Article Text

Abstract
Background Age-related loss of muscle, sarcopenia, is recognised as a clinical syndrome with multiple contributing factors. International European Working Group on Sarcopenia in Older People (EWGSOP) criteria require generalised loss of muscle mass and reduced function to diagnose sarcopenia. Both are common in COPD but are usually studied in isolation and in the lower limbs.
Objectives To determine the prevalence of sarcopenia in COPD, its impact on function and health status, its relationship with quadriceps strength and its response to pulmonary rehabilitation (PR).
Methods EWGSOP criteria were applied to 622 outpatients with stable COPD. Body composition, exercise capacity, functional performance, physical activity and health status were assessed. Using a case–control design, response to PR was determined in 43 patients with sarcopenia and a propensity score-matched non-sarcopenic group.
Results Prevalence of sarcopenia was 14.5% (95% CI 11.8% to 17.4%), which increased with age and Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD) stage, but did not differ by gender or the presence of quadriceps weakness (14.9 vs 13.8%, p=0.40). Patients with sarcopenia had reduced exercise capacity, functional performance, physical activity and health status compared with patients without sarcopenia (p<0.001), but responded similarly following PR; 12/43 patients were no longer classified as sarcopenic following PR.
Conclusions Sarcopenia affects 15% of patients with stable COPD and impairs function and health status. Sarcopenia does not impact on response to PR, which can lead to a reversal of the syndrome in select patients.
- COPD epidemiology
- Pulmonary Rehabilitation
- Clinical Epidemiology
Statistics from Altmetric.com
Key Messages
What is the key question?
-
What is the prevalence and impact of sarcopenia in COPD and does sarcopenia affect response to pulmonary rehabilitation?
What is the bottom line?
-
Sarcopenia affects 15% of patients with stable COPD and impairs exercise capacity, functional performance and health status, though it does not limit response to pulmonary rehabilitation.
Why read on?
-
We characterise the sarcopenia phenotype in COPD using internationally agreed criteria and demonstrate the impact of pulmonary rehabilitation, which can reverse the syndrome in select patients.
Introduction
Skeletal muscle dysfunction is a recognised manifestation of COPD.1 Key features include quadriceps weakness,2 atrophy3 and a type II fibre shift4 all of which are associated with a poor prognosis independent of lung function.5–7 Sarcopenia describes age-related loss of skeletal muscle, which leads to increased risk of physical disability, poor health status and death.8 ,9 Sarcopenia is increasingly recognised as a clinical syndrome with multiple contributing factors, including physical inactivity, malnutrition and chronic disease. Since COPD, in some respects, is considered a disease of accelerated ageing, one would hypothesise that sarcopenia would be relevant to patients with COPD.
In COPD, most studies examining dysfunction of skeletal muscle have focused on one aspect of sarcopenia, predominantly in the lower limbs.10 This contrasts with international consensus statements for sarcopenia, which emphasise the loss of both muscle mass and function in diagnostic criteria, and underscore the importance of generalised muscle dysfunction.8 In particular, assessment of a single aspect of sarcopenia is considered insufficient, as the relationship between muscle mass and strength is non-linear,3 because muscle atrophy does not always lead to impairment of function11 and cut points for weakness that relate to functional status are lacking.1 ,2
The European Working Group on Sarcopenia in Older People (EWGSOP) developed practical clinical diagnostic criteria for sarcopenia8 which are endorsed by international organisations and have been used to examine the prevalence and impact of the syndrome across settings12–14 and disease states.9 Though the term has been used loosely in COPD,15 data on consensus-defined sarcopenia are lacking, but are necessary to understand the size and nature of this problem in a disease characterised by differential muscle atrophy and weakness. Sarcopenia is relevant to many common disease management strategies, including exercise training10 and nutritional therapy.16 Given the advent of medicines directed at sarcopenia in other disease conditions, such data will also be useful for drug development.17
In this study, we used the EWGSOP criteria to determine the prevalence and risk factors for sarcopenia in COPD and to determine the impact of sarcopenia on functional exercise capacity and health status. We also sought to examine the relationship between sarcopenia and quadriceps strength and explore if sarcopenia can be reversed by exercise training as part of pulmonary rehabilitation (PR).
