Article Text

Abstract
Introduction The impact of obstructive sleep apnoea (OSA) treatment with CPAP on weight is not clear. This meta-analysis was designed to assess whether OSA treatment with CPAP promotes changes in body mass index (BMI) and weight.
Methods We searched PubMed, SCOPUS and Cochrane Central Register electronic databases through 1 October 2013 (including papers in press at that time), without language restrictions. We identified randomised trials of CPAP versus controls with a minimum treatment duration of 4 weeks that objectively measured BMI. Data were independently abstracted and reviewed by two investigators using a standardised protocol.
Results We included a total of 3181 patients from 25 randomised trials that measured BMI and weight. All studies enrolled mainly overweight and obese patients. The fixed-effects meta-analysis revealed that CPAP promoted significant increase on BMI (Hedges’ g=0.14, 95% CI 0.07 to 0.21, I2=16.2%) and weight (Hedges’ g=0.17, 95% CI 0.10 to 0.24, I2=0%). The funnel plot revealed low risk of publication bias. Meta-regression analyses including age, gender, baseline BMI, baseline weight, OSA severity, CPAP compliance, use of sham CPAP, study duration, study design (crossover/parallel), study origin (Western/Eastern), recommendation for dietary changes or physical activity, revealed that no single predictor influenced the main outcome for weight. Baseline weight was a predictor of increased BMI after CPAP.
Conclusions OSA treatment with CPAP promotes significant increase in BMI and weight. Additional therapies for body weight reduction must be recommended for overweight or obese patients with OSA initiated on CPAP.
- Sleep apnoea
Statistics from Altmetric.com
Key messages
What is the key question?
-
Is obstructive sleep apnoea treatment able to promote significant changes in body mass index and weight?
What is the bottom line?
-
CPAP, the standard treatment for more severe forms of obstructive sleep apnoea, promoted significant increase in body mass index and weight.
Why read on?
-
In contrary to some non-randomised studies, the present meta-analysis comprising randomised investigations found that obstructive sleep apnoea treatment promotes weight gain.
Introduction
Obesity is one of the most important risk factors for obstructive sleep apnoea (OSA).1 The vast majority of the patients referred for treatment of OSA are overweight or obese. Data from the Wisconsin Sleep Cohort Study found that a 10% weight gain predicted a corresponding 32% increase in the Apnoea–Hypopnoea Index (AHI) and a sixfold increase in the risk of developing moderate to severe OSA. Conversely, a 10% weight loss predicted a 26% decrease in the AHI.2 Excess body weight has been hypothesised to predispose to OSA in numerous ways, including reduction in upper airway lumen due to fat deposition, reduction of lung volume due to increased abdominal fat and instability of breathing associated with leptin resistance.3
While on the one hand it is clear that excessive weight contributes to OSA, on the other hand, there is emerging evidence that OSA itself feeds back into a complex mechanism that leads to either the development or the contribution to obesity.4 OSA may contribute to weight gain through several potential mechanisms, including changes in neurohormonal mechanisms that control satiety and hunger, changes in dietary habits and decreased physical activity.4 CPAP is the standard treatment for OSA and, therefore, could in theory decrease body mass index (BMI) by mitigating several factors involved in weight gain. Supporting this hypothesis, at least two earlier non-randomised studies5 ,6 have shown that the treatment of OSA with CPAP is associated with a significant reduction in BMI. These results suggested that overweight and obese patients with OSA should expect weight loss when properly treated with CPAP. However, more recent studies were not able to replicate this finding. At least one non-randomised investigation found a strong trend for increasing BMI in the 6-month follow-up of CPAP.7 Another retrospective study found that CPAP was associated with weight gain in some patients. Interestingly, none lost weight.8 One recent substudy data derived from the Apnoea Positive Pressure Long-term Efficacy Study showed that CPAP promoted a modest but statistically significant weight gain in patients with OSA.w19 Given the fact that a considerable number of well-designed randomised studies that evaluated the effects of the treatment of CPAP on a variety of end points also carefully reported BMI, we decided to investigate the impact of CPAP therapy on BMI in patients with OSA using a meta-analysis approach. Based on the fact that the reported effects of CPAP are conflicting and of small magnitude, we hypothesised that the initiation of CPAP will produce no significant effect on BMI.
