Article Text

Abstract
Smoking is a major public health problem. As smokers age and die prematurely, the tobacco industry must continue to recruit new, young smokers. Survey data indicate that currently in the UK around 207 000 children aged 11–15 start smoking every year. We used local data on adult smoking rates to apportion national data on child smoking uptake to specific areas. The presentation of data for individual local authorities, which now have responsibility for public health, can be used to focus attention locally. For example, this analysis demonstrates that each day, 67 children, more than two classrooms full, start smoking in London.
- Tobacco and the lung
- Clinical Epidemiology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Background
Tobacco smoking is a major public health problem, even more so for smokers who start at a young age. Lung development is affected,1 ,2 meaning that subsequent decline in lung function starts from a lower base increasing the risk of COPD in later life. Moreover, people who start to smoke before the age of 15 have a higher risk of lung cancer than those who start later even after the amount smoked is taken into account.3
There is compelling evidence that young people are susceptible to branding and advertising and are influenced by the depiction of smoking in films.4 ,5 Legislation is needed to counter the efforts of the tobacco industry, but this requires political will by legislators at both national and local levels. This in turn depends on effective health advocacy.
National figures for smoking rates are available, but we propose that it would be useful to make available local estimates of smoking uptake among children. These could be used to help to focus attention and resources on what is essentially a child protection issue. In England, local authorities now have responsibility for public health and greater awareness of local burden should encourage them to give attention to implementation and enforcement of public health measures.
Methods
The initial analysis was based on data from the ‘Smoking, drinking and drug use among young people in England’ reports. This is an annual survey of secondary school pupils in England in years 7–11 (mostly aged 11–15) carried out for the Health and Social Care Information Centre. Questionnaires were completed by 6519 children in 219 schools during the Autumn term of 2011. By comparing rates of current smokers at each age with the smoking rates for that cohort surveyed in the year before, the number of new child smokers aged 11–15 could be estimated, giving a figure of 207 000 new smokers between 2010 and 2011 in the UK.6 Current smokers included both regular smokers (one or more cigarettes per week) and occasional smokers (less than one cigarette per week).
This UK estimate was then split across geographical areas according to their adult smoking prevalences, based on the assumption that there was likely to be a greater proportion of childhood smokers in areas that have more adult smokers, since parental smoking is one of the strongest predictors of smoking among children.7 ,8 This would provide a more valid estimate than simply dividing the national figure by the local population.
The adult (18 years and above) population for England, Wales, Scotland and Northern Ireland were collected from each country's relevant data authority. The smoking prevalence for each country was similarly retrieved and applied to the adult population to produce a total aggregated UK smoking population size. Local authority level data were used to get reliable estimates of smoking prevalence for England from The Office for National Statistics Integrated Household Survey (2011/12) and from the Statistics for Wales—Welsh Health Survey—smoking (2011). The total UK number of new child smokers was then apportioned according to the proportion of the total adult smoking population at a given locality. Further details of and links to the data sources used are available in an online supplement.
