Article Text

Abstract
Background Compliance with continuous positive airway pressure (CPAP) therapy is essential in patients with obstructive sleep apnoea (OSA), but adequate control is not always possible. This is clinically important because CPAP can reverse the morbidity and mortality associated with OSA. Telemedicine, with support provided via a web platform and video conferences, could represent a cost-effective alternative to standard care management.
Aim To assess the telemedicine impact on treatment compliance, cost-effectiveness and improvement in quality of life (QoL) when compared with traditional face-to-face follow-up.
Methods A randomised controlled trial was performed to compare a telemedicine-based CPAP follow-up strategy with standard face-to-face management. Consecutive OSA patients requiring CPAP treatment, with sufficient internet skills and who agreed to participate, were enrolled. They were followed-up at 1, 3 and 6 months and answered surveys about sleep, CPAP side effects and lifestyle. We compared CPAP compliance, cost-effectiveness and QoL between the beginning and the end of the study. A Bayesian cost-effectiveness analysis with non-informative priors was performed.
Results We randomised 139 patients. At 6 months, we found similar levels of CPAP compliance, and improved daytime sleepiness, QoL, side effects and degree of satisfaction in both groups. Despite requiring more visits, the telemedicine group was more cost-effective: costs were lower and differences in effectiveness were not relevant.
Conclusions A telemedicine-based strategy for the follow-up of CPAP treatment in patients with OSA was as effective as standard hospital-based care in terms of CPAP compliance and symptom improvement, with comparable side effects and satisfaction rates. The telemedicine-based strategy had lower total costs due to savings on transport and less lost productivity (indirect costs).
Trial register number NCT01716676.
- Sleep apnoea
Statistics from Altmetric.com
Key messages
What is the key question?
What is the clinical and economic impact of a telemedicine-based approach for the follow-up of continuous positive airway pressure (CPAP) treatment in patients with obstructive sleep apnoea (OSA)?
What is the bottom line?
Adherence to CPAP treatment is essential for treatment success; telemedicine could provide a cost-effective alternative to the standard face-to-face approach of CPAP follow-up.
Why read on?
This multicentre randomised controlled trial provides evidence that a telemedicine-based strategy for the CPAP follow-up of OSA patients is as effective as the face-to-face approach but has lower cost for society.
Introduction
Obstructive sleep apnoea (OSA) is a common condition that causes significant morbidity and mortality and increased use of healthcare resources.1 ,2 Currently, improved case detection and the resulting higher healthcare demands have not been accompanied by any real improvement in OSA management. In addition, health resources assigned to OSA and its treatment have been found to be inadequate.3 Continuous positive airway pressure (CPAP) is the optimal treatment for OSA. Nevertheless, many patients fail to use CPAP adequately; this is clinically relevant since increased adherence reduces symptoms and comorbidities.4 Optimising adherence is therefore an essential aspect of patient management and different educational and technical measures have been proposed.5 ,6–10 However, adequate provision of such support is not always possible, and overloaded sleep centres can be hard-pressed, especially after recent healthcare budget cuts. Therefore, alternative and cost-effective approaches are urgently needed to improve OSA management and to promote CPAP compliance. A possible approach is telemedicine, defined here as the use of information and communication technology (ICT) to provide clinical care for a patient at a distance.11 However, conflicting results have been found12 ,13 and the economic impact of telemedicine on OSA management is still unclear.14–18 We conducted a multicentre randomised controlled trial (RCT) to evaluate the efficacy of a new telemedicine-based strategy for OSA patients under CPAP treatment. Specifically, we assessed its impact on treatment compliance, sleepiness, quality of life (QoL) and cost-effectiveness when compared with traditional face-to-face follow-up.
Methods
Study design
This RCT was approved by the ethics committees of the eight participating hospitals in Spain. All patients provided informed consent prior to participation. Patients were randomly assigned to either standard face-to-face follow-up (control group) or to telemedicine-based follow-up for 6 months (figure 1).

