Article Text

Abstract
Background The BCG vaccine's ability to prevent Mycobacterium tuberculosis infection (MTI) remains highly debated. In Greenland, BCG vaccination was introduced in 1955, but was temporarily discontinued (1991–1996) due to nationwide policy changes. The study aimed to use the transient stop in BCG vaccination to evaluate the effect of vaccination on MTI prevalence and TB incidence.
Methods MTI study: A cross-sectional study (2012), comprising East Greenlanders born during 1982–2006, evaluated the effect of BCG vaccination on MTI prevalence; a positive interferon γ release assay defined an MTI case. Associations were estimated using logistic regression. TB study: a cohort study covering the same birth cohorts with follow-up until 2012 evaluated the vaccine's effect on TB incidence. A personal identifier allowed for follow-up in the TB notification system. Associations were estimated using Cox regression.
Results MTI study: Included 953 participants; 81% were BCG-vaccinated; 29% had MTI, 23% among vaccinated and 57% among non-vaccinated. BCG vaccination reduced the odds of MTI, OR 0.52 (95% CI 0.32 to 0.85), p=0.01. Vaccine effectiveness against MTI was 20%. TB study: Included 1697 participants followed for 21 148 person-years. 6% were notified with TB, 4% among vaccinated and 11% among non-vaccinated. BCG vaccination reduced the risk of TB, HR 0.50 (95% CI 0.26 to 0.95), p=0.03, yielding a vaccine effectiveness of 50%.
Conclusions BCG vaccination was effective in reducing both MTI and TB disease among children and young adults in a TB high-endemic setting in Greenland.
- Tuberculosis
- Clinical Epidemiology
- Infection Control
Statistics from Altmetric.com
Key messages
What is the key question?
-
What is the effect of BCG vaccination on Mycobacterium tuberculosis infection (MTI) and TB disease among children and young adults in a TB high-endemic setting?
What is the bottom line?
-
We report a significantly lower MTI prevalence and TB incidence among BCG-vaccinated individuals.
Why read on?
-
The effectiveness of BCG vaccination in preventing MTI is highly debated; in Greenland, nationwide policy changes, first to stop and then subsequently reintroduce BCG vaccination, provided us with an ideal controlled TB research environment to study the effect of the BCG vaccination against both MTI and TB.
Introduction
The BCG vaccine remains the only licensed vaccine against TB, with an estimated global coverage of 85%.1 ,2
The protective effect of BCG vaccination has been extensively investigated and is well documented for disseminated TB and TB meningitis in children whereas the protective effect against pulmonary TB ranges from partial to good long-lasting protection.3–6 New and emerging data show that BCG vaccination may also protect against Mycobacterium tuberculosis infection (MTI); however, this is highly debated.1 ,7–12
The heterogeneity in vaccine effectiveness (VE) is a result of several influential factors, including characteristics of the host and the environment.1 ,2 Studies have documented decreased BCG VE among individuals with HIV and other immune deficiencies.2 Also a high level of environmental non-tuberculous mycobacteria (NTM) seems to decrease effectiveness.5 ,13
Since the 1990s, Greenland has experienced a continuously high TB incidence reaching 157/100 000 inhabitants in 2012; currently, East Greenland is experiencing an ongoing epidemic.14–16 In contrast to other high TB-endemic settings, the incidence of HIV and of multi-drug resistant TB is low in Greenland,14 ,17 and the Arctic climate diminishes the occurrence of NTM to an almost non-existing level.18
In 1955, neonatal BCG vaccination was introduced in the Greenlandic national childhood vaccination programme. Due to a marked reduction in TB incidence from 1970 to 1990, BCG vaccination was completely stopped in 1991. Following cases of TB meningitis in children and an increase in TB incidence, BCG vaccination was re-introduced in 1997. When BCG vaccination was part of the vaccination programme, the BCG vaccine coverage exceeded 93%.19 No catch-up vaccination was offered to the unvaccinated birth cohorts.20 ,21
The study aim was to use the transient stop in BCG vaccination for evaluating the effect of BCG vaccination on MTI and TB in a TB high-endemic setting.