Results
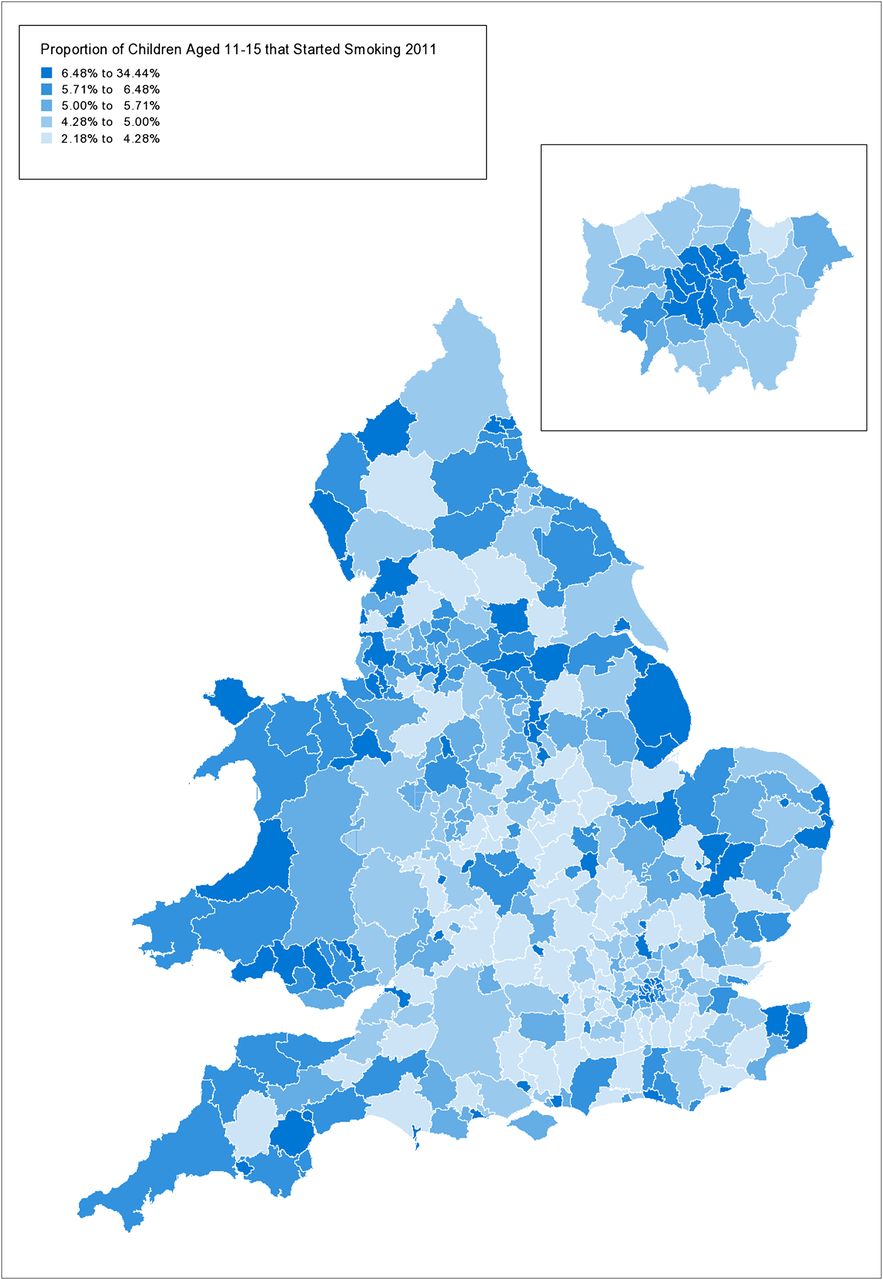
The estimated proportion of children aged 11–15 who started to smoke in 2011 are presented by location as a heat map in figure 1. Tables with daily, weekly, monthly and annual figures for each UK country (see online supplementary table S1) and for Local Authorities and Districts in England and Wales (see online supplementary table S2) are available online (http://dx.doi.org/10.1136/thoraxjnl-2013-204379). Of 3.7 million children aged 11–15 across the UK, an estimated 463 start to smoke daily in England, 55 in Scotland, 30 in Wales and 19 in Northern Ireland. In each Welsh region, a mean (SD) 10 (4.5) children start smoking each week, from a mean population of 8200. Of 74 000 children in Birmingham, 9 start to smoke daily; in London it is 67 from a population of 458 000.
{kind=link}
Estimate of proportion of children aged 11–15 who started smoking in England and Wales in 2011.