Methods
This systematic review and meta-analysis was conducted according to the Cochrane Handbook guidelines9 and reported using Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).10
Data sources and searches
We looked for relevant articles in the following databases: PubMed/Medline, SCOPUS and Cochrane Central Register. We browsed for additional data in the references of retrieved articles, and we also contacted experts for non-published data. Two authors independently searched from 1966 to 1 October 2013 (including papers in press at that time) using the following key terms: ‘obstructive sleep apnoea’ AND ‘CPAP’ OR ‘continuous positive airway pressure’ AND ‘randomized clinical trial’ OR ‘randomised clinical trial’ OR ‘sham-controlled’ OR ‘placebo-controlled’ OR ‘controlled-trial’. Consensus was achieved for all data.
Based on our outcomes, we required a minimum treatment duration of 4 weeks to select potential articles for analysis. The computerised search was supplemented with a manual search of the bibliographies of all retrieved articles. Potentially relevant articles were assessed for inclusion against prespecified eligibility and exclusion criteria. Data were independently extracted by two authors (LFD and RJ) and checked for accuracy in a second review.
Study selection
Inclusion criteria were (1) randomised, clinical trials with an active and a control (either sham or no treatment) group, (2) trials that actively measured standard BMI and weight, (3) trials reporting mean and SD (or SE) of BMI and weight before and after intervention (if mean and SD/SE data were not provided but the article was eligible, we contacted the authors) and (4) no language restrictions. We did not include articles that (1) reported duplicated data, (2) used non-randomised designs, (3) compared CPAP with another active lifestyle or drug intervention, (4) covered studies conducted in animals, (5) were reviews, editorials or letters, (6) lasted <1 month (because we considered this timeframe too short for significant weight changes to present) or (7) lacked data that were crucial to our analysis.
Data extraction and quality assessment
For each study, the authors used a structured form to extract the following data:
-
Metadata (first author’s name, publication year, journal)
-
clinical characteristics (age, percentage of men, AHI at baseline, mean and SD for preintervention BMI and weight values)
-
intervention characteristics (duration of the intervention, CPAP compliance, delta BMI and weight (mean and SD))
-
methodology (sample size, parallel or crossover study design, attrition, use of sham CPAP or non-intervention)
-
other data (eg, country of origin, recommendations for physical activity or dietary changes).
All authors were contacted. BMI and weight (plus SDs) were extracted from the main text and tables of each study or sent by email. For crossover studies, we used only data prior to the crossover to avoid carryover bias. When a study reported BMI and weight values for more than one time point, we used the last available time point. If a particular patient population was reported in more than one article, we selected the article that provided the most complete dataset. Finally, if one study reported two data sets (eg, an independent analysis in men and women), then it was considered as two studies.
The methodological quality of the included trials was evaluated by using the Delphi list developed by Verhagen et al,11 as previously described. Two reviewers (LFD and RJ) independently assessed the methodological quality of all studies included in the meta-analysis.
Data synthesis and analysis
Analyses were performed using Stata V.12 (StataCorp, College Station, Texas, USA) for Mac OS X. First, we calculated the mean change and SD for each group from each study (endpoint scores), using the formulas provided by the Cochrane handbook.9 With these data in hand, we determined a standardised effect size for each study. Here, we used the Hedges’ g effect size, which is more adequate than Cohen's d for studies that have small sample sizes. Values of 0.2, 0.5 and 0.8 are considered small, medium and large effect sizes, respectively.12 Next, we measured the pooled weighted effect size (weighted by the inverse variance of each study) using the random effects model. Heterogeneity was evaluated using the χ2 test. We reported outcomes for the fixed-effects model.
Meta-regression was performed for BMI and weight separately using appropriate statistics13 for age (years), gender (percentage of men), baseline BMI, baseline weight, OSA severity, CPAP compliance (number of hours per night), use of sham CPAP (yes/no), study duration (months), study design (crossover/parallel), study origin (Western/Eastern; see online supplementary file) and single recommendation at the study entry for dietary changes (yes/no) as well as physical activity (yes/no). We meta-regressed only one variable at a time.