Study flowchart. The two groups received CPAP treatment follow-up via two different strategies: conventional follow-up, which consisted of face-to-face hospital visits (the control group), and telemedicine-based follow-up, using a website and televisits (the telemedicine group). The main outcomes were CPAP compliance, QoL and cost-effectiveness. During the intermediate visits, only questionnaires were administered and some corrective actions were recommended if required. CPAP, continuous positive airway pressure; ITT, intention-to-treat; OSA, obstructive sleep apnoea; PP, per protocol; QALY, quality-adjusted life year; QoL, quality of life.
Population
Participants were prospectively enrolled between December 2011 and December 2013. In accordance with Spanish health service guidelines, all enrolled patients were classified as requiring CPAP treatment after an overnight study.19 Exclusion criteria were as follows: severe sleepiness, severe nasal obstruction, pregnancy, psychiatric disease, dangerous employment, clinical instability and current or previous treatment for OSA. We excluded patients who lacked sufficient internet skills or refused to participate in the study. Both groups were equipped with conventional masks and received the same instructions regarding initial CPAP use.
Procedures
Clinical evaluation and follow-up
Patients’ baseline characteristics were collected at the initial visit. In addition, EuroQol-5D, the Epworth Sleepiness Scale (ESS), the Functional Outcomes of Sleep Questionnaire (FOSQ) and the Quebec Sleep Questionnaire (QSQ) were administered. At 6 months, data on CPAP compliance, satisfaction and side effects were gathered and questionnaires repeated. Data related to costs were collected for the entire process. At intermediate visits (months 1 and 3), additional information was recorded regarding side effects, lifestyle changes and actions taken.
Sleep studies
All patients underwent a sleep study which was scored manually by trained personnel.19 Optimal CPAP pressure was titrated by an auto CPAP device to obtain a fixed pressure.20 Tests were repeated if patients claimed to sleep less than 4 h, or when less than 5 h of recording were available.
Randomisation
Participants who completed the baseline visit were randomly assigned (1:1) to the control or telemedicine group. Randomisation was at an individual level without restriction (ie, no blocking) and was completely automated by use of an unseen random number function embedded in the data collection website code. There was no clinician involvement at this stage, and the software only revealed the allocation group when an investigator provided the data of a fully eligible patient, thus guaranteeing concealment of the randomisation sequence.
Telemedicine-based follow-up
Patients randomised to the telemedicine group received their follow-up at home supported by a website developed for this study, where they could find information about OSA and CPAP therapy, and a biweekly six-item questionnaire about their status, physical activity, sleep time, CPAP use and treatment side effects. Each centre's staff monitored questionnaire answers and communicated with patients through the website messaging tool to solve treatment-related problems. To participate, patients only required an internet-connected device with a microphone and webcam. Televisits via video conference were undertaken at months 1 and 3. We used Skype due to its availability, ease of use and good performance.21 Patients automatically received a confirmation email indicating the date and time of their appointment. Extra televisits or hospital visits were scheduled as necessary.
Hospital-based follow-up
As shown in figure 1, patients randomised to the control group had the same follow-up schedule as the telemedicine group, but attended the hospital. Specifically, they received standard face-to-face follow-up with visits at months 1, 3 and 6, and extra visits if needed.
Outcomes
The primary outcomes were: (1) CPAP compliance; and (2) the cost-effectiveness of the two follow-up strategies, compared using quality-adjusted life years (QALYs) as a measure of effectiveness. QALYs were estimated from the EQ-5D tariffs.22–24 Secondary outcomes included questionnaire changes from baseline, CPAP treatment side effects and patient satisfaction.
