Article Text

Abstract
Our understanding of chronic obstructive pulmonary disease (COPD) has changed dramatically over the past two decades. We have moved from an airflow limitation-centric view to the realisation that COPD is a complex and heterogeneous disease, which leads inevitably to the need for personalising the assessment and treatment of patients with COPD. This review provides a brief perspective of the extraordinary transition that the COPD field has experienced in the last two decades, and speculates on how it should/can move forward in the near future in order to really achieve the goal of personalising COPD medicine in the clinic.
- COPD ÀÜ Mechanisms
- COPD Pharmacology
Statistics from Altmetric.com
Introduction
Our understanding of chronic obstructive pulmonary disease (COPD) has changed dramatically over the past two decades.1 We have moved from an airflow limitation (forced expiratory volume in 1 s, FEV1)-centric view of the disease2 to the realisation that COPD is a complex and heterogeneous condition.3 ,4 It is important to emphasise that, in this context, ‘complex’ means that COPD has a number of intrapulmonary and extrapulmonary components whose dynamic interactions along time are not linear, whereas ‘heterogeneous’ indicates that not all of these components are present in all individuals at any given time point.5 This realisation inevitably leads to the need for personalising the assessment and treatment of patients with COPD.1 ,5
The Global Strategy for the Diagnosis, Management and Prevention of COPD (GOLD) has already started to move in that direction.4 Since 2011, GOLD recommends a multidimensional assessment of patients with COPD that, while keeping the severity of airflow limitation (as determined by FEV1, percentage reference) still a core component of the proposal,2 includes two new dimensions: symptoms