Methods
Setting
Greenland is an integral part of the Kingdom of Denmark, but is governed by the Greenland Self-Government. The population is wealthy by the standards of developing countries and has universal and free access to healthcare including TB treatment. The studies were performed in the East Greenlandic district of Tasiilaq with 2957 inhabitants, corresponding to 87% of the East Greenlandic population and 5% of the total Greenlandic population.22 The majority of the Greenlandic population is Inuit (89%).22
National registers
All live-born children and new residents in Greenland are assigned a unique personal identifier through the Civil Registration System (CRS).23 The identifier allows follow-up of individuals through all national registers and provides information on, for example, birth place, sex, date of birth and place of residence. Linkage to the national birth register, the TB notification system and the school registers was done using the CRS identifier. To be categorised as Inuit, both parents should be registered as born in Greenland. Since 1955, TB has been mandatory notifiable in Greenland and cases are notified to the National Board of Health in Greenland. Schooling (age 6–16) is mandatory, and all children are registered in the local school registers.
BCG vaccination
In Greenland, the national childhood vaccination programme is voluntary and free of charge and has included the BCG vaccine since 1955, except for a temporary discontinuation from 1991 to 1996. The BCG vaccine is administered intradermally to neonates (0.05 mL live attenuated vaccine Mycobacterium bovis BCG (Danish strain 1331)).20 ,21 From 1955, information on vaccination status has been kept locally in medical records, and from 2001, centrally in the national birth register. We assumed all individuals born in Greenland from 1 January 1991 to 31 December 1996 to be non-vaccinated. Information on BCG vaccination for participants in the MTI study (see Study designs section below) was reviewed for 842 of 953 participants (88%). Adequate information was present for 680 (81%) and of these 99% followed the national BCG vaccination policy, which supported our assumption.
Study designs
To evaluate the effect of BCG vaccination on the prevalence of MTI, we designed a cross-sectional study (The MTI study). To evaluate the effect of BCG vaccination on the incidence of TB, we designed a register-based cohort study (The TB study).
The MTI study
This was a cross-sectional study designed to assess the prevalence of MTI. The study population included the birth cohorts from 1982 to 2006 (age 5–30), living in the Tasiilaq district in 2012. All eligible inhabitants were identified through the CRS and the local school registers. Due to frequent migration, all non-responders were conferred with the local authorities to confirm residency. At study start, September 2012, 1197 participants were resident and were invited to participate. One week in advance, the participants received a personal letter of invitation, study information and a consent form. When possible, participants were also contacted by phone. On predefined dates, from September 2012 to April 2013, study staff assessed the participants at schools, the district hospital or at health clinics.
MTI was assessed using the interferon γ release assay (IGRA), QuantiFERON-TB Gold test (QFT).24 ,25 All tests were analysed at Statens Serum Institut, Denmark, following the instructions of the manufacturer.25 MTI was defined as having a positive QFT, regardless of clinical status, treatment status and prior testing.
The TB study
This was a cohort study, based exclusively on data from national registers, and designed to assess the incidence of TB. All individuals born in the Tasiilaq district from 1982 to 2006 were included. Follow-up was from time of birth until the first of the following events: first record of TB, emigration from the district, death or end of follow-up (31 December 2012). By linking the personal identifiers of individuals in the cohort with the TB notification system, all TB cases were obtained. A case of TB was defined using national Greenlandic case definitions which follow WHO case definitions.21 ,26 The different regions of Greenland have experienced different secular trends in M. tuberculosis exposure.14–16 For comparison, we therefore designed an additional register-based cohort, including the same birth cohorts for Greenland excluding East Greenland.
Statistical analysis
In the cross-sectional study, logistic regression was used to estimate the association between BCG and MTI, with ORs as effect measure. All ORs were adjusted for sex, age and ethnicity (Inuit/non-Inuit) with age modelled as a cubic spline with four degrees of freedom with knots at the 25% (age 10), 50% (14 years) and 75% (age 21) quartiles. BCG vaccination status is defined by birth cohort and is therefore correlated to age in the cross-sectional study. Thus, the age-adjusted BCG effect should be interpreted as the deviation from the smoothed age effect. The estimation of the BCG effect is based on the assumption that the age effect among non-vaccinated is sufficiently captured in the above way. The predicted MTI prevalence was also estimated using the above model but without the effect of sex and ethnicity. Differences between participants and non-participants were evaluated for BCG and TB (as a proxy for MTI) stratified by age with Fisher's exact test to address potential selection bias.