Cost analysis
We adopted a societal perspective in the cost-effectiveness analysis, where both direct and indirect costs were considered but immaterial costs were not taken into account. Direct health costs were associated with the use of healthcare resources, such as medical and nursing personnel salaries and all costs related to follow-up. These included material costs such as masks, humidifiers and medications used by patients, as well as the costs of extra visits to respiratory physicians, other specialists, general practitioners, nurses and emergency services. Two types of extra visits were defined: OSA-related and non-OSA-related. Unit costs were provided by the administrative departments of one of the participating hospitals.
Direct non-health costs referred to the travel expenses incurred by patients when attending hospital. Indirect costs referred to the opportunity costs of lost productivity and work due to follow-up visits; we considered time lost due to both hospital visits and video conferences. The final visit after 6 months was a face-to-face visit for both groups; this was included in the protocol to allow comparison with the data obtained at the first visit. However, in normal practice this face-to-face visit would not be needed for the telemedicine group. For this reason, the costs of transport to the 6-month visit were not considered in the cost analysis for the telemedicine group, and we assumed indirect costs similar to those for the intermediate visits.
The total costs were evaluated against the QALYs through a Bayesian cost-effectiveness analysis. Other complementary cost-effectiveness analyses were assessed, taking into account changes in the ESS and CPAP treatment compliance.
Statistical analysis
We considered two analysis populations for this trial: an intention-to-treat (ITT) population (all randomised patients) and a per protocol (PP) population (all randomisation patients who finished the study). The planned sample size was based on the assumptions that 85% of the patients who were randomly assigned to treatment would meet the above definition of a PP sample for the non-inferiority test. The study was based on the assumption that the average compliance without intervention would be 4 h/day (SD 1.8). According to a one-sided type I error of 0.025 and 80% power to verify that CPAP compliance in the telemedicine group was not less than 1 h/day (SD 2), and assuming a 10% drop-out rate, the sample size was 60 patients in each group.
We reported means and SD for continuous variables with normal distribution and medians (1st quartile–3rd quartile) for those with non-normal distribution, and compared them using the t test or the non-parametric Mann–Whitney test, respectively. Categorical variables are presented as number of patients (%) and were compared using the χ2 test or Fisher exact test.
Conventional regression imputation techniques were used to estimate values for patients without valid CPAP use measurements at 6 months, assuming that missing data were missing at random. For the 16 patients with missing CPAP use at 6 months (eight in the control group and eight in the telemedicine group), we generated values based on sex, age, baseline snoring, witnessed apnoeas, choking episodes, nocturia, daytime sleepiness, non-restorative sleep, daytime fatigue, drowsiness during driving, nasal problems and ESS score, using stochastic regression imputations by a linear regression method.
The non-inferiority analyses were based on the PP sample according to International Committee for Harmonization (ICH) E9 guidelines.25 Non-inferiority of the telemedicine group compared with control was assessed by a one-sided 97.5% CI for the point estimate of the difference between the two groups, calculated by adequacy of CPAP adherence, using two-sample t tests.
Overall efficacy analyses were conducted using the ITT sample. We evaluated treatment effects by two-sided tests with a significance level of α=0.05. Multiple linear regression analysis was performed to assess the relationship between potential predictive factors and CPAP compliance (dependent variable). Details about variable selection are provided in online supplementary material. We compared continuous efficacy measures between groups using analysis of covariance (ANCOVA) models with adjustment for baseline variables and centre. We analysed categorical efficacy and safety measures by using logistic regression models.
All analyses were performed with IBM SPSS Statistics V.20.0.
Cost-effectiveness analysis
The cost-effectiveness analysis was carried out in a Bayesian framework.26 ,27 Considering the asymmetry in the cost distribution and the correlation between effectiveness and cost, we assumed a multivariate normal distribution for the effectiveness and the log-transformed costs. In a Bayesian analysis, the prior distributions for the parameters of the model should be defined. We used non-informative priors to let the sample data control the posterior distribution. We estimated posterior distributions using Markov Chain Monte Carlo methods.28 The expected mean effectiveness and costs, and 95% Bayesian credible interval were then estimated from the posterior distributions. Moreover, we assessed the incremental effectiveness and cost, and the probability that telemedicine would be more effective or cheaper than control. To illustrate the results, we used the cost-effectiveness plane, where the joint posterior distribution of the incremental effectiveness and costs are displayed in an x-y plot, and the cost-effectiveness acceptability curve (CEAC), where the probability of preference for telemedicine is displayed as a function of the willingness to pay for a QALY.29 Furthermore, for certain combinations between groups, we assessed the incremental effectiveness, incremental cost and incremental net benefit.