Discussion
Although the historical trend for smoking in both adults and children is downwards,6 the figure is still high and pressure needs to be maintained to ensure that the necessary public health measures are sustained and new initiatives are introduced to reduce it further. Measures that are recognised to be effective and need to be sustained include making tobacco less affordable by increasing taxation and reducing the illicit trade as well as continuing to run sustained, well-funded anti-smoking media campaigns. New measures include putting all cigarettes out of sight in all shops (due to be implemented in England in Spring 2015), the introduction of legislation for standardised packaging to reduce children's exposure to branding and the extension of smoke-free legislation to private vehicles. The banning of additives such as menthol which make cigarettes more palatable for children is also an important objective.
The data presented here are based on extrapolation from survey data and thus necessarily approximate. However, the availability of local estimates will enable pressure to be brought directly to bear on those with responsibility for developing and enforcing regulations in particular locations which may be more salient than a national figure.
Local authorities, which following the Health And Social Care Act (2012) now have responsibility for public health, should be encouraged to develop tobacco control policies and programmes designed to reduce local smoking prevalence and live up to their obligations under both the WHO Framework Convention on Tobacco Control Article 5.3 to protect their public health policies from the commercial and vested interests of the tobacco industry (http://www.who.int/fctc/guidelines/adopted/article_5_3/en/) and also the Tobacco Control Plan for England (https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/213757/dh_124960.pdf). Action on Smoking and Health (ASH) has developed the Challenge, Leadership and Results (CLeaR) standard for tobacco control, which was launched in July 2012 and as of August 2013, 89 out of around 150 upper tier authorities have signed up to it. The CLeaR standard is effectively a score card which local authorities can use to check whether their tobacco control policies live up to best practice (http://www.ash.org.uk/information/clear-excellence-in-local-tobacco-control).
Figures for child smoking uptake in specific areas may be useful when challenging members of parliament who have accepted hospitality, such as trips to Glyndebourne or The Chelsea Flower Show, from the tobacco industry.9
There are some limitations of the data presented. Although the Smoking Drinking and Drug Use Survey is relatively large with over 6000 respondents, the analysis is dependent on comparisons by age and sex and the sample sizes within these categories are clearly smaller. The analysis is also dependent on the publicly available data which have been rounded. Although rounding errors will, to some extent, cancel each other out this does add some uncertainty to the national-level estimate. A further limitation, specifically related to the local-level data, is that it is based on the assumption that smoking uptake by children is proportionate to adult smoking rates, since accurate local childhood smoking rates are not available. In addition, the estimates assume a constant ratio between adult and child population across the UK. However, the mean proportion of 11–15-year-olds to over 18s in England is 7.5% with a SD of 0.8%, so the spread is low and this is therefore unlikely to introduce significant bias (see online for data sources). Finally, although the data are presented at a UK level, this is based on an extrapolation of survey data from English children to the UK population.
In addition to this, while our figures are for under-16s, the age limit on buying tobacco products is 18. It is interesting to note that, although the Smoking Drinking and Drug Use in Young People Survey is collecting data for the 11–15 years age group, the national ambition for reduction in smoking prevalence in young people is for 15-year-olds and is to reduce smoking prevalence from 15% in 2009 to 12% or less by the end of 2015. This is problematic, as the data for 15-year-olds are based on small sample sizes and the CIs wide. Furthermore, there are also no robust data on smoking in 16-year-olds and 17-year-olds. This is a critical transitional period for smoking behaviour and falls below the legal age limit for buying tobacco products, so and it would be useful to have robust annual data on how many contemporary 16–17-year-olds are smoking, and how much.
Smoking is among the largest causes of preventable deaths worldwide. The present data should help to raise awareness of childhood smoking and to focus attention on the need to address this important child protection issue.
Supplementary materials
Press release
Files in this Data Supplement:
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
- Data supplement 2 - Online table 2
Footnotes
-
Contributors NSH and DA conceived the paper. NO-S and AC performed the initial analysis to obtain UK estimate. AL-G performed the analysis to produce local estimates. NSH wrote the first draft to which all authors subsequently contributed.
-
Funding The study was supported by the NIHR biomedical research unit at Royal Brompton and Harefield NHS Foundation Trust and Imperial College, London.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves