Article Text

Abstract
Purpose To evaluate the reliability of HRCT-parameters suggesting Pulmonary Hipertension (PH) in a population of Idiopathic Pulmonary Fibrosis (IPF) patients with or without PH at right-sided-heart-catheterization.
Methods and materials The HRCT scans of 26 patients with IPF, underwent both right-sided-heart-catheterization and echocardiography, were retrospectively, blindly and independently, evaluated by one radiology resident and one experienced-radiologist (with a 10-years-experience in thoracic-radiology).
The diameter and area of Pulmonary Artery (PA), before its bifurcation, the diameter of ascending aorta and the mid anteroposterior-diameter of the thoracic vertebra, on the same CT-section, and the widest short-axis-diameters of four segmental arteries and bronchus, in both upper and lower lobes, were measured. The diameters of left ventricle and inferior vena cava, the presence of emphisema, pericardial effusion and hiatal hernia were also evaluated.
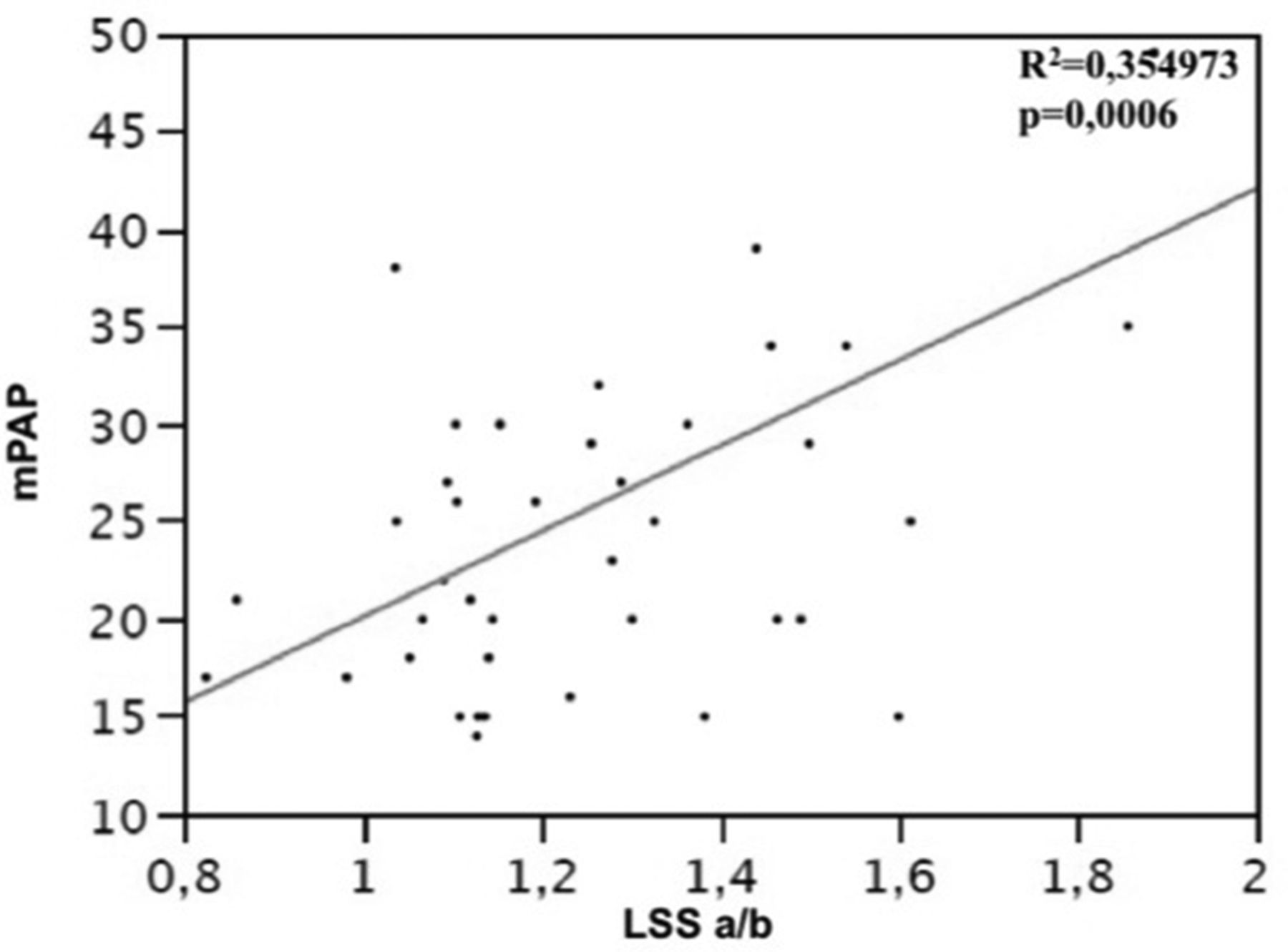
Results 15 out of 29 patients had PH at RHC. The HRCT parameters related to the mean pulmonary artery pressure (mPAP) were: the PA-area (R2=0.238079; p = 0.04), the ratio of the PA-area to the ascending aorta diameter (R2=0.215345; p = 0.0524) and above all the ratio of the diameter of segmental artery to the adjacent bronchus in the left upper lobe (R2=0.354973; p = 0.0006).
The combination of systolic pulmonary artery pressure (sPAP), the PA-area at HRCT and the ratio of the diameter of segmental artery to the adjacent bronchus in the apicoposterior segment of the left upper lobe was strongly correlated to mPAP (R2=0.785163; p = 0.0001). The contribution of other echocardiographic-parameters (longitudinal STRAIN and Time-to-Peak STRAIN values, TTP) in multivariate regression analysis was not statistically significant, probably because of the small number of patients.
Using the ROC Analysis we found that 931,6 is the upper limit of normal (ULN) for the PA-area, with a 86% sensitivity and 61% specificity (0.839 AUC); while 20.34 is the ULN for the ratio of the PA-area to the ascending aorta diameter, with a 100% sensitivity and 50% specificity (0.804 AUC).
Conclusion (S) HRCT remains an useful tool to identify patients with PH, however the combination of HRCT and echocardiograpy improves accuracy in PH diagnosis.
{kind=link}
Linear regression between mean puhnonary artery pressure measured by right heart catheterization (mPAP) and the ratio of the diameter of segmental artery to the adjacent bronchus of the apicoposterior segment of the left upper lobe