Results
Overview
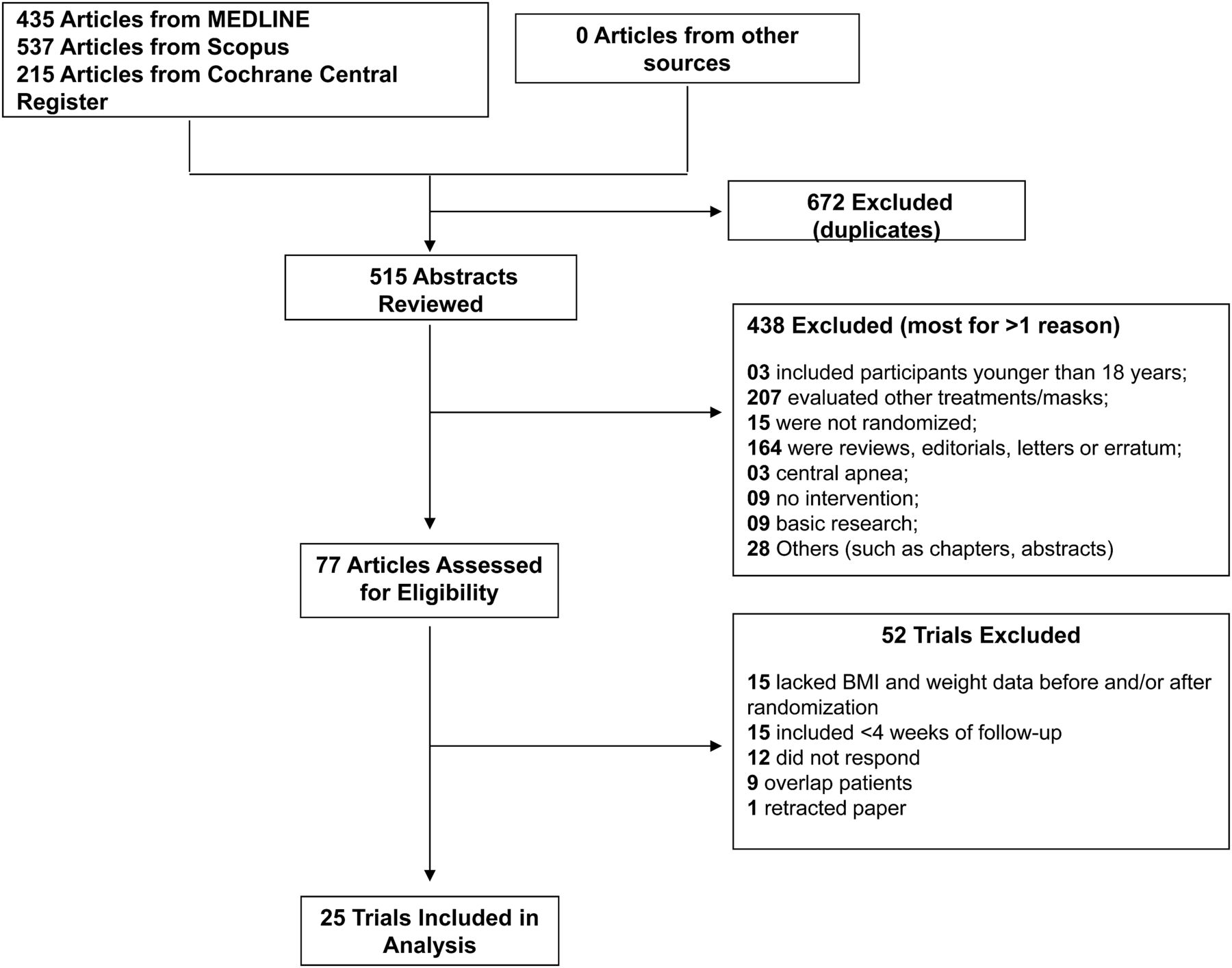
Figure 1 depicts the PRISMA flow diagram and the details used to identify studies in our meta-analysis. Quality assessment revealed that the risk of selection bias was low because most studies described the eligibility criteria of the sample. All studies assessed weight and height by performing measurements on site. Trials were of good quality, with a mean Delphi score of 7 (range 5–8).