In the cohort study, Cox regression was used to estimate the association between BCG and TB with age as underlying time scale and HR as effect measure. The proportional hazard assumption was evaluated by a test based on the scaled Schoenfeld residuals; these were not fulfilled for the covariate sex and therefore the adjusted analysis was stratified by sex. In addition, the adjusted analysis was adjusted for time of birth using a cubic spline with two degrees of freedom with knots at the median (1994). The time of birth-adjusted BCG effect is interpretable in the same manner as described above for the cross-sectional study. We tested for effect modification by age (<15, ≥15 years of age) by including an interaction term in the regression analysis. The cumulative risk of TB by BCG vaccination and age was estimated as one minus the Kaplan–Meier estimator of the survival function.
VE for TB (VETB) was calculated as VETB=1 − HR, with HR taken from the Cox regression analysis of the cohort data. VE for MTI (VEMTI) was calculated as VEMTI=1 − RR, with RR (risk ratio) estimated in the cross-sectional data using log-linear binomial regression (analysis performed as the logistic regression except that the log-link is used instead of the logit-link). The RR from the cross-sectional study was used to approximate the rate ratio in the underlying cohort. Assuming non-differential misclassification of MTI, the VEMTI was estimated with and without correction for misclassification; the crude RR corrected for misclassification was estimated by a matrix adjustment method.27 All tests and 95% CIs were based on Wald statistics. Analyses were performed using the R software.
Ethical considerations
The studies fulfilled the Helsinki Declaration II. Written and informed consent was given by all participants and by parents or legal guardians of children <age 18 years. Child acquiescence was required for children <age 18 years. All participants with a positive QFT were referred to the district hospital for further evaluation. The Commission for Scientific Research in Greenland (approval No. 2012-4) and the Danish Data Protection Agency approved the studies.
Results
The MTI study
Of 1197 invited, 953 participants were enrolled and tested for MTI (all QFT were conclusive), yielding an overall participation rate of 80% (91% among schoolchildren, 67% among young adults). In total, the study population included 1.7% of the total population in Greenland.22 Demographic information for participants is shown in table 1. Neither BCG vaccination nor TB status was associated with participation after stratification for age.
Demographic characteristics of 953 children and young adults in East Greenland examined for Mycobacterium tuberculosis infection (MTI)
Overall, 280 (29%) of the participants had MTI: 103 (57%) among the non-vaccinated and 177 (23%) among vaccinated. Figure 1A shows the observed age-specific MTI prevalence and indicates increased MTI prevalence among the non-vaccinated participants (age 16–21). Figure 1B illustrates the higher prevalence among non-vaccinated participants by modelling the age-specific prevalence for vaccinated versus non-vaccinated participants. Table 2 shows the estimated ORs for the association between BCG vaccination and MTI prevalence. In the adjusted analysis, BCG vaccination was significantly associated with lower risk of MTI, OR 0.52 (95% CI 0.32 to 0.85), p=0.01. Based on these cross-sectional data, the BCG VEMTI was 20%. Assuming a sensitivity of 84% and specificity of 99% for the QFT in an immune competent population, the VEMTI was estimated to 22% when taking misclassification into account.28–30
OR of Mycobacterium tuberculosis infection (MTI) by BCG vaccination and other demographic characteristics, among 953 children and young adults in East Greenland
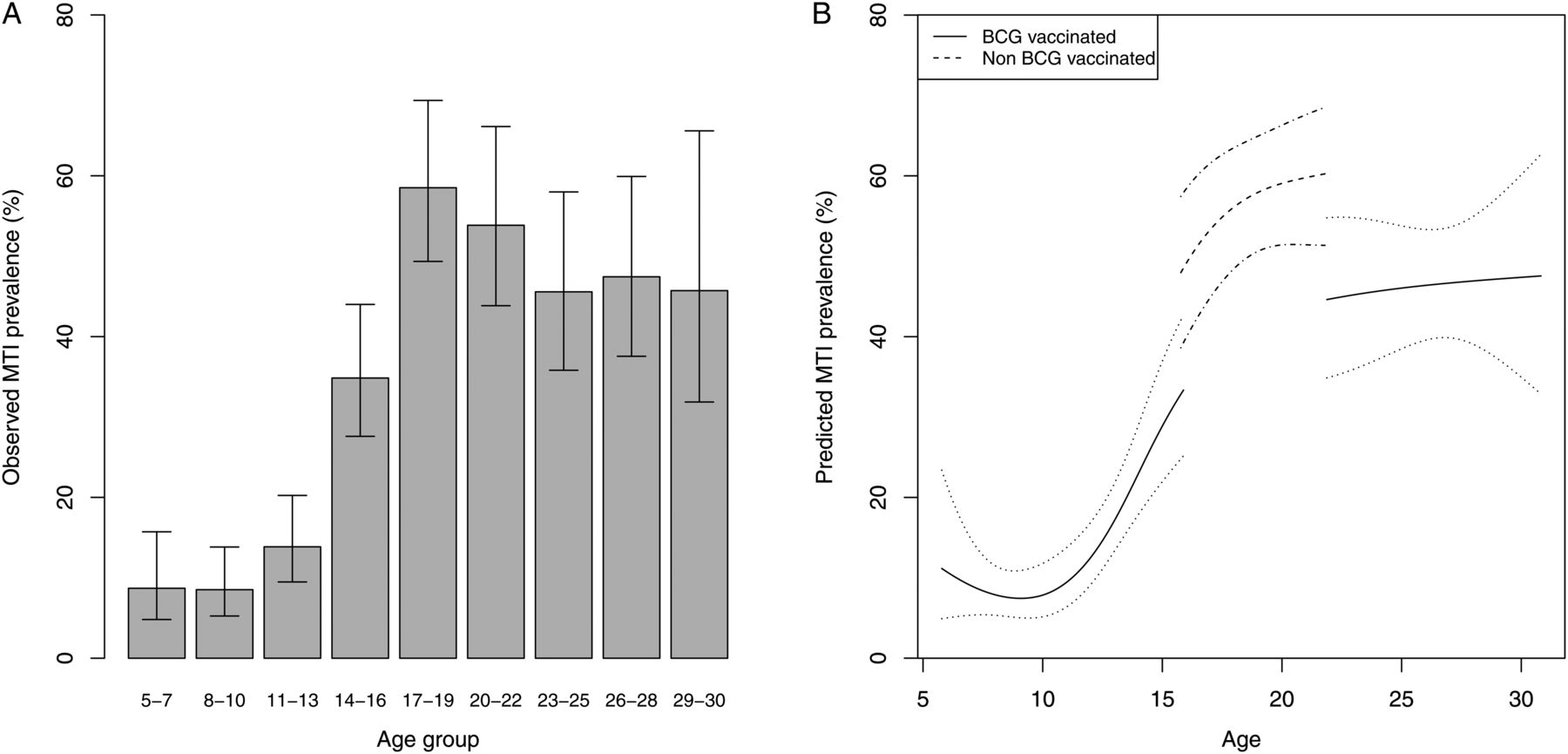
Observed and predicted Mycobacterium tuberculosis infection (MTI) prevalence by age. (A) The observed prevalence of MTI by age among the 953 study participants examined for MTI in East Greenland. The non-BCG vaccinated birth cohorts (age 16–21) are partly represented by the age groups 17–22. (B) The predicted MTI prevalence (with 95% CIs) by age, for BCG vaccinated and non-BCG vaccinated participants. Prediction is based on a logistic regression model, with age modelled by a spline.
The TB study
Through the CRS, 1697 individuals were identified as born in the Tasiilaq district (birth cohorts 1982–2006). The majority of the participants were Inuit (1520, 90%), 841 (50%) were men and 1278 (75%) were BCG-vaccinated. During a total of 21 148 person-years of follow-up, 94 (6%) were notified with TB at least once, corresponding to an average TB incidence of 440/100 000 participants/year. Mean (IQR) follow-up time was 12.5 years (6.4–17.8).