Methods
Participants
Patients diagnosed with COPD according to Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD) guidelines were recruited from outpatient respiratory clinics at Harefield Hospital (Harefield, Middlesex, UK) between April 2011 and January 2014. Exclusion criteria were unstable cardiac disease, an exacerbation within the preceding 4 weeks, predominant neurological limitation to walking (eg, significant hemiplegia) or contraindication to bioelectrical impedance analysis (BIA) including an implanted pacemaker or defibrillator. All participants gave written informed consent.
Assessments
Sarcopenia was defined according to the EWGSOP criteria.8 Skeletal muscle mass (SMM, kg) was estimated using whole-body BIA and Skeletal Muscle Mass Index (SMI) calculated as SMM/height2. Handgrip strength was measured using a handheld dynamometer and physical performance by the 4-metre gait speed (4MGS), as previously described.18 ,19 The following cut-off values were used to identify sarcopenia: SMI of ≤8.50 kg/m2 for men and ≤5.75 kg/m2 for women,20 and either handgrip strength of <30 kg for men and <20 kg for women, or a gait speed of <0.8 m/s.8 ,21
Further measurements included the incremental shuttle walk test (ISWT), five-repetition sit-to-stand test (5STS), short physical performance battery (SPPB), quadriceps maximum voluntary contraction (QMVC), St George's Respiratory Disease Questionnaire and COPD Assessment Test. Physical activity was assessed by the modified Minnesota Leisure-time Physical Activity Questionnaire and, in a subgroup, by a multisensory accelerometer (SenseWear, Bodymedia, Pittsburgh, USA) which integrates biaxial accelerometry (longitudinal and transverse planes) with multiple physiological measures including galvanic skin resistance and body temperature to calculate estimates of energy expenditure.22 The iBODE composite prognostic index (Body mass index, airflow Obstruction, Dyspnoea, and Exercise capacity) was calculated. Comorbidity burden was assessed by the Charlson index. Full details and references are found in the online supplement.
Pulmonary rehabilitation
The PR programme was an 8-week outpatient multidisciplinary exercise and education programme comprising two supervised and at least one additional home session per week. Further details of exercise prescription and educational content are found in the online supplement.
Statistical analysis
Data are presented as mean (SD) or median (25th, 75th percentiles) where data were not normally distributed. The prevalence of sarcopenia with 95% CIs was determined and compared according to gender, age, GOLD staging, iBODE and quadriceps weakness2 using the χ2 for trend test with posthoc comparisons between a reference group with the lowest prevalence. Baseline characteristics were compared between groups according to the presence of sarcopenia, or low SMI, handgrip strength, or 4MGS alone using one-way analysis of variance or Kruskal–Wallis tests with posthoc comparisons.
Response to PR was calculated for patients with sarcopenia who had attended ≥50% of the supervised sessions (≥8/16) and had completed a post-PR assessment. A matched group of patients without sarcopenia fulfilling these criteria were identified by using propensity score matching,23 considering baseline age, gender, FEV1% predicted, Medical Research Council dyspnoea score, and ISWT distance as moderators of PR outcome. Change from pre-PR to post-PR was compared between groups using independent t test or Mann–Whitney U test. Analyses were performed using SPSS (V.21, IBM, New York, USA). To control for Type I errors in view of multiple testing, a p value <0.01 was considered significant.