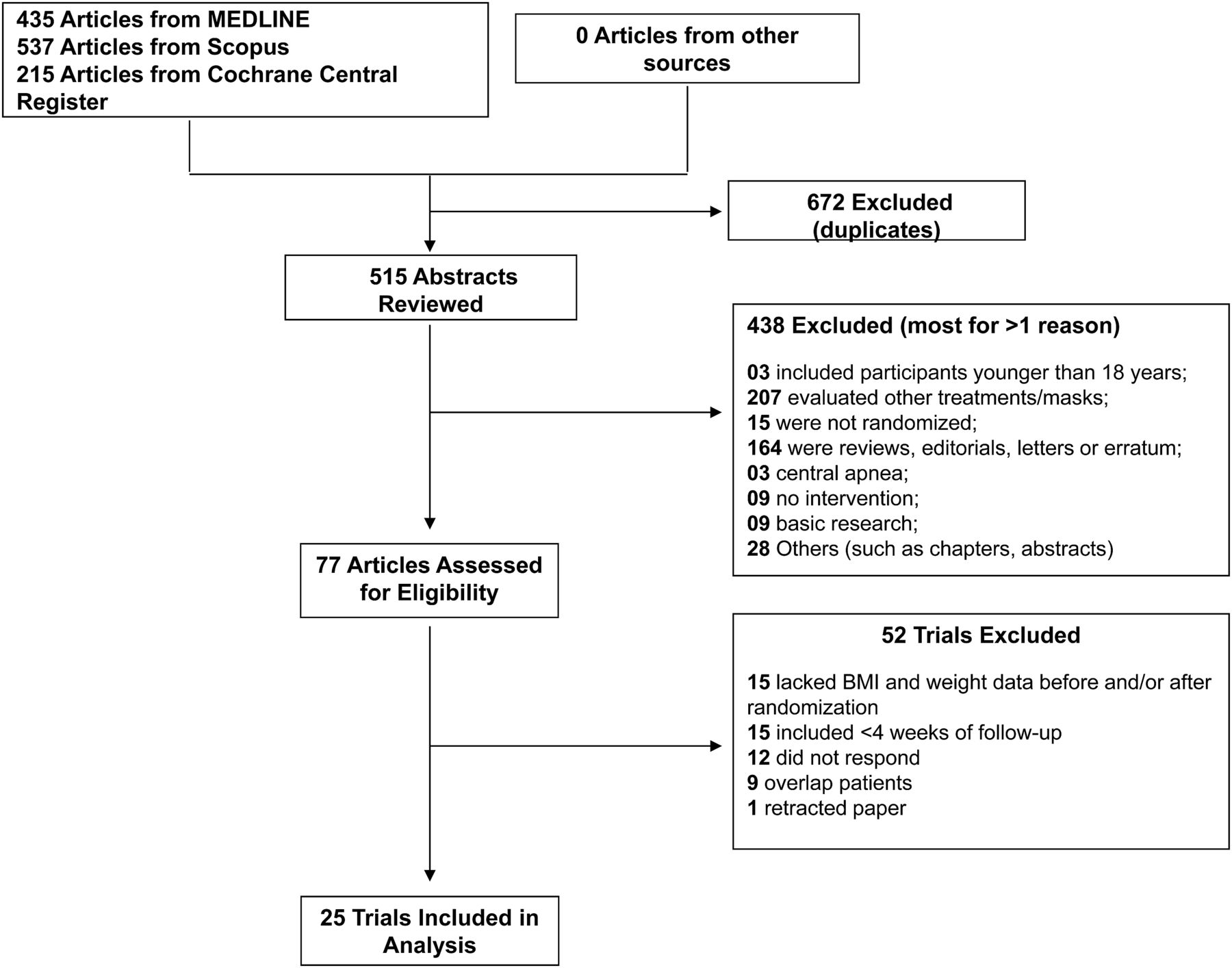
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram of the literature search. BMI, body mass index.
Main analysis
The 25 articlesw1–w25 (due to reference limits, all selected articles were prefixed with ‘w’ and included in the online supplement) enrolled 3181 subjects for BMI analysis. Overall, 83.9% of the study participants were men. The mean age was 52.5 years; SD 5.1 years) and the mean baseline BMI were 31.3 (SD 3.0) kg/m2 for control group and 31.2 (SD 2.9) kg/m2 for CPAP group. All selected studies enrolled mainly overweight and obese patients with OSA. Median study duration was three (range 1–48) months. Information from each study is summarised in table 1.
Study designs and characteristics of participants in 29 randomised trials of CPAP
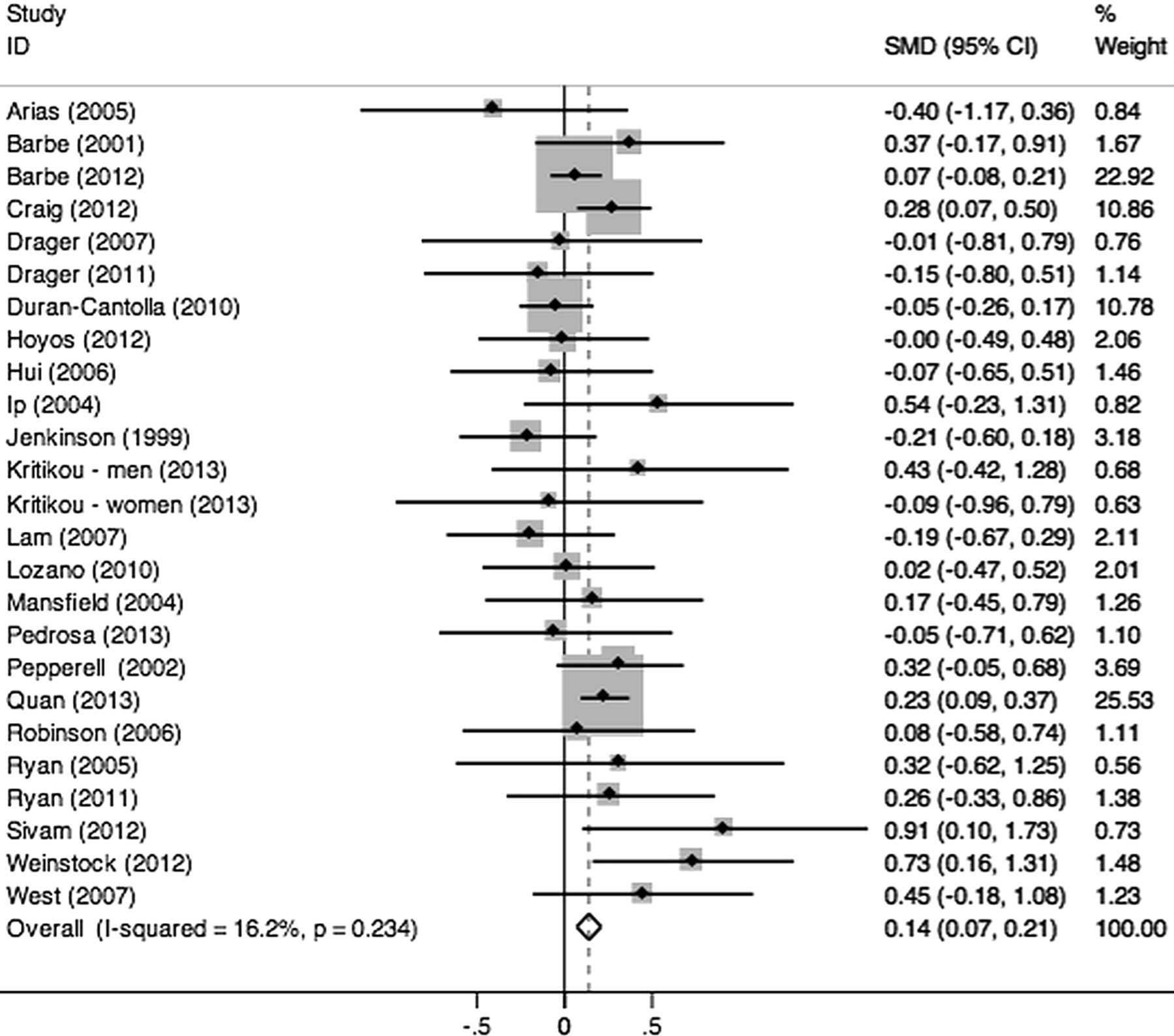
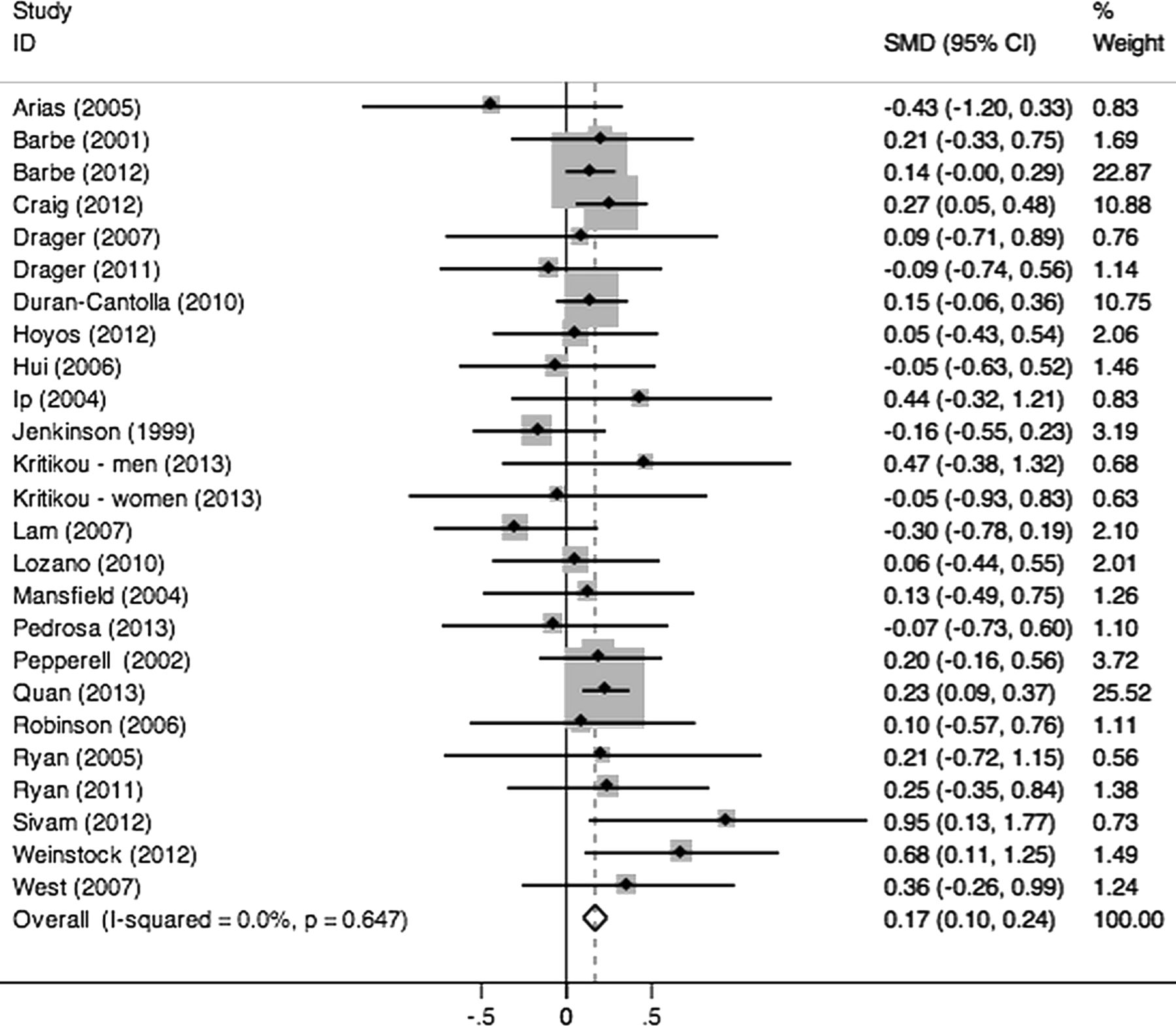
The delta BMI (BMI postintervention minus preintervention) was −0.018±0.243 kg/m2 for control conditions and 0.134±0.273 kg/m2 for CPAP. The delta weight (weight postintervention minus preintervention) was −0.096±0.718 kg for control conditions and 0.417±0.718 kg for CPAP. The fixed-effects meta-analysis revealed that CPAP promoted significant increase on BMI (Hedges’ g=0.14, 95% CI 0.07 to 0.21, I2=16.2%, p=0.234; figure 2) and weight (Hedges’ g=0.17, 95% CI 0.10 to 0.24, I2=0%, p=0.647; figure 3). Begg’s test was not significant for BMI (p=0.881) and for weight (p=0.552). The visual inspection of the funnel plot reveals that the vast majority of the studies were symmetrically distributed, indicating a low risk of publication bias (figure 4). Moreover, the sensitivity analysis that excludes one study at a time showed that the results were not driven by any particular study. Meta-regression analyses using the variables described in the Methods section revealed that baseline weight influenced the BMI outcome (table 2). No predictor influenced the weight outcome (table 3).
Meta-regression analyses for BMI
Meta-regression analyses for weight

Forest plot for body mass index. Fixed-effects model. The effect size statistic is Hedges’ g. Values below and above 0 represent lower and higher body mass index scores, respectively, for the active versus control group. I2=16.2% (p=0.234), suggesting that the meta-analysis did not present significant between-study heterogeneity. SMD, standard mean difference.