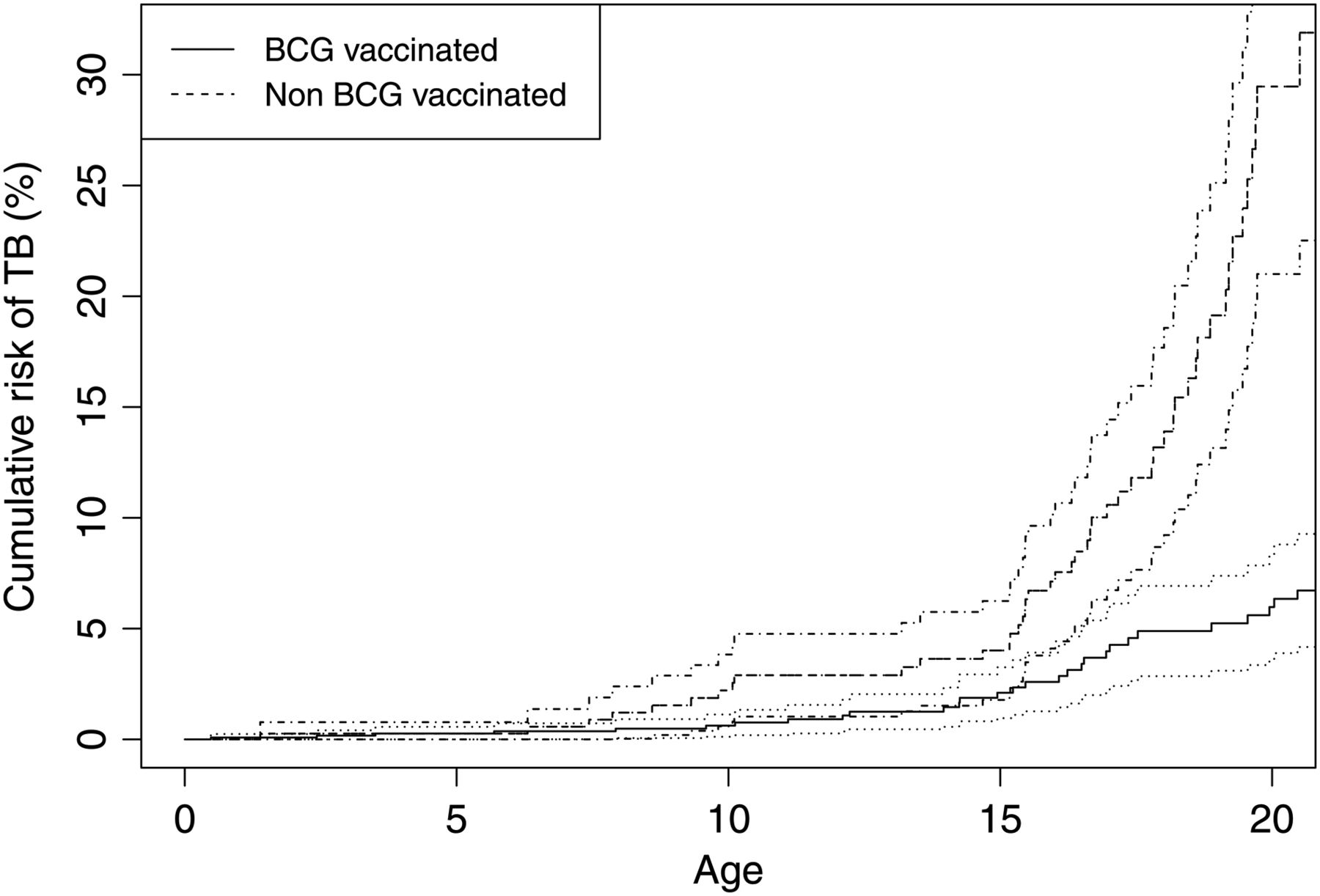
Among non-vaccinated individuals, 47 (11%) had been notified with TB compared with 47 (4%) among vaccinated. Figure 2 shows the cumulative risk of TB among the vaccinated and non-vaccinated participants by age. The unadjusted HR for TB among BCG-vaccinated individuals was 0.25 (95% CI 0.16 to 0.40) (table 3). In the adjusted analysis, BCG vaccination was significantly associated with reduced TB incidence, HR 0.50 (95% CI 0.26 to 0.95), p=0.03. The calculated BCG VETB was 50%. The association was the same in participants <age 15 years and ≥age 15 years (p=0.12). During follow-up, 764 (43%) emigrated and 102 (6%) died. To evaluate selection bias, we performed the same type of survival analysis but using death and emigration as outcome and stopping follow-up (censoring) at TB. We found no association between BCG vaccination and death or emigration. BCG vaccination was also significantly associated with reduced TB incidence when considering the Greenland-excluding-East-Greenland cohort (adjusted HR 0.53 (95% CI 0.37 to 0.76)).