Results
Prevalence of sarcopenia in COPD
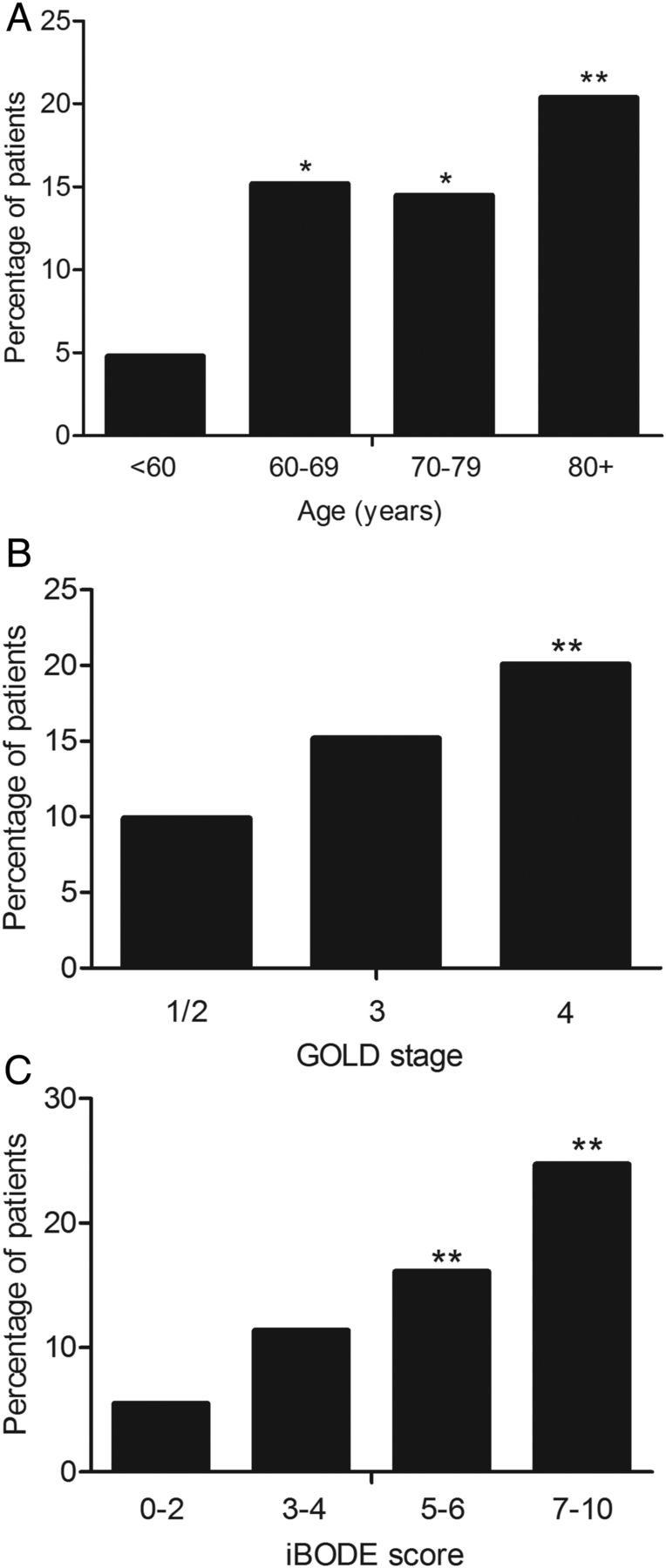
Six hundred and twenty-two outpatients with stable COPD were studied. The overall prevalence of sarcopenia was 14.5% (11.8% to 17.4%). A flowchart, according to the EWGSOP algorithm, is outlined in online supplementary figure S1. Prevalence did not differ by gender (men 16.1% (12.4% to 20.3%) vs women 12.3% (8.6% to 16.9%); p=0.20), but increased with age (p=0.020) (figure 1A) and GOLD stage (p=0.005), with a twofold increase in stage IV, 20.1% (14.2% to 27.2%) as compared with stage I/II disease, 9.9% (6.4% to 14.5%) (figure 1B). Prevalence also increased with iBODE score (p<0.001) and was lowest in the quartile with the best prognosis (iBODE 0–2: 5.5% (2.4% to 10.5%)) and highest in the quartile with the worst prognosis (iBODE 7–10: 24.7% (18.1% to 32.3%)) (figure 1C).

