Article Text

Abstract
Background Guidelines advocate the use of spirometry to assess pulmonary function in asthmatic patients. Commonly used measures include forced expiratory volume in 1 second (FEV1), forced expiratory ratio (FEV1/FVC) and forced mid-expiratory flow between 25% and 75% of forced vital capacity (FEF25–75). Impulse oscillometry (IOS) is an effort independent test performed during tidal breathing. IOS may be used to assess the total and central airway resistance at 5 Hz (R5) and 20 Hz (R20) respectively and hence derive the peripheral airway resistance from the difference (R5-R20).
Objective To compare spirometry and IOS as tests of global airway function (i.e. FEV1, FEV1/FVC, R5) and putative measures of small airways function (i.e. FEF25–75, R5-R20) and their relationship to long-term asthma control.
Methods Spirometry and IOS measurements from asthmatics were linked to a health informatics database for oral steroid and short-acting beta agonist (SABA) use 1 year prior to the measurements.
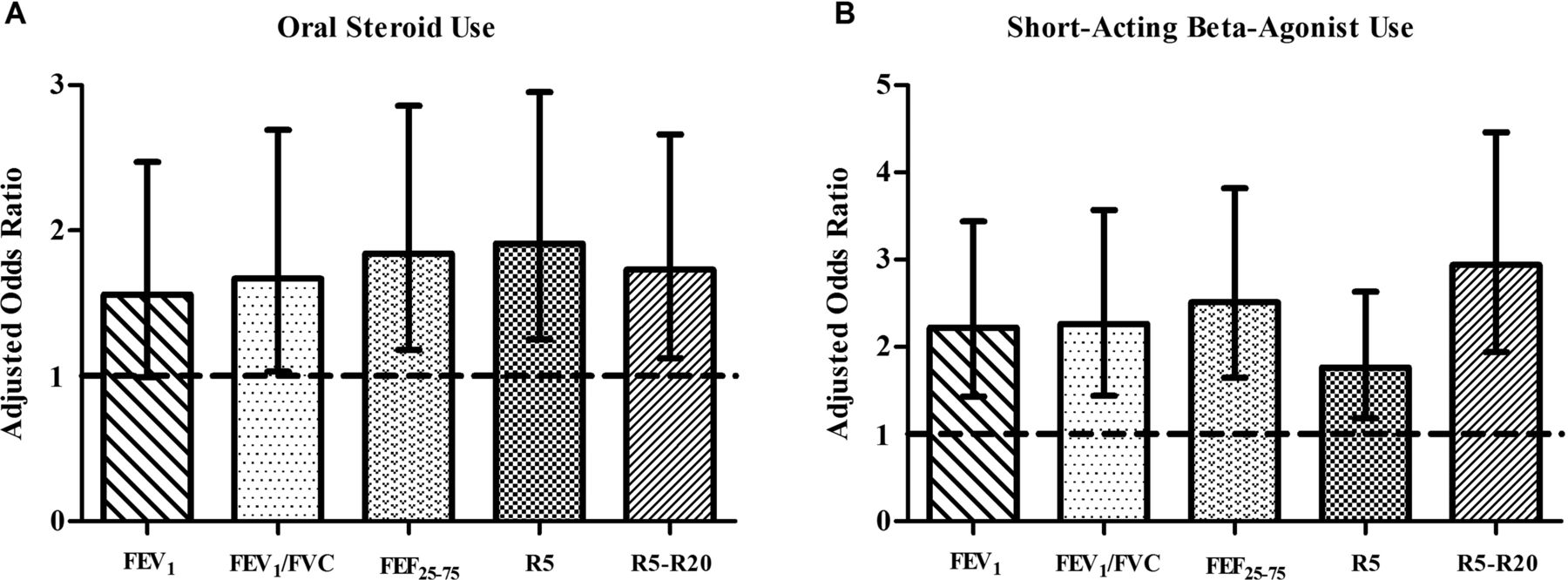
Results 442 patients had both spirometry and IOS, mean FEV1= 86% predicted, 94% on ICS, median dose 800 µg/day. IOS and spirometry measures were equally predictive of impaired asthma control for both oral steroid and SABA use. For oral steroid use, the adjusted odds ratio, OR (95% CI): FEV1 <80%: 1.56(0.99–2.47) p = 0.056, FEV1/FVC25–75 <60%: 1.84(1.18–2.86) p = 0.007, R5 >150%: 1.91(1.25–2.95) p = 0.003 and R5-R20 >0.1 kPa·L-1·s 1.73(1.12–2.66) p = 0.013. For SABA use, the adjusted OR (95% CI): FEV1 <80%: 2.22(1.43–3.44) p < 0.001, FEV1/FVC 25–75 <60%: 2.51(1.65–3.82) p < 0.001, R5 >150%: 1.76(1.18–2.63) p = 0.006 and R5-R20 >0.1 kPa·L-1·s: 2.94(1.94–4.46) p.
Conclusion Spirometry or IOS measurements are equally useful as potential markers of asthma control in persistent asthmatic patients.
{kind=link}
Adjusted odds ratios (95% CI) for oral steroid (A) and short-acting beta-agonist use (B) in the year preceding measurements of FEVi (<80% predicted, n = 140 vs >80% predicted, n = 302), FEV1/FVC (<0.70, n = 131 vs >0.70, n = 311), FEF25–75 (<60% predicted, n = 238 vs >60% predicted, n = 204), R5 (>150% predicted, n = 183 vs <150% predicted, n = 259) and R5-R20 (>0.10 kPa-L–1-s, n = 185 vs <0.10 kPa-L–1-s, n = 257). The 95% CIs which exclude unity are defined as being of statistical significance.