Forest plot for weight. Fixed-effects model. The effect size statistic is Hedges’ g. Values below and above 0 represent lower and higher weight scores, respectively, for the active versus control group. I2=0% (p=0.647), suggesting that the meta-analysis did not present significant between-study heterogeneity. SMD, standard mean difference.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Funnel plot, a graph that compares the standardised mean difference (SMD) (x axis) against its SE (y axis). The vast majority of the studies are within the pseudo 95% CI limit of the funnel plot, suggesting that the meta-analysis has low risk of publication bias.
Discussion
To our knowledge, this is the first meta-analysis addressing the impact of OSA treatment with CPAP on BMI and weight. We found that OSA treatment with CPAP promoted significant increase on BMI and weight. The BMI results were influenced by baseline weight. The increasing weight after OSA treatment were not influenced by age, gender, baseline BMI, baseline weight, OSA severity, differences in study design, duration of follow-up, CPAP compliance as well as presence of diet or physical activity counselling. Therefore, clinicians and patients should emphasise adjunctive therapy for weight loss in overweight and obese patients with OSA that are initiated on CPAP.
The literature is consistent in showing the effectiveness of CPAP in mitigating the respiratory events and sleep-related symptoms associated with OSA. In contrast, the effects of CPAP on BMI and weight are not clear so far. While earlier studies suggested that the initiation of CPAP was associated with weight loss,5 ,6 one recent substudy from a large randomised trial concluded that patients gain weight after CPAP initiation.w19 It must be stressed that the vast majority of the studies were limited by the small sample size and were not specifically designed for evaluating the impact of OSA treatment on BMI and weight. However, BMI and weight are well standardised measurements providing an opportunity for a reliable meta-analysis. Our study included a large sample of patients reported from well-designed randomised trials. The main result clearly indicates that CPAP initiation in patients with OSA promotes a small and significant increase in BMI and weight. The positive effects of CPAP initiation on BMI and weight may be explained by the fact that determinants of weight are complex. Weight balance is determined by the net effect of hormones that control satiety and hunger, caloric intake, energy expenditure and physical activity. While it is clear that obesity is a main risk factor for OSA, there are also evidences that OSA may promote weight gain.14 This observation leads to the hypothesis that the treatment of OSA with CPAP may promote weight loss. One retrospective study showed that in contrast to matched