Results
Of the 240 patients screened, 139 were randomised and 123 (88%) completed the study (figure 1). Data are reported on an ITT basis unless otherwise stated. Both groups had similar baseline characteristics (table 1), except for lower mean age in the control group.
Baseline characteristics
CPAP adherence
Mean CPAP use was 4.2±2.0 h/day in the control group and 4.4±2.0 h/day in the telemedicine group (p=0.827). When using the accepted definition of adequate adherence (>4 h/day), 57% of controls had adequate compliance compared with 65% of the telemedicine group (p=0.329).
On bivariate analysis, several variables were significantly associated with CPAP compliance (see online supplementary table S1). Among these variables, in the multivariate analysis CPAP compliance was significantly influenced by age and self-reported daytime fatigue at the end of the study.
In the non-inferiority analysis, using the PP sample the point estimate of the difference in CPAP compliance (telemedicine minus control) was 0.04. The lower bound of the one-sided 97.5% CI for the point estimate was −0.72 for the PP sample, which exceeded the previously specified −1 margin and met the criteria for non-inferiority (see online supplementary figure S1).
Clinical outcomes
As shown in table 2, we found general improvements in QoL and sleepiness (ESS) after 6 months of CPAP treatment, but there were no significant differences in change from baseline between the telemedicine and control groups, except for FOSQ (−0.89; 95% CI −1.70 to −0.08; p=0.031). There was no change in body mass index (BMI) in either group. Similar reductions were seen in the most common OSA symptoms (snoring, witnessed apnoeas, nocturia) in both groups after CPAP treatment (table 3). The side effects of CPAP treatment were comparable between the two groups at the end of the study (see online supplementary table S2). The two groups reported similar degrees of satisfaction with the follow-up procedures (see online supplementary tables S3 and S4).
Comparison of change from baseline in QoL, ESS and BMI between the telemedicine and control groups
Comparison of typical OSA symptoms between the telemedicine and control groups
Resource use and cost analysis
Table 4 shows the average use of resources and costs of both follow-up strategies. There were no significant differences in the average lengths of follow-up visits or mask changes. The telemedicine group required more extra visits: 16.7% and 28.3% of these patients visited a physician or a nurse, respectively, during the 6-month treatment period, compared to rates of 7.9% and 9.5% in the control group, with a significant difference found for nurse visits. Visits to general practitioners and emergency services were more frequent in the telemedicine group, although the differences were not statistically significant. The number of visits to general practitioners was lower when only OSA-related visits were considered (falling from 28 to 12 for the control group and from 40 to 9 for the telemedicine group). Only one visit to the emergency service was OSA related. The main differences between groups concerned the time required for travelling to the hospital and the missed work due to face-to-face visits.