experienced by the patient and the risk of future exacerbations.4 This is because the relationship of FEV1 with these two important dimensions of the disease is weak.3 Instead, dyspnoea is a better prognostic indicator of mortality in COPD,6 and the previous history of exacerbations is the best surrogate marker of the risk of future exacerbations.7 Clearly, this is a step towards personalised medicine in the clinic (figure 1), but it is not likely to be the last one.5
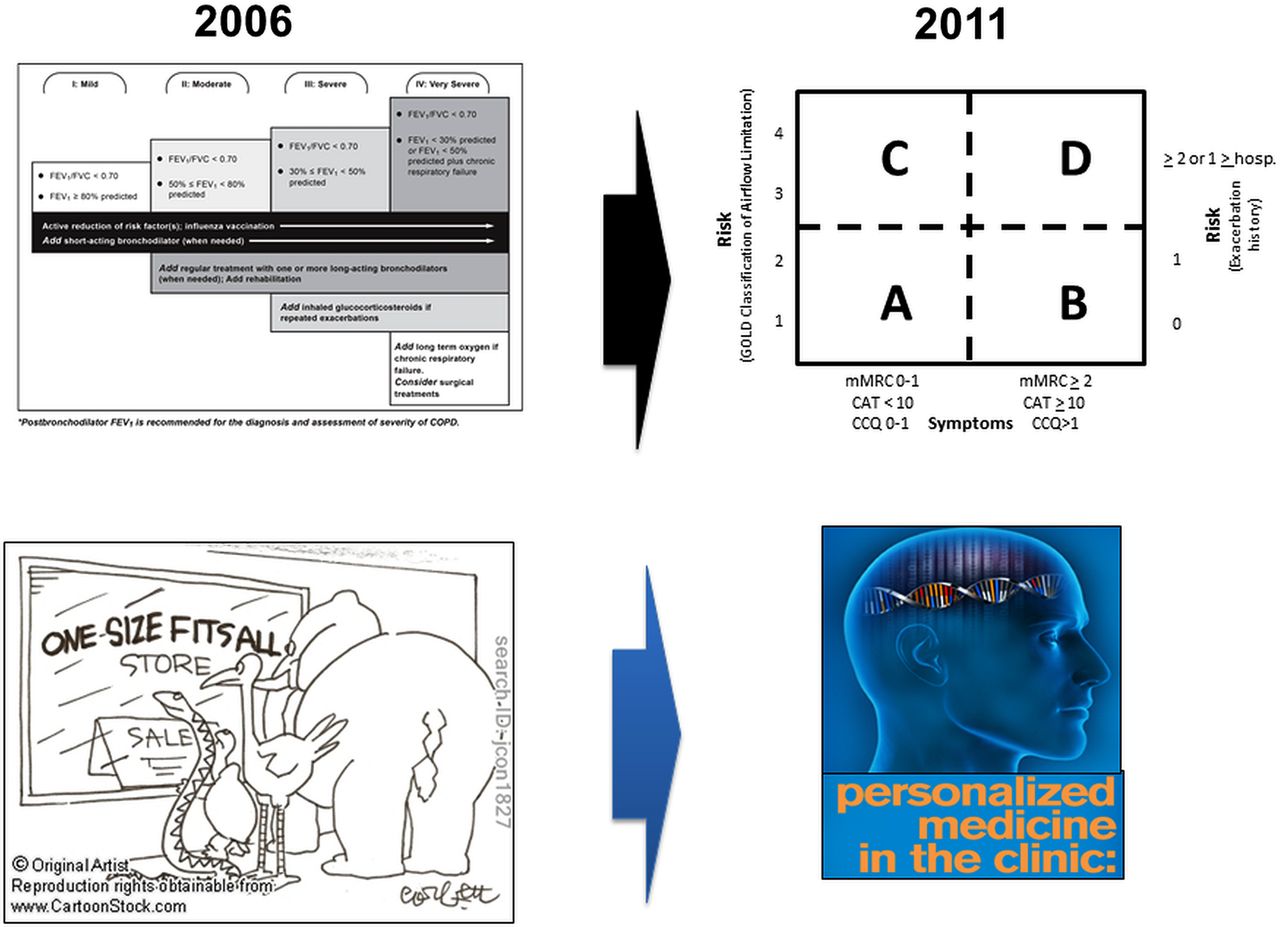
Pictorial representation of the important paradigm change proposed by GOLD at the end of 2011. The traditional (2006) assessment and treatment scheme for chronic obstructive pulmonary disease was centred almost exclusively on the severity of airflow limitation (as determined by the forced expiratory volume in 1 s (FEV1) value) whereas the new one (2011) is multidimensional. This represents the move from ‘one size fits all’ towards a personalised medicine approach in the clinic (bottom). For further explanation, see text.
This review provides a brief perspective of the extraordinary transition that the COPD field has experienced in the last two decades, and speculates on how it should/ can move forward in the near future in order to achieve the goal of really personalising COPD medicine in the clinic (figure 2).
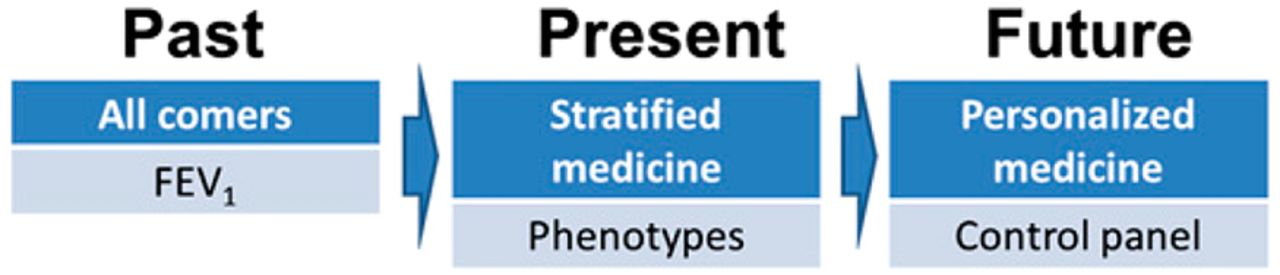
Temporal evolution of the understanding and management of chronic obstructive pulmonary disease. FEV1, forced expiratory volume in 1 s. For further explanation, see text. Reprinted with permission of the American Thoracic Society. Copyright © 2014 American Thoracic Society. Agusti A. Phenotypes and disease characterization in chronic obstructive pulmonary disease. Toward the extinction of phenotypes? Ann Am Thorac Soc 2013;10:S125–30. Official Journal of the American Thoracic Society.