Prevalence of sarcopenia according to age (A), disease severity (B), and Body mass index, obstruction, dyspnoea, exercise capacity index (iBODE) (C). Between-group differences compared with base group (far left) denoted by * <0.05 or ** <0.01.
Factors associated with sarcopenia in COPD
Baseline clinical characteristics, according to the presence of low SMI, low physical function or sarcopenia, are shown in table 1. About one-third of the patients met none of the criteria and over half of the patients met one of the criteria, most often low physical function (figure 2A). Low muscle mass alone impacted adversely on 5STS but not on other outcomes of physical functions, such as 4MGS, ISWT or SPPB, or on self-reported physical activity (table 1). Patients with sarcopenia were significantly older, had more airflow obstruction and reduced quadriceps strength, exercise capacity, functional performance, subjective and objective physical activity and health status compared with patients without sarcopenia. There were no significant differences in smoking status, number of comorbidities, self-reported hospital admissions or exacerbations between groups (table 1).
Baseline clinical characteristics expressed as n/%, mean (SD) and median (25th and 75th centiles)

Relationships between sarcopenia and (A) low muscle mass or function, and (B) quadriceps weakness.
Of the 622 patients, 554 patients had QMVC measured. When patients were classified according to quadriceps weakness, there was no significant difference in the prevalence of sarcopenia between groups (weak: 14.9% (11.2% to 18.6%) vs normal: 13.8% (10.2% to 18.0%), p=0.404). Furthermore, of the 90 patients who were sarcopenic, 33 (36.7%) did not present with quadriceps weakness (figure 2B). Clinical characteristics, according to the presence of quadriceps weakness, sarcopenia or both, are found in the online supplementary table S1.
Response to PR
Patients with and patients without sarcopenia attended a mean (SD) of 13 (2) and 13 (3) PR sessions, respectively. Following PR, there were no statistical differences for change in outcomes of body composition, functional performance or health status between patients with and patients without sarcopenia (table 2). In the sarcopenic group, SMI, handgrip strength and 4MGS improved by a mean of 0.11 kg/m2, 2.08 kg and 0.12 m/s, respectively, such that 12/43 patients (28%) no longer met EWGSOP criteria for sarcopenia. Adherence was similar in patients whose state was reversed and unchanged (14 (2) vs 13 (2) sessions). Three patients had a change in both mass and functional status, six patients had a change in SMI only and three patients changed their functional status (one improved gait speed and two improved handgrip strength). These patients were generally closer to cut-offs for SMI and function at baseline (figure 3).
Comparison of response to pulmonary rehabilitation between sarcopenic and propensity-matched patients with non-sarcopenic COPD expressed as mean (95% CI)

{kind=link}
{kind=link}
{kind=link}
Response to pulmonary rehabilitation (PR) in sarcopenic male (closed circles) and female (open squares) patients according to European Working Group on Sarcopenia in Older People criteria for diagnosing sarcopenia. SMI, Skeletal Muscle Mass Index.
Discussion
We have identified a 14.5% prevalence of sarcopenia in patients with stable COPD as defined by EWGSOP criteria,8 which increased with age and disease severity. Sarcopenia was distinct from the loss of quadriceps strength alone and was associated with reduced functional performance, exercise capacity and quality of life. Despite this, sarcopenia did not appear to impact on response to PR. In about one-quarter of patients, PR completion led to a reversal of their sarcopenia status.
Critique of the method
Various definitions for sarcopenia have been proposed24 including some that only consider muscle mass, as suggested within the recent European Respiratory Society (ERS) statement for nutritional assessment and therapy.16 The current international consensus is that the sarcopenia syndrome includes the presence of both low muscle mass and function, hence, our decision to adopt the EWGSOP criteria.8 Our study supports the construct validity of these criteria which identified sarcopenic patients as having the greatest levels of impairment across a range of domains. Our large cohort of well-phenotyped patients with stable COPD provides an accurate estimation of overall prevalence of sarcopenia, and allows for detailed study around the effects of sarcopenia on clinical outcome. The use of EWGSOP criteria also permits comparison of prevalence and characteristics of a sarcopenic phenotype in COPD with other patient groups.
We acknowledge that this study was undertaken in ambulatory hospital outpatients, and hence, our findings need to be corroborated in other COPD subgroups including those with mild disease and those hospitalised with an acute exacerbation. Nonetheless, this is the first study to have examined EWGSOP defined sarcopenia in COPD. We also acknowledge debate around the use of BIA for the assessment of muscle mass, as compared with alternative methods, such as dual-energy X-ray absorptiometry (DEXA) or MRI. Previous studies have shown that BIA underestimates muscle mass compared with DEXA.25 Our cut-off values also arose from international cohorts, and their application to a UK setting requires testing. However, this offers a simple, portable assessment that was considered acceptable by the EWGSOP. Our data also raise an exemplary issue in the assessment of sarcopenia in chronic diseases. Specifically, while a low SMI is (within technical limitations) incontrovertible evidence of low muscle mass, low function may reflect both the primary disease process as well as secondary muscle dysfunction. This may overestimate the prevalence of EWGSOP defined sarcopenia, and in that context, we note that prevalence increased with spirometrically-defined disease severity.
Significance of the findings
This is the first study to examine sarcopenia in COPD using EWGSOP criteria. Previous studies in community-dwelling and hospitalised older adults report lower overall prevalence rates26–29 than found in our cohort. Patel et al26 reported an overall prevalence of 6.8% and 7.8% in community-dwelling older adults using DEXA to define low muscle mass. The Belgian BELFRAIL study reported prevalence in 288 adults aged ≥80 years and found that 12.5% were sarcopenic,27 similar to the prevalence in our COPD cohort, who had a mean age of 71 years. We demonstrated an association between the presence of sarcopenia and disease severity according to GOLD stage and composite prognostic indices. No previous studies have examined this relationship; though our observation is in keeping with Schols et al,30 who found a low body mass index (BMI) (<21 kg/m2) and a low Fat-Free Mass Index (<16/15 for males/females) was more prevalent in patients with stage IV compared with stages II–III disease.
There was no difference in prevalence of sarcopenia between patients with or without quadriceps weakness, and one-third of sarcopenic patients had preserved quadriceps strength. In both regards, sarcopenia appears to be a distinct phenotype, which cannot be identified by generalised wasting or localised weakness alone. Our findings also suggest that loss of quadriceps strength may precede loss of whole-body muscle mass in COPD. Specifically, the prevalence of quadriceps weakness was high (315 of 554 patients in whom it was measured), but of these, only 47 patients with quadriceps weakness met EWGSOP criteria for sarcopenia, while an additional 33 met the criteria without evidence of quadriceps weakness. Multiple aetiologies underlie the muscle dysfunction observed in COPD, which is characterised by atrophy, weakness and a shift towards a less oxidative fibre-type profile.1 ,9 Physical inactivity is a generally agreed precipitating factor and patients with sarcopenia had the lowest daily step count and energy expenditure based on self-reported and objective assessments. Other aetiological factors, such as hypoxaemia, inflammation, medication, may also have an adverse effect on the muscular system, and contribute to the sarcopenic state.10
Few studies have investigated a differential response to rehabilitation in patients with sarcopenia. Liu et al31 followed older adults with mobility disabilities undertaking a 12 to 18-month exercise programme and found no significant difference in the adherence rate of patients with and patients without sarcopenia (74% vs 71%, respectively, p=0.59). COPD patients with sarcopenia responded well to PR, with improvements in functional performance, exercise capacity, lower and upper limb strength, and health status, similar to those gained by patients without sarcopenia and exceeding known minimally important differences.32 ,33 Although observed improvements were equivalent, patients with sarcopenia started PR from a lower baseline; they were weaker, had a lower BMI, reduced exercise capacity and functional performance. To this end, we were able to demonstrate that PR can reverse sarcopenia in select patients, in particular, those with an SMI or functional performance that was close to the cut-off threshold at baseline. The reversal of the state in 12/43 (28%) patients was helped by the EWGSOP diagnostic criteria; an improvement in either SMI or an aspect of function across a cut-off led to a state reversal. In this respect, the criteria are operationally more likely to show benefit from exercise and nutritional interventions, which impact favourably on function as well as muscle mass. Nonetheless, a larger proportion of patients maintained their sarcopenia status, supporting a role for testing pharmacological adjuncts in selected patients.
The risk associated with sarcopenia in COPD has not yet been studied, and future longitudinal studies are required to examine its impact on adverse events and survival. In older nursing-home residents, Landi et al34 demonstrated that sarcopenia was associated with increased risk of all-cause mortality, and in a separate cohort of acutely unwell older patients, sarcopenia increased the risk of non-elective readmission and mortality.13 Aspects of muscle dysfunction and low functional performance have previously been related to adverse outcomes in COPD,5–7 ,35 though the serious consequences of the sarcopenia syndrome warrant further research to establish the risk it carries in patients with COPD.29 ,30
In conclusion, there is a 15% prevalence of sarcopenia in patients with COPD. The sarcopenia phenotype is associated with reduced function, exercise capacity and health status, and is distinct from localised quadriceps weakness. Sarcopenia does not appear to impact on response to PR in COPD, which can lead to a reversal of the syndrome in select patients.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
SEJ and MM contributed equally.
-
Contributors WD-CM is the overall guarantor of this manuscript and takes responsibility for the content, including the data and analysis. The original study conception was by WD-CM and MM. SEJ, SSCK, JLC, CMN and ALC contributed to data acquisition. SEJ and MM undertook the initial analysis of data, which was then reviewed by WD-CM and MIP. SEJ and MM produced a first draft of the manuscript. All authors critically revised the manuscript and approved the submitted version.
-
Funding SEJ, JLC and MIP are fully or partly funded by the NIHR Respiratory Biomedical Research Unit at the Royal Brompton and Harefield NHS Foundation Trust and Imperial College London. MM is supported by a National Institute for Health Research (NIHR) Post-Doctoral and a Clinical Trials Fellowship. SSCK is supported by the Medical Research Council. CMN is supported by a NIHR Doctoral Fellowship. WD-CM is supported by a National Institute for Health Research Clinician Scientist Award (CS/7/007), a Medical Research Council (UK) New Investigator Research Grant (G1002113) and a National Institute for Health Research Clinical Trials Fellowship (NIHR-CTF-01-12-04). This project was undertaken at the NIHR Respiratory Biomedical Research Unit at the Royal Brompton and Harefield NHS Foundation Trust and Imperial College London. The views expressed in this publication are those of the authors and not necessarily those of the NHS, the NIHR nor the Department of Health.
-
Competing interests MIP has received personal reimbursement for lecturing or consultancy regarding muscle function in COPD from Novartis and Philips Respironics; he discloses institutional reimbursement for consultancy from GlaxoSmithKline, Novartis, Regeneron, Lilly, Biomarin and Boehringer Ingelheim and institutional agreements to do research with GlaxoSmithKline, Novartis, AstraZeneca and Philips Respironics. All other authors declare that they have no conflicts of interest.
-
Ethics approval West London (11/H0707/2) and London Camberwell St Giles (11/LO/1780) research ethics committees.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement There are no unpublished data from this study. Additional data can be found in the online supplement.