Article Text

Abstract
Introduction and objectives There is no agreed model for Pulmonary Rehabilitation (PR) and wide variation in services exists. A regional PR network was established 4 years ago, with the aim to drive up standards and reduce variation. An audit was undertaken of all PR services in the region to determine costs of services and factors influencing variance.
Method In June 2013 e-questionnaires were sent to all 16 known PR providers; fifty questions requested average annual/weekly data including: staff pay bands, time spent on exercise, education, administration, travel and other identifiable costs, numbers failing to complete (drop-out) and clinical outcomes. All costs were calculated in terms of cost-per-patient. Providers were assured actual costs and their identity would not be revealed.
Results
PR regionally serviced 3712 patients annually
Many providers total per patient costs were above the national tariff
Administration formed the highest share of providers total cost (24%),
Administration time per patient per course varied widely (1 – 14 h)
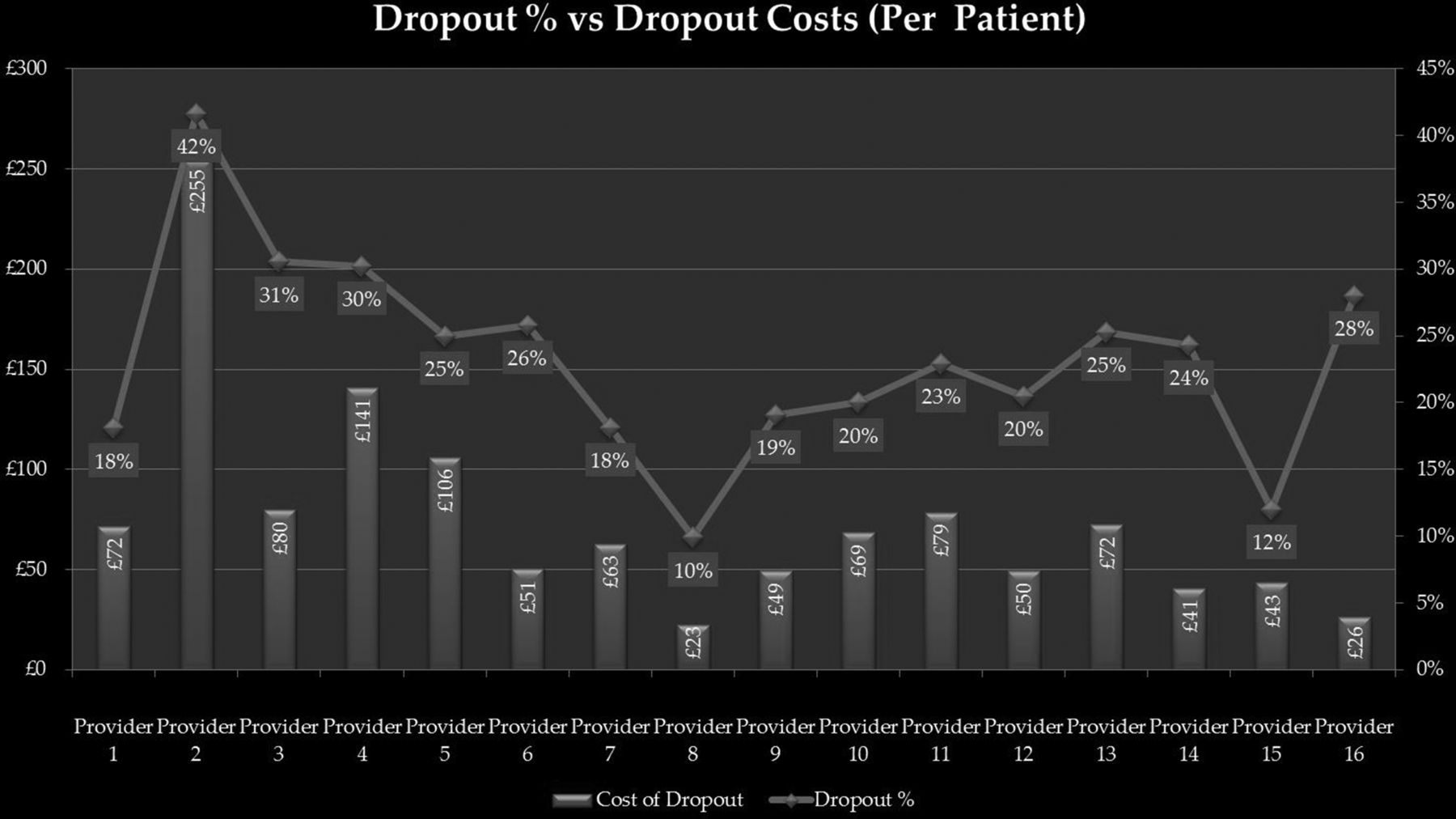
There was a wide range of drop-out, 10–42%, mean 23%
The mean (£76) and range (£23-£255) of drop-out cost per patient was high, rising at an ever increasing rate for every dropout (Figure)
Both larger patient numbers and rolling programmes were associated with higher per patient cost, the latter accountable to higher admin costs surpassing savings in exercise session costs.
Inconsistent reporting of clinical outcome data by providers.
Conclusion Our analysis demonstrates significant variation in the makeup of providers’ individual costs, with the majority of the variation between providers’ total cost per patient attributed to dropouts. Administration and drop-out were the greatest contributory factors to higher service costs. Higher cost was associated with larger patient numbers and rolling programmes.
Discussion Insufficient clinical outcome data were received to make any meaningful comparison of cost with outcome. Further work in this area is therefore required. Providers expected that providing services for larger numbers of patients and using rolling programmes would have lower costs, but the reverse was true. Administration costs for PR are very significant and may frequently be the key driver behind cost differences.
{kind=link}
Dropout% vs Dropout Costs (Per Patient)