Cost analysis
Cost-effectiveness analysis
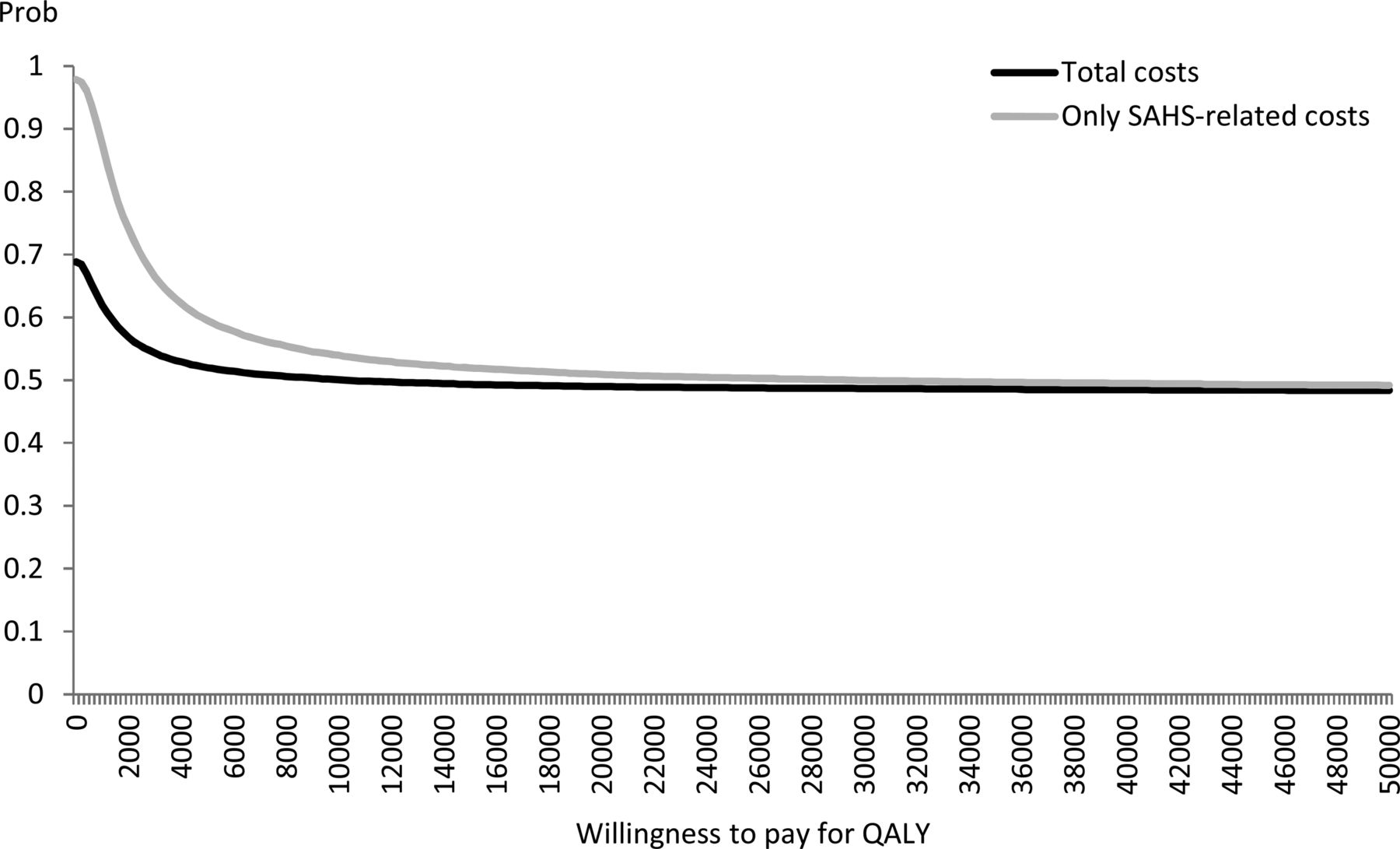
Table 5 summarises the cost-effectiveness analysis. The mean total costs were €180.4 and €168.4 for the control and telemedicine groups, respectively. The estimated probability that telemedicine would be cheaper than control was 68.8%. When only OSA-related visits and drugs were considered, the estimated cost for the control group was €150.9 and €114.5 for the telemedicine group; this also increased the probability to 97.9%. The efficacy measure (QALYs) was lower on average for the telemedicine group compared with the control group, although the difference was not statistically significant. The posterior distribution of the incremental effectiveness and incremental cost are showed in figure 2. Figure 3 shows the CEAC. Since the telemedicine-based strategy was cheaper than the hospital-based follow-up, it was preferable in situations with low willingness to pay. At a standard willingness-to-pay threshold of €20 000–30 000 per QALY, the two procedures were equally cost-effective. CPAP compliance and ESS improvements were considered alternative measures of effectiveness, but neither resulted in statistically relevant differences.