controls, patients recently diagnosed with OSA reported significant recent weight increase (average of 7.4 kg).14 The candidate mechanisms to explain a positive feedback between OSA and obesity are multiple. During slow-wave sleep, the anabolic growth hormone is released while the stress hormone cortisol is inhibited.15 Because OSA decreases slow-wave sleep and the treatment of OSA with CPAP restores slow-wave sleep,16 it is conceivable that OSA treatment with CPAP increases the anabolism. OSA may also interfere with leptin, which is a well-studied adipocyte-derived hormone that inhibits appetite. Both obesity17 and OSA18 ,19 have been independently associated with leptin resistance. However, the effect of OSA treatment with CPAP on leptin levels is controversial.5 ,20 ,21 Changes in dietary habits leading to positive energy balance may also contribute to weight gain in patients with OSA. For instance, in the Swedish Obese Subjects Study, patients reporting symptoms suggestive of OSA exhibited a higher energy intake than matched sleep-asymptomatic control subjects of equal weight.22 OSA was associated with an increased preference for calorie-dense foods that are high in fat and carbohydrates in children.23 In addition, low physical activity, which has been reported by some patients with OSA,24 may also contribute to weight gain. However, one randomised study showed that 3 months of CPAP therapy did not modify physical activity in male patients with OSA.25 However, there are also good arguments to hypothesise that the presence of OSA may, in fact, promote weight loss and, therefore by analogy, the treatment of OSA with CPAP could promote weight gain. Intermittent hypoxia, a hallmark of OSA, triggers adipose tissue lipolysis26 and promotes weight loss in mice.27 Patients with OSA struggle to breath during obstructive respiratory events and produce large intrathoracic pressure swings. In addition, sympathetic overactivity is a hallmark of OSA and promotes increases in energy expenditure.28–30 In line with this theoretical framework, one study showed that OSA is associated with increased energy expenditure.31 Therefore, based on the aforementioned factors and the results of this meta-analysis, it is conceivable that factors promoting weight gain counterbalance OSA-related factors promoting weight loss (notably energy expenditure due to recurrent respiratory events during sleep). Reversing OSA with CPAP treatment may result in a small positive effect on BMI and weight.
This present study has some strengths and limitations that should be addressed. Strengths include the use of a prespecified protocol and inclusion of trials published in languages other than English. We assessed methodological quality with the Delphi scale rather than the Cochrane Risk of Bias tool because the Delphi scale has been shown to have acceptable reliability32 and validity,33 ,34 whereas previous studies have reported reliability limitations with the Cochrane tool.35 ,36 Many of the limitations of this meta-analysis are related to the study design of available randomised trials in the literature: (1) although we carefully excluded studies designed to test the effect of weight loss interventions beyond CPAP, the vast majority of studies were not specifically designed to evaluate the effect of CPAP on BMI, (2) virtually no studies performed a detailed analysis of participants’ dietary patterns and physical activity, (3) it is possible that the meta-regression analysis may have no power to detect significant predictors of weight gain after CPAP, (4) finally, most of adult patients were overweight or obese men with moderate to severe OSA. These are typical features of OSA. However, the present results may not be applied to children, women as well as patients with mild forms of OSA and patients who are lean.
In conclusion, treatment of OSA with CPAP promoted significant increase in BMI and weight. It is possible that the magnitude of these increases may not have significant implications at the individual or populational levels. Therefore, when CPAP is initiated to treat overweight and obese patients with OSA, additional therapies for body weight reduction such as lifestyle interventions should be recommended.
Acknowledgments
We would like to thank all authors who provided data for this meta-analysis.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
- Data supplement 2 - Online references
Footnotes
-
Contributors LFD and ARB had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: LFD, GL-F, IJMB and PAL. Acquisition of data: LFD and RJ. Analysis and interpretation of data: LFD, ARB, GL-F, IJMB and PAL. Drafting of the manuscript: LFD, GL-F, IJMB and PAL. Critical revision of the manuscript for important intellectual content: all authors. Statistical analysis: LFD and ARB.
-
Funding Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP). LFD is supported by a Young Investigator Award from FAPESP (2012/02953-2). The funder has no role in the study design, data acquisition, data analysis and interpretation.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.