The COPD Stone Age: an FEV1-centric view
It was only 15–20 years ago, ‘yesterday’ in historical terms, when COPD was basically a neglected, almost orphan,8 disease. At that time, COPD was viewed as a self-inflicted disease for which basically nothing could be done other than persuading the patient to quit smoking and use some short-acting bronchodilators and/or theophylline, which were frequently associated with significant side effects. Available treatment was basically ‘inherited’ from asthma, which at that time clearly dominated the respiratory scientific scene.9 This landscape began to change in 2001 when the first GOLD document was released.10 This initiative of the Heart, Lung, and Blood Institute and the WHO has had a profound effect in the field. According to its initial declaration, its objectives were ‘to increase awareness of COPD and to help patients suffering this disease and dying prematurely from it or its complications’.10 It certainly achieved these goals, since GOLD has contributed extraordinarily to the rise in awareness of the prevalence and burden of the disease.11 Yet, in the context of this paper, it should be noted that both this first GOLD document10 as well as the first revision released in 20062 were FEV1-centric, since the degree of airflow limitation present was central for the diagnosis, assessment and treatment of COPD.
The COPD Renaissance: complexity, phenotypes and stratified medicine
A second major change in the field of COPD occurred in November 2011 when the third revision of the GOLD document was released.4 This change was fuelled by the realisation that COPD was a complex and heterogeneous disease with a number of intrapulmonary and extrapulmonary components,12 ,13 and that FEV1 had a weak relationship with them.3 In other words, FEV1 was a necessary but insufficient parameter to characterise the complexity and severity of COPD and to guide its treatment.14 ,15 Following from this, GOLD 2011 proposed a three-dimensional assessment of COPD which, while still considering the severity of airflow limitation (eg, FEV1), also includes the level of symptoms experienced by the patient and the previous history of exacerbations to predict the risk of future exacerbations.4 This proposal was, however, by and large not based on evidence but rather on ‘expert opinion’. It is not surprising, therefore, that many questions arose after its publication16 since, according to Niels Bohr (Copenhagen, Denmark, 1885–1962), “an expert is a person who has made all the mistakes that can be made in a very narrow field”.17
On the other hand, in order to deal with the complexity of COPD, the investigation of COPD ‘phenotypes’ became very popular.18–20 The term phenotype classically refers to ‘any observed quality of an organism, such as its morphology, development or behaviour’, as opposed to its genotype—the inherited instructions it carries, which may or may not be expressed.21 The phenotype is composed of traits or characteristics, some of which are controlled entirely by the individual’s genes whereas others are controlled by genes but are significantly affected by environmental factors.21 This definition is hard to apply to clinical medicine since some phenotypes so defined may be completely irrelevant for the disease process of interest. In 2010, another group of experts therefore proposed the concept of a ‘clinical COPD phenotype’ as ‘a single or combination of disease attributes that describe differences between individuals with COPD as they relate to clinically meaningful outcomes (symptoms, exacerbations, response to therapy, rate of disease progression, or death)’.22 This intellectual process is depicted graphically in figure 3. Because COPD is a heterogeneous disease (as represented by the different colours in figure 3A), the concept of a clinical phenotype attempted to provide some order by grouping patients with similar clinically relevant characteristics (figure 3B). However, in real life, patients with COPD are not only heterogeneous but also complex, indicating that different clinical characteristics can occur in varying proportions in any given patient (figure 3C). Therefore, although the concept of a clinical phenotype is useful for research in order to understand the heterogeneity of the disease, it is of limited use in clinical practice, which deals with individual patients (personalised medicine) and not with groups of patients classified according to a particular clinical phenotype (stratified medicine) (figure 2).5

Cartoon representation of complexity and potential alternatives for assessment and management of chronic obstructive pulmonary disease (COPD). Each node represents one theoretical patient and each colour represents one clinical characteristic. For further explanation, see text.
The COPD future: personalised (P4) medicine
Niels Bohr also said: “It's difficult to make predictions, especially about the future”.23 In the context of this paper, however, it is hard to fail if the prediction is that the future of COPD (and medicine in general) is to become more ‘personalised’. Of note, personalised medicine is not exactly the same as ‘individualised’ medicine (M Perpiña, Valencia, Spain; personal communication). Fortunately, the practice of medicine has been ‘individualised’ for the last 2000–3000 years at least.5 The term ‘personalised’ medicine goes beyond that of ‘individualised’ medicine since it pretends that, based on the individual's genome (personalised), predictions about future risks can be made and, accordingly, preventive strategies can be implemented, most often requiring the participation of the patient. This is why ‘personalised medicine’ is also known as ‘P4 medicine’.1 ,24
So the real question is not where we are heading (P4 medicine) but how we are going to get there. To help us think about this, a number of domains and characteristics of COPD that may be clinically relevant (ie, may eventually become therapeutic targets) but are not currently included in the GOLD recommendations are discussed below,4 as well as a potential way to integrate these different actionable (ie, treatable) domains into clinical practice (the COPD control panel), as proposed recently.25
What are we currently missing?
I have no doubt that the new GOLD multidimensional assessment proposal4 marks a point of no return in our understanding and management of COPD (figure 1). However, ‘transformation is a process, not an event’,26 so there is no reason to believe that the current proposal is the end of the story. Rather, it is likely to be the beginning of a transformative process. Hence, it is legitimate to ask what other domains of the disease will probably have to be incorporated to evolve, improve and refine the current situation. Box 1 presents some of them. The list does not pretend to be exhaustive and is only presented to stimulate the scientific debate. Comorbidities, which are highly prevalent in patients with COPD,3 ,27 are not discussed here since they are repeatedly discussed in the current GOLD document.4
Box 1 Clinically relevant domains to potentially consider in the future management of chronic obstructive pulmonary disease
-
Inflammation
-
Pulmonary
-
Systemic
-
-
Lung microbiome
-
Disease activity
-
Imaging
-
Emphysema
-
Lung cancer
-
Bronchiectasis
-
Molecular imaging
-
-
Others (open for suggestions and debate!)
COPD is ‘a common preventable and treatable disease, characterised by persistent airflow limitation that is usually progressive and associated with an enhanced chronic inflammatory response in the airways and the lung to noxious particles or gases’.4 Despite the fact that this definition refers to the chronic inflammatory process that characterises the disease, both in the lungs28 and the systemic circulation,29 no specific recommendations are made on how to measure and monitor it and/or what therapeutic alternatives should be used based on the assessment of this abnormal inflammatory response. Yet, some recent reports are beginning to pave the way towards the use of inflammatory markers in the management of COPD. For instance, the systemic inflammome associated with both smoking and COPD has recently been described (figure 4).30 Importantly, the results showed that, contrary to established beliefs,29 not all patients with COPD have persistent systemic inflammation (in fact, about a third of them appear to be persistently non-inflamed30) and that, despite having similar FEV1 values, patients with persistent inflammation had more frequent exacerbations and a six times higher mortality during 3 years of follow-up than patients without inflammation.30 These results have now been reproduced in other cohorts31 and, more importantly, ‘inflammometry’ has now been used in pilot studies to guide therapy in COPD with very encouraging results.32 ,33 It is therefore conceivable that, somehow, inflammatory markers will sooner or later be included in the routine management of patients with COPD.

The systemic inflammome of smoking and chronic obstructive pulmonary disease (COPD). Each node represents one circulating inflammatory biomarkers (as per the colour code shown in the slide), whose diameter is proportional to the number of subjects in each group (non-smokers, smokers with normal spirometry and patients with COPD) with abnormal values of that particular biomarker. Nodes are connected if participants present abnormal values of both biomarkers, the width of the link being proportional to the number of subjects in that group with abnormal values of the two linked biomarkers (as indicated in the figure). For further explanation, see text. Reproduced from Agusti et al.30
Chronic airway ‘colonisation’ is known to occur in some patients with otherwise clinically stable COPD.34–36 It is likely to impact negatively on their clinical course by increasing the symptoms (chronic cough and expectoration), accelerating their rate of FEV1 decline and/or promoting the occurrence of exacerbations.37 ,38 Yet again, current recommendations do not mention when and how this should be diagnosed, monitored or treated. Even more importantly, the old dogma that the healthy human lung is sterile is wrong.39 The use of modern molecular techniques rather than the old culture-based methods has opened a new frontier in respiratory medicine40 by showing that even healthy lungs display a complex ‘microbiome’, and that this changes in many diseases including COPD.41–49 The influence of changes in the lung microbiome of patients with COPD (either spontaneous or induced by treatment) on clinically relevant domains of the disease such as symptoms, exacerbations, rate of FEV1 decline, predisposition to lung cancer and/or relationship with pulmonary and systemic inflammation, as discussed above, will have to be investigated and eventually included in the clinical assessment and management of these patients.
A third domain that will probably need to be considered in the future is that of ‘disease activity’.50 This concept refers to the ‘level of activation of the biological processes that drive disease progression’.51 It is well established in other chronic diseases, such as rheumatoid arthritis, where it is clearly differentiated from that of ‘severity’ of the disease (ie, the extent of functional loss of the target organ(s)), that of ‘early versus late’ disease (ie, the time point in the natural history of a disease at which it is diagnosed or studied) and/or that of the ‘impact’ of the disease on the patient (ie, health status).51 Despite its clear importance in order to guide therapy,50 there is no consensus yet on what marker(s) should be used to evaluate and monitor disease activity in COPD. Some recent reports have suggested that the presence of eosinophils is a controllable aspect of the disease which is present in some patients with COPD.32 ,52–55 Further, some clinical surrogates can be conceived. First, now we know that—again contrary to the established dogma56—not all patients with COPD have an accelerated decline of lung function with time,57 it is conceivable that those with it have more ‘active’ disease than those without it (table 1). Similarly, it is conceivable that patients with frequent exacerbations also have more ‘active’ disease than those without exacerbations.7 In any case, the investigation of disease activity biomarkers is clearly one of the areas that can contribute more to personalise medicine in patients with COPD in the near future.
Another aspect of COPD which is currently neglected in the routine clinical management of these patients, despite cumulative evidence of its potential importance, is the rapidly evolving field of thoracic imaging (table 1) including low-dose CT scanners, positron emission tomography and other techniques of molecular imaging.58–60 Whether or not the routine management of patients with COPD should involve this sort of imaging technique is currently unclear. However, as an example, a single CT scan can provide information on the presence of emphysema,61 lung cancer,62 bronchiectasis63 and coronary artery calcification,64 as well as others such as pulmonary emboli, column osteoporosis and pectoralis muscle mass. All of them are clinically relevant and potentially actionable (ie, treatable). For instance, the identification of emphysema or lung cancer may be relevant per se but, more importantly, because of their often ignored inter-relationship. In this context, it is well established that tobacco smoking is the major risk factor for both COPD and lung cancer, even though not all smokers develop these diseases. What is often less appreciated, however, is that the risk of lung cancer is significantly higher in smokers who have developed COPD, particularly emphysema.65 In fact, it is exceptional to see a patient with lung cancer and normal spirometry. Given that survival in patients with lung cancer is directly related to early diagnosis,66 it is possible that a greater awareness of lung cancer risk in patients with COPD might have a significant clinical impact.67 Unfortunately, few physicians today think about lung cancer risk in front of a patient with COPD, despite the fact that other surrogates of emphysema (such as carbon monoxide transfer factor) appear also to predict the risk of lung cancer in patients with COPD.65 Intervention to reduce the incidence of lung cancer in patients with COPD (eg, chemoprevention or screening) should be intensively investigated. Likewise, bronchiectasis is prevalent in patients with COPD68–70 and, importantly, it appears to be significantly associated with an increased risk of mortality.63 Yet, whether this should be investigated routinely in all patients with COPD, how to do this and what to do if it is found is not currently considered. Furthermore, the relationship between bronchiectasis identified clinically or by imaging and the lung microbiome, as discussed above, is currently unclear. The identification of coronary artery calcification in these patients64 may also be clinically relevant, given the high prevalence of cardiovascular disease in COPD.71 Finally, the development of molecular imaging techniques may facilitate the diagnosis and monitoring of pulmonary inflammation, changes in the microbiome and/or early diagnosis of lung cancer in COPD,58 ,59 a disease component that, as discussed above, is currently ignored.
How can we put all this together?
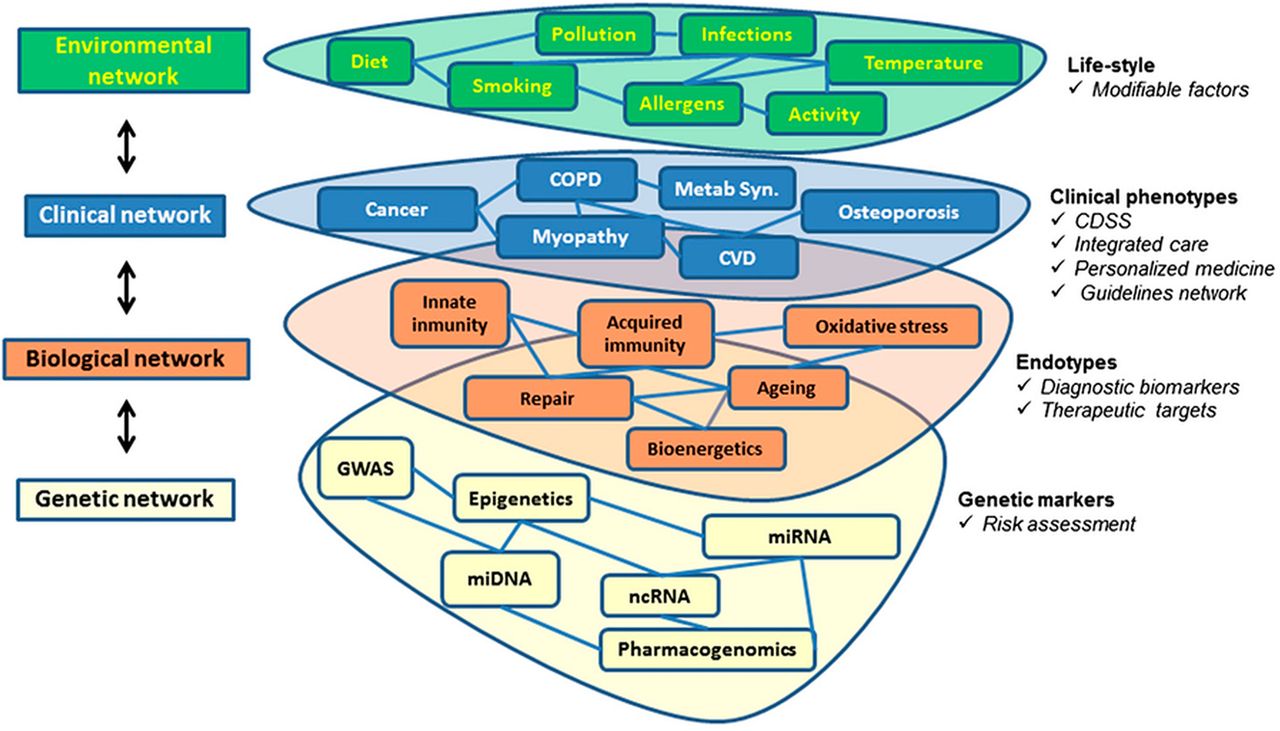
In my opinion, the answer to this question requires the consideration of two different aspects. First, the integration of multiple levels of data (environmental, clinical, biological and genetic) using network science.1 ,72–74 As shown in figure 5, this approach has the potential to deliver clinically relevant outcomes from each of these four levels,72 including the identification of genetic markers that facilitate the assessment of risk of future events (lung function decline, exacerbations, comorbidities), biomarker validation and new therapeutic targets identification, clinical decision support systems (CDSS) and other integrated care tools, and lifestyle changes, all of which are important in the prevention and treatment, of chronic diseases like COPD.75
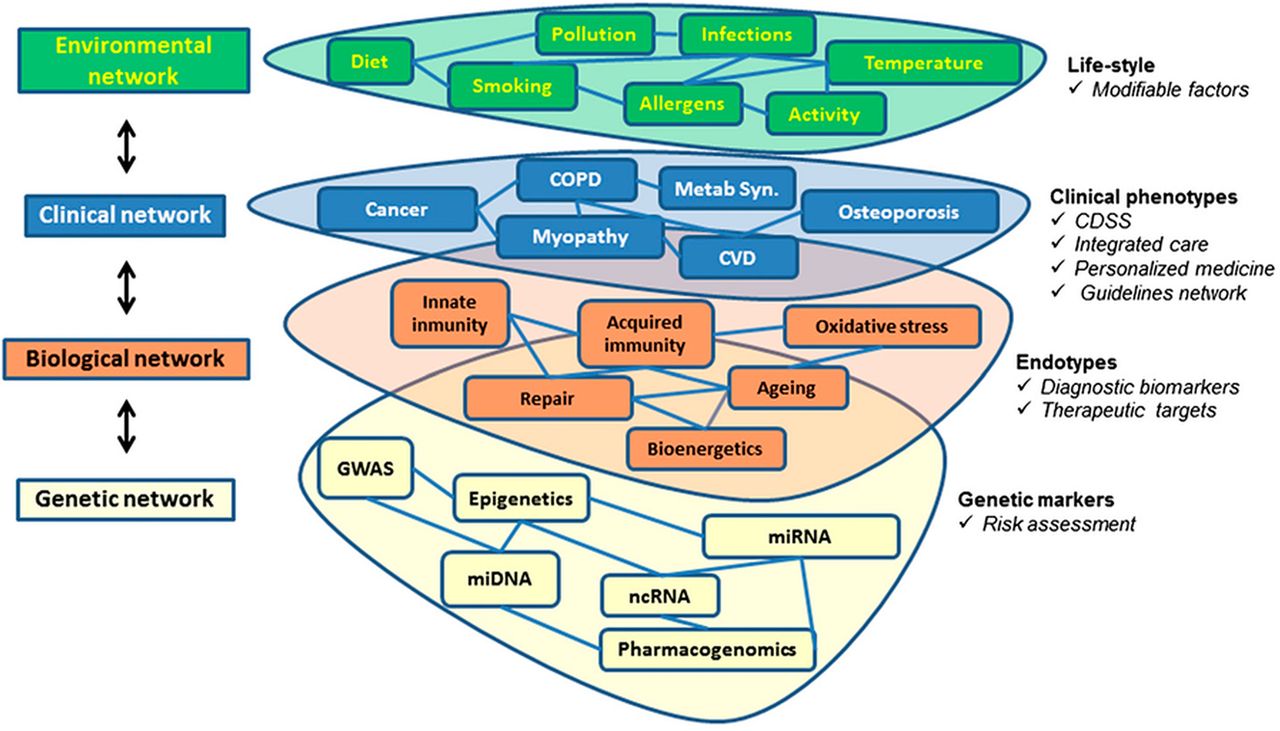
Multilevel (environmental, clinical, biological and genetic) network approach to chronic obstructive pulmonary disease (COPD) complexity. On the right is a list of potential outcomes from each level of potential usefulness for a COPD personalised approach. For further explanation, see text. Reprinted with permission of the American Thoracic Society. Copyright © 2014 American Thoracic Society. Cite: Agusti A, Vestbo J. Current controversies and future perspectives in chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2011;184:507–13. Official Journal of the American Thoracic Society.
The second aspect has to do with the best way to implement all this new information in real clinical practice. If the current three-domain assessment system proposed by GOLD4 has already been criticised because of its complexity,76 needless to say a much more complex system like the one proposed here may not be well received. Yet the answer is not difficult and may come from other fields such as engineering. Using the analogy of aeroplane pilots who, in order to fly the plane safely, need to receive multidimensional information (eg, altitude, route, weather conditions, fuel reserve, potential incoming aircraft), we have recently proposed that a similar ‘control panel’ can provide physicians with the actionable information necessary for the best personalised treatment of a given patient.25 In essence, this would be a sort of validated CDSS that, importantly, can be customised to make it simpler or more complex depending on the local practice circumstances (eg, primary vs specialised care). The original COPD control panel proposal25 included three modules (severity, activity and impact), each of them including a number of related and actionable variables. Of course this proposal is only conceptual and has not been adequately validated, so the specific content of each module requires research. However, we believe that the concept is valid in order to progress to COPD personalised medicine in clinical practice. Yet again this is an evolving concept. For instance, a very recent prespecified analysis in 5125 patients with COPD included in the Prevention Of Exacerbations with Tiotropium in COPD (POET-COPD) trial77 showed that polymorphisms of the β2-adrenergic receptor (ADRB2) gene (Arg16Gly (rs1042713) and Gln27Glu (rs1042714)) did indeed influence the effect of long-acting bronchodilators (tiotropium vs salmeterol) in the prevention of exacerbations.78 This is therefore a good example of pharmacogenetic testing being considered in the personalised treatment of COPD and, in my opinion, it paves the way towards the future incorporation of a fourth ‘omics’ module in a refined COPD control panel (figure 6).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Chronic obstructive pulmonary disease control panel for personalised medicine in the clinic. Each of the three modules (severity, activity and impact) provides information on an actionable (ie, treatable) component of the disease. CAT, COPD Assessment Test; FEV1, forced expiratory volume in 1 s; IC, inspiratory capacity; mMRC, modified Medical Research Council dyspnoea score; 6MWD, 6 min walk distance; Pao2, arterial oxygen tension; TLC, total lung capacity. For further explanation, see text. Reproduced with permission from Agusti and MacNee.25
Conclusions
This review attempts to convey some (personal) perspective to the extraordinary series of changes that have occurred in the field of COPD over the last two decades or less, where we have been liberated by moving away from an FEV1-centric view of the disease to one which also considers clinically relevant domains of the disease such as the level of current symptoms and the history of previous exacerbations.4 It is proposed, however, that the future of COPD will inevitably become even more personalised, and a series of components of the disease that may provide additional, independent and clinically useful information for a better management of patients with COPD are discussed. Finally, it is suggested that a COPD control panel seems an appropriate CDSS that can be tailored to different clinical conditions and needs. All in all, this approach might help to sort out the differential diagnostic of airflow limitation due to other chronic respiratory diseases and/or ageing79 to facilitate the development of novel therapeutic drugs by recruiting discrete subgroups of patients with COPD into clinical trials80 and, eventually, to manage COPD more efficiently.33
Acknowledgments
This review is the result of many previous discussions with colleagues and friends in the field, to whom I am grateful. Discussions finally crystalised into this paper during a visit to Tokyo (Japan) in March 2014. I want to thank my family (my wife in particular) for allowing me the time required for these activities.
References
Footnotes
-
Funding ISCiii PI041966/2012 and PI10/00523
-
Competing interests AA is a member of the Scientific Committee and Board of GOLD.
-
Provenance and peer review Not commissioned; internally peer reviewed.
Linked Articles
- Airwaves