Cost-effectiveness analysis

Cost-effectiveness acceptability plane. A scatterplot of the posterior cost and effectiveness differences. Grey points represent OSA-related costs and black points represent total costs. OSA, obstructive sleep apnoea; SAHS, sleep apnoea-hypopnoea syndrome.
{kind=link}
{kind=link}
{kind=link}
Cost-effectiveness acceptability curve showing the cost-effectiveness probabilities for telemedicine-based follow-up by different degrees of willingness to pay for QALYs. QALY, quality-adjusted life year; SAHS, sleep apnoea-hypopnoea syndrome.
Discussion
In this multicentre RCT, we compared a new telemedicine-based follow-up strategy for OSA against standard face-to-face follow-up over a 6-month treatment period. Although the study groups achieved similar levels of CPAP use and clinical outcomes, probably due to the low possibility of further improvement in our setting, where levels of compliance are generally high,30 analyses showed telemedicine to be more cost-effective, with travel costs and lost work time being the most important sources of savings. Interestingly, the telemedicine group made more extra visits than the face-to-face group, but most of them were non-OSA-related. This may be explained by the fact that telemedicine improved the communication between professionals and patients, thereby increasing the detection of non-OSA-related problems.
CPAP is the optimal treatment for OSA,31 but adherence fails in some subjects. After analysing the relationship between compliance and effects on symptoms in 30 articles (2047 participants), a 2014 Cochrane review emphasised the need for new strategies that promote CPAP compliance and assessment of their cost-effectiveness.32 Our study analysed these two aspects (adherence to treatment and cost-effectiveness) in a novel telemedicine-based approach for CPAP follow-up.
The application of ICT is increasing in clinical practice for different diseases but prudence is required, especially after some recent negative results.12 ,13 Some authors have highlighted the need for a better understanding of the factors that predict success in telemedicine programmes before they are widely implemented, stressing the importance of appropriate patient selection.33 In a previous study we demonstrated that an OSA population could benefit from a telemedicine-based management approach.34
Diverse results have been found for telemedicine interventions designed to improve CPAP compliance in OSA.14–18 Sparrow et al14 randomly assigned 250 patients starting CPAP therapy either to a telephone-linked interactive voice-response system or to an attention placebo control for 12 months. Patients in the telemedicine group showed improvements but result interpretation is limited due to generally low CPAP adherence.14 Similar limitations were found in another RCT that assessed the application of a CPAP wireless telemonitoring system.15 Other telemedicine interventions, such as televisits, improved CPAP adherence in a small group of non-compliant OSA patients.16 Nevertheless, other studies have not found any positive effects.17 ,18 In summary, the results vary widely, and most studies were single-centre with low levels of CPAP compliance and small sample sizes. Moreover, very few performed cost-effectiveness analyses.
In a recent systematic review of the cost-effectiveness of telemedicine, the authors stated that, even though the use of this technological approach has grown over the last 30 years, decisions are still influenced by financial constraints.35 As mentioned, Wilson and colleagues33 reached similar conclusions. Therefore, the cost-benefit ratio of telemedicine-based health strategies has still to be established. The Bayesian cost-effectiveness analysis used in this paper is well suited to this scenario, where there are small differences in the effectiveness of the proposed strategies; that is, where there is a non-negligible probability of a very small value for the denominator of the incremental cost-effectiveness ratio. In that situation, the Bayesian model allows us to estimate the parameters of interest by introducing a non-informative prior density.