HR of TB by BCG vaccination and other demographic characteristics in a cohort of children and young adults in East Greenland
{kind=link}
{kind=link}
The cumulative risk (with 95% CIs) of TB by age in a cohort of BCG vaccinated and non-BCG vaccinated children and young adults in East Greenland. At age 17, the probability of ever having had TB was 4% (95% CI 2% to 6%) among vaccinated versus 11% (95% CI 7% to 14%) among non-vaccinated participants.
Discussion
In the present study, we found BCG vaccination to significantly reduce both MTI and TB among children and young adults. To our knowledge, this is the first study to evaluate BCG VE against both MTI and TB in the same setting. Our findings are of particular interest as the Inuit population in Greenland represents a TB high-endemic population free from many elements often thought to interfere with BCG VE, such as immune deficiencies and NTM. The BCG VE was 20% against MTI and 50% against TB in this Inuit population with an M. tuberculosis prevalence of 29% and a TB incidence of 440/100 000 participants.
The BCG VE in reducing TB disease has been estimated in several studies,3–6 whereas studies estimating the BCG VE in reducing MTI remain scarce. To date, four similar studies on BCG and MTI have used an IGRA to define MTI in estimating the association between BCG and MTI.8–11 The protective effect of BCG vaccination against MTI was first reported in a prospective cohort study, performed in a TB medium-endemic setting among children who were TB contacts (adjusted OR 0.6 (95% CI 0.43 to 0.83)). The study relied on scar formation to determine BCG vaccination status.8 Similarly, a protective effect was reported in two British outbreak studies and in a cross-sectional and register-based study among children, pooling data from five sites in Europe with BCG vaccination status relying on vaccination card and/or BCG scar formation (OR of 0.41 (95% CI 0.30 to 0.55)).9–11 All previous studies reporting a protective effect of BCG vaccination against MTI have been carried out in TB low- or medium-endemic settings; our MTI study is the first to be placed in a TB high-endemic setting. Compared with previous studies our VEMTI of 20% is low. In three of the above mentioned studies, a BCG VEMTI was calculated from the OR converted into a RR, and not from a directly estimated RR.8–10 This is a controversial approach considering the high prevalence of the outcome (MTI).31 In our MTI study, we chose a more direct approach with estimation of the RR, which in most circumstances would lead to a more conservative estimate for the BCG VEMTI.
In the TB study, BCG vaccination significantly reduced the incidence of TB in the young study population, revealing a high BCG VETB. The effectiveness did not decline among individuals ≥age 15 years, as has been observed in other studies.32 One possible explanation could be the lack of NTM in the Arctic, which might lead to a better primary BCG vaccine response.2 ,5 ,13 The interference of NTM on the immune response has been discussed in a number of studies,5 ,13 and the mechanism is still debated.1 In a meta-analysis done on efficacy of the BCG vaccine, 66% of the heterogeneity of BCG vaccine efficacy was attributable to latitude.6 Whether this is attributed to NTM, thereby possibly also affecting the increased long-term effectiveness reported among Northern populations, is not clear as discussed by Sterne et al.32
Our studies have several strengths; they are large compared with previous studies and unique by being population-based, yielding generalisable effect measures. The BCG vaccine practice was similar throughout the country, with a remarkably high coverage,20 and non-vaccination of individuals born during 1991–1996 was a result of the change in vaccine policy applied in the entire country. This altogether minimises misclassification of the exposure and facilitates the best possible randomisation of the exposure in a non-randomised trial. In the cohort study, inclusion and censoring were based on information from national registers with mandatory registration, and we found no influence of BCG vaccination on censoring from the cohort, which together minimises the risk of selection bias in the cohort study. In the cross-sectional study, surviving to the time of sampling and wanting to participate was a prerequisite for inclusion in the eligible birth cohorts. In the BCG and TB studies, BCG status was not associated with mortality/emigration, and neither BCG vaccination nor TB status was associated with participation in the BCG and MTI study after age stratification. These findings suggest that BCG is not associated with inclusion of participants, minimising the risk of selection bias in the cross-sectional study. Information on demographic characteristics for participants in both studies was obtained from national registers, minimising information bias. Information on MTI was obtained using the QFT which has a sensitivity and specificity of approximately 84% and 99%.28 These findings would only lead to a minimal underestimation of the VEMTI. Information on TB diagnosis was obtained from national registers and was defined using guidelines following WHO criteria (all cases are believed to be notified according to the National Board of Health in Greenland). Because potential misclassification of the TB diagnosis most likely is non-differential, the specificity of the TB diagnosis is very high, and since TB is a rare event, the bias on the VETB will be negligible. These elements combined with the adjustment for confounding and the unique characteristics of the TB research environment strengthen the internal validity of the studies. We believe it is unlikely that the observed reduction of MTI and TB with BCG can be accounted for by bias or confounding.
To explore the potential effect of secular changes in the exposure to M. tuberculosis in the community, we compared the association between BCG and TB in the East Greenlandic cohort study with the association in the Greenland-excluding-East-Greenland cohort. Compared with the ongoing epidemic in East Greenland, micro epidemics emerged in North West Greenland in the late 1990s and in South Greenland in the beginning of the 21st century.15 ,16 Reassuringly, we found that the adjusted HRs in the two cohort studies for the association between BCG vaccination and TB were similar, suggesting that the effectiveness of the BCG vaccine is not modified by the community M. tuberculosis exposure.
In conclusion, we documented a significantly lower MTI prevalence and TB incidence among BCG vaccinated compared with non-vaccinated Inuit in Greenland. This population is free from many of the factors known to interfere with the effectiveness of the vaccine, which provided a unique opportunity to determine the VE in a high-endemic population. Thus, the vaccine appears to protect against TB and MTI.
Acknowledgments
We thank translator Abia Kuitse (Tasiilaq, Greenland), nurse Margit Weissmann (Tasiilaq, Greenland), medical student Simon Haahr (University of Copenhagen, Denmark), master of science and technology Elisabeth Alvestad (Olso, Norway) and medical doctor Karen Bjørn-Mortensen (Department of Epidemiology Research, SSI, Denmark) for help in conducting the field work. Furthermore, we would like to thank nurse J Sommer (Tasiilaq district hospital, Greenland) and laboratory technician H Due-Boye (Tasiilaq district hospital, Greenland) for assorted field work assistance. We would like to thank statistician Mikael Andersson for generating data from the national registries. We also thank The National Board of Health (Nuuk, Greenland) for generating TB notification data. Finally, we would like to thank all the participants in the Tasiilaq district and all the staff at the Tasiilaq district hospital, health clinics and district schools, Tasiilaq, Greenland.
References
Footnotes
-
Contributors Substantial contributions to the conception or design of the work: SWM, BS, MM, AK, STH, EMA, LC, JW. Substantial contributions to the acquisition of the data for the work: SWM, BS, TL, HCFS, STH, EMA. Substantial contributors to the analysis of the data for the work: LC, JW, SWM, BS, MM. Substantial interpretation of data for the work: SWM, BS, MM, AK, STH, EMA, LC, JW. Drafting the work or revising it critically for important intellectual content, final approval of the version to be published, and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved: SWM, BS, AK, LC, STH, EMA, TL, HCFS, JW, MM.
-
Funding The Commission for Scientific Research in Greenland and The Danish research Council (grant number 11-115052), Rosalie Petersens Fond, Ebba Celinders Legat, Aase og Ejnar Danielsens Fond, Dagmar Marshalls Fond, Fonden af 17.12.1981, Christian X fond, Fonden til lægevidenskabens fremme, The Danish Lung Association, Sundhedspuljen Greenland Self-Government and Forskningspuljen Greenland Self-Government. The sponsors played no role in the study design; the collection, analysis or interpretation of data, the writing of the report or in the decision to submit the manuscript for publication.
-
Competing interests None.
-
Ethics approval The Commission for Scientific Research in Greenland (approval No. 2012-4) and the Danish Data Protection Agency approved the studies.
-
Provenance and peer review Not commissioned; externally peer reviewed.