmed. The risk of exacerbation was increased when RR (OR 5.6, 95% CI 1.4 to 22.4) and %Trigg (OR 4.0, 95% CI 1.1 to 14.5) were considered as ‘high value’ on ≥2 days out of five.
Conclusions This proof-of-concept study shows that daily variations in RR and %Trigg are predictors of an exacerbation.
- COPD Exacerbations
- Non invasive ventilation
Statistics from Altmetric.com
Introduction
Early detection of exacerbations to rapidly implement therapeutic interventions is a major goal in the management of patients with severe chronic obstructive pulmonary disease (COPD).1 Respiratory rate (RR) is a physiological parameter that changes during an episode of exacerbation and may serve as the warning signal of a developing exacerbation.2
Home long-term non-invasive ventilation (NIV) is a modality of treatment for patients with COPD at the end stage of chronic respiratory failure.3 Home ventilators are now equipped with built-in software providing data such as RR, percentage of respiratory cycles triggered by the patient (%Trigg) and daily usage.
Our objective was to assess whether day-to-day variation in these three parameters recorded by the ventilators can predict an imminent exacerbation in patients with COPD treated at home with NIV.
Materials and methods
Patients with COPD treated at home with NIV and oxygen therapy were eligible for this prospective observational study (see online supplement for details).
Assessment of exacerbations
Patients filled in the EXACT-Pro questionnaire every day for a maximum of 6 months. This questionnaire was used to detect exacerbation events.4 Each event detected using the EXACT-Pro score had to be validated by an event committee of two chest physicians.
Analysis of data recorded by ventilators
RR, %Trigg and daily usage (h/day) were analysed as follows: 25th and 75th percentiles of each 24 h parameter recorded by the ventilator were calculated from the fourth day of follow-up onwards and updated daily. For a given day, when the value of a parameter was >75th or <25th percentile, the day was recorded as ‘abnormal value’ (‘high value’ >75th, ‘low value’ <25th).
Stratified (one stratum/patient) conditional logistic regression models were used to estimate the risk of exacerbation when ≥2 days (for RR and %Trigg) or ≥3 days (for NIV daily usage) out of 5 days had ‘abnormal values’.
Results
Sixty-four patients were included, 44 of whom completed the study. EXACT-Pro detected 21 medically confirmed cases of exacerbation (mean (SD) age 72 (6) years, forced expiratory volume in 1 s/forced vital capacity 42 (12)%).
The risk of exacerbation was increased when RR (OR 5.6, 95% CI 1.4 to 22.4, p=0.01; sensitivity 46.2%; specificity 89.7%) and %Trigg (OR 4.0, 95% CI 1.1 to 14.5, p=0.037; sensitivity 53.8%; specificity 76.2%) were ‘high value’ on ≥2 days out of five. The variation in daily usage of NIV (>75th or <25th percentile) tended to be associated with a risk of exacerbation (OR 3.0, 95% CI 0.8 to 11.3, p=0.097). Figure 1 shows, for the 21 exacerbations, the EXACT-Pro score, daily use of NIV, respiratory frequency and triggered cycles in the 14 days preceding and following the onset of the exacerbation (see online supplement for detailed results).
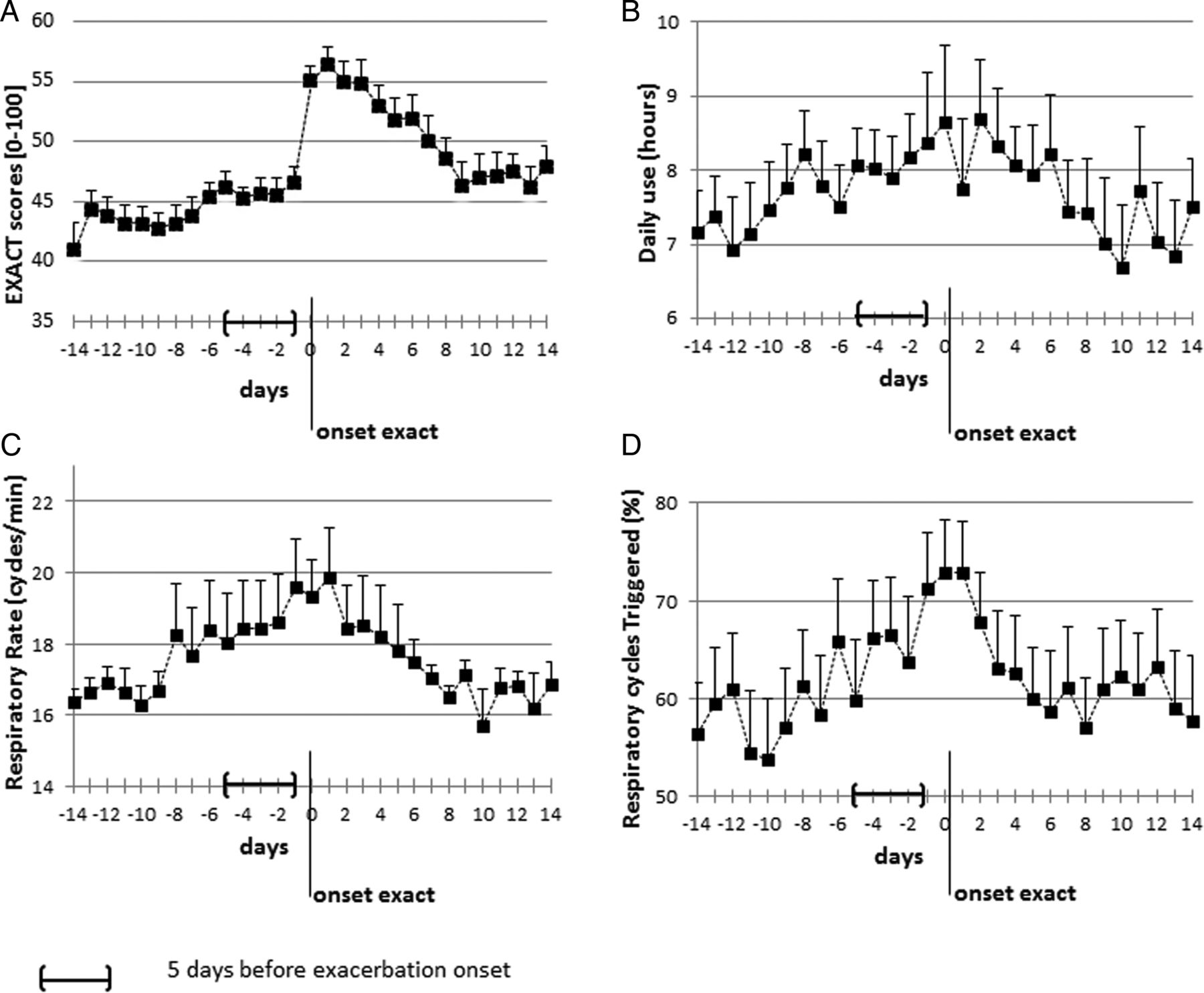
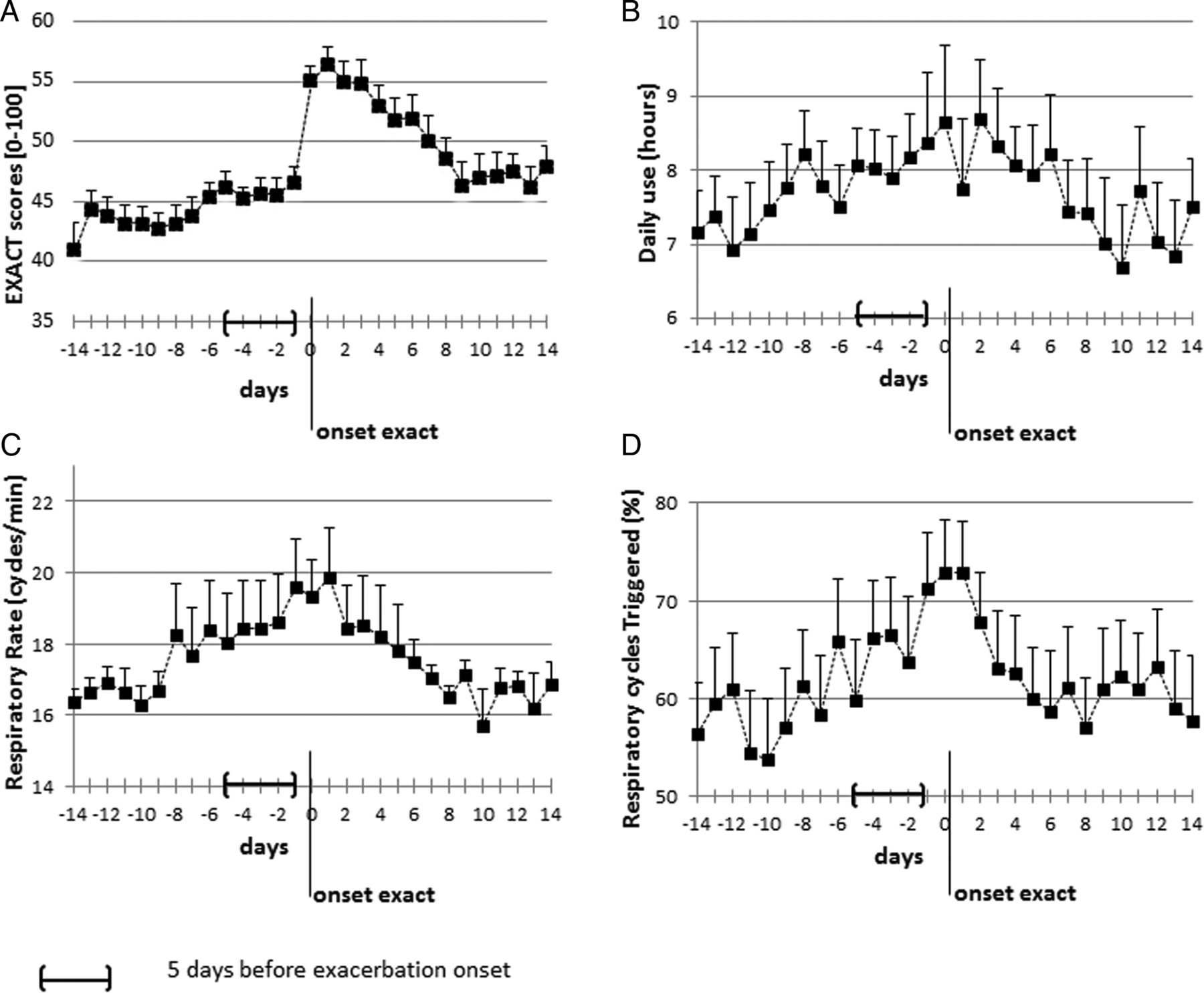{kind=link}
(A) EXACT-Pro score, (B) daily use of non-invasive ventilation, (C) respiratory rate and (D) percentage of respiratory cycles triggered by the patient in the 14 days preceding and following the onset of exacerbation (n=21). Data are reported as mean and SE.
Discussion
Providing useful tools for detecting exacerbations is the cornerstone of COPD management. This study presents the proof of concept that exacerbations of COPD can be detected by the time-course of respiratory parameters recorded by NIV software. RR and %Trigg increased in the days preceding exacerbation onset. Regarding daily NIV usage, some patients increased their usage of NIV, probably with the expectation of reducing breathlessness. Conversely, other patients reduced NIV usage, certainly reflecting intolerance and/or inadequacy of the ventilator settings during exacerbations.
The main advantage of this approach for detecting exacerbations is that it requires neither the patient's active involvement nor additional sensors in the patient's environment. Studies are needed to confirm these results and to investigate their clinical usefulness.
Acknowledgments
We thank Dr Alison Foote (Grenoble Clinical Research Center) for critical reading and language editing.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
J-CB and JP contributed equally.
-
Contributors Involvement in the conception, hypothesis delineation and design of the study: J-CB, J-LP, CP, RT, J-FT. Acquisition of data or analysis and interpretation: J-CB, J-LP, JP, NT, AB, NA. Writing the article or substantial involvement in its revision prior to submission: J-CB, J-LP, JP, NT, RT.
-
Funding Philips-Respironics and Agir à dom (Meylan, France).
-
Competing interests J-CB is employed by Agir à dom, a non-profit home care company, and has received personal fees from Philips (outside the submitted work). NA and NT are employed by Agir à dom. CP has received grants from Agir à dom (outside the submitted work). J-CB, RT, J-LP, NT and NA have a patent pending on the algorithm to detect exacerbations.
-
Patient consent Obtained.
-
Ethics approval This study was approved by our institutional review board (IRB-6705).
-
Provenance and peer review Not commissioned; externally peer reviewed.