In our analyses we identified as key factors the costs related to patients’ transport to the hospital and missed work time. Therefore, our telemedicine-based approach could be especially advantageous if applied to the working population and to residents in medically underserved areas. It is also reasonable to expect that this new management strategy could be suitable in clinical settings or health systems that achieve lower compliance levels with conventional follow-up. As it should be for any treatment option, appropriate patient selection remains a key issue. Also, specific training of the staff involved in long-distance follow-up would be necessary for optimal implementation.
As recommended by major guidelines regarding the application of cost-effectiveness analysis, we adopted the societal perspective where all costs are considered regardless of who pays. However, from the healthcare payer perspective, the telemedicine-based strategy would be more expensive than face-to-face follow-up (mean total costs would be €126.6 and €116.8, respectively), confirming that the main savings are related to patients’ transport to hospital and loss of productivity.
Although the economic analyses in this study were rigorous and extensive, some limitations are worthy of note. We did not consider the indirect hospital costs or the costs of the equipment needed to connect to the website. In addition, it could be argued that a significant number of patients with OSA do not have sufficient computer expertise; in our study approximately 40% of screened patients lacked such skills. However, given the current exponential growth of internet and mobile phone use, this percentage is likely to decrease over the next few years.
In this multicentre RCT we compared standard hospital-based CPAP follow-up with a novel telemedicine-based strategy. We conclude that the telemedicine procedure was more cost-effective due to savings related to transport and productivity losses. Patient satisfaction and side effects were similar. Therefore, telemedicine represents a cost-effective strategy to support the routine clinical follow-up of OSA patients receiving CPAP treatment. Moreover, we believe that a telemedicine-based strategy could provide an excellent alternative approach when adequate face-to-face consultations are impractical.
Acknowledgments
The authors would thank Mr. Albert Gabarrus for his support with statistical analysis of the study data. A special thanks to Esteve-Teijin for their support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Collaborators Spanish Sleep Network: Ester López, Hospital Universitario de Bellvitge, Hospitalet del Llobregat, Spain; Mercè Gasa, Hospital Universitario de Bellvitge, Hospitalet del Llobregat, Spain; Estefania García-Ledesma, Hospital San Pedro de Alcántara, Cáceres, Spain; Maria-Isabel Rosco-Due, Hospital San Pedro de Alcántara, Cáceres, Spain; Joaquín Durán, Unidad del Sueño, Hospital Universitario Araba, Vitoria-Gasteiz, Spain; Nuria Reyes-Nuñez, Hospital Universitario de Valme, Sevilla, Spain; Susana Pou, Hospital Germans Trias i Pujol, Universidad Autónoma de Barcelona, Badalona, Spain; Félix del Campo, Servicio de Neumología, Universidad de Valladolid, Valladolid, Spain; Gabriel Sampol, Hospital Universitario Vall d'Hebron, Barcelona, Spain; Odile Romero, Hospital Universitario Vall d'Hebron, Barcelona, Spain; Marta Torres, Centro de Investigación Biomédica en Red de Enfermedades Respiratorias (CIBERES), Madrid, Spain.
Contributors All the authors are responsible for and confirm the accuracy and completeness of the data and analyses. VI and JMM are the guarantors of the manuscript. VI was the clinical research fellow for the trial, participated in the trial design, was responsible for creating the website and for the oversight of the trial, and is the first author of the report. MAN, FJVP and MME were responsible for the cost-effectiveness analyses and for the revision of the final version of the manuscript. CM, JFM, NF, AA, FCR, CR, JA, MG, PLL, CE, MP, JP, MD, NS, JC, BJ, CL, CE, AM, OP, MA and RC contributed to the study concept, data collection and approval of the final version of the manuscript. VI, CE, MD, RF and JMM contributed to the data interpretation and manuscript preparation. FJVP, RF and JMM contributed to the study concept and design, and provided critical revision of the manuscript.
Funding This project was supported by SEPAR/FIS PI14/00416 and ECO2013-47092 (MINECO, Spain).
Competing interests None declared.
Ethics approval The Ethics Committee of each of the participating centres approved this study.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves