Article Text

Abstract
Background Person-to-person transmission of respiratory pathogens, including Pseudomonas aeruginosa, is a challenge facing many cystic fibrosis (CF) centres. Viable P aeruginosa are contained in aerosols produced during coughing, raising the possibility of airborne transmission.
Methods Using purpose-built equipment, we measured viable P aeruginosa in cough aerosols at 1, 2 and 4 m from the subject (distance) and after allowing aerosols to age for 5, 15 and 45 min in a slowly rotating drum to minimise gravitational settling and inertial impaction (duration). Aerosol particles were captured and sized employing an Anderson Impactor and cultured using conventional microbiology. Sputum was also cultured and lung function and respiratory muscle strength measured.
Results Nineteen patients with CF, mean age 25.8 (SD 9.2) years, chronically infected with P aeruginosa, and 10 healthy controls, 26.5 (8.7) years, participated. Viable P aeruginosa were detected in cough aerosols from all patients with CF, but not from controls; travelling 4 m in 17/18 (94%) and persisting for 45 min in 14/18 (78%) of the CF group. Marked inter-subject heterogeneity of P aeruginosa aerosol colony counts was seen and correlated strongly (r=0.73–0.90) with sputum bacterial loads. Modelling decay of viable P aeruginosa in a clinic room suggested that at the recommended ventilation rate of two air changes per hour almost 50 min were required for 90% to be removed after an infected patient left the room.
Conclusions Viable P aeruginosa in cough aerosols travel further and last longer than recognised previously, providing additional evidence of airborne transmission between patients with CF.
- Cystic Fibrosis
- Infection Control
- Bacterial Infection
- Respiratory Infection
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Key messages
-
What is the key question?
-
Several studies have suggested that airborne transmission of Pseudomonas aeruginosa among patients with cystic fibrosis (CF) is feasible; however, it is unclear how far cough generated aerosols travel or how long they remain viable in the airborne phase.
-
What is the bottom line?
-
Using two validated cough aerosol sampling systems to measure the viability of P aeruginosa in droplet nuclei we demonstrate that patients with CF produce cough aerosols containing viable organisms that are capable of travelling up to 4 m and persisting in the air for up to 45 min.
-
Why read on?
-
Data presented here challenge current CF infection control practices of separating patients by 1–2 m to prevent cross-infection by respiratory bacteria, suggesting a re-examination of current infection control practices within the CF community is needed.
Introduction
Communicable respiratory infections are an important cause of mortality and morbidity and result in healthcare costs worth billions of dollars.1 ,2 The person-to-person transmission of respiratory pathogens may occur by three key routes: contact transmission, where infectious respiratory secretions spread by direct contact or indirectly through a contaminated intermediate object or person; droplet transmission, where large infectious droplets travel directly over short distances from the respiratory tract to deposit onto mucosal surfaces (eg, nasal and conjunctival mucous membranes); and airborne transmission, involving dissemination of small droplet nuclei within the respirable size range that remain infectious over time and distance and are inhaled by susceptible individuals.3 Airborne transmission may pose a significant risk for hospital-acquired respiratory infection,4 with evidence that it is an important mode of acquisition for many respiratory infections, including Mycobacterium tuberculosis (TB) and Bordetella pertussis.5 ,6
Cystic fibrosis (CF) is the most common life-limiting autosomal-recessive disorder in Caucasians with most affected persons dying in their third-to-fourth decade from respiratory failure complicating chronic pulmonary infections.7 Pseudomonas aeruginosa is the most common pathogen in CF lung disease, and once infection is established there is an accelerated decline in lung function, quality of life and survival.8 ,9 While many patients with CF acquire P aeruginosa sporadically from the environment, molecular-typing studies show shared strains are common in some CF centres, suggesting person-to-person transmission may also be occurring.10 ,11 In Australia, P aeruginosa strains AUST-01 and AUST-02 are responsible for 40% of chronic infections11 and are associated with worse clinical outcomes and increased treatment requirements.11 ,12 The mechanisms of cross-infection in CF are unknown. However, despite CF centres implementing contact and droplet transmission control measures, P aeruginosa cross-infection continues11 ,13 ,14 and is only interrupted by implementing strict patient segregation policies.15 ,16
It seems that a plausible mechanism of transmission between patients is the airborne route. Indeed, patients with CF infected with P aeruginosa produce droplet nuclei containing viable bacteria.17 Furthermore, studies using air sampling in CF clinical settings have demonstrated viable P aeruginosa after physiotherapy and in corridors outside inpatient cubicle rooms housing patients with shared strain P aeruginosa infection.18 ,19 Others have also suggested that airborne transmission is feasible, with shared and mucoid P aeruginosa strains having a survival advantage.20 ,21 However, methods used in previous studies were unable to demonstrate how long viable bacteria were present in aerosols or how far they could travel from the original source. We therefore sought to enhance understanding of P aeruginosa aerosol production in CF in order to (i) determine the duration and distance of viable cough aerosols, (ii) identify the factors influencing pathogen viability and to (iii) understand the effects of room ventilation on controlling the duration of viable airborne P aeruginosa.
Methods
Subjects
Patients with CF (n=19) aged >12 years old and chronically infected with P aeruginosa were recruited from the Royal Children's Hospital (RCH) and The Prince Charles Hospital (TPCH), Brisbane, Australia. Exclusion criteria included recent pneumothorax, haemoptysis and pregnancy. Healthy, non-smoking controls (n=10) were recruited from hospital staff and their families. Further details are provided in the online supplementary methods. The RCH (HREC/11/QRCH/44), The University of Queensland (2012000615) and the Queensland University of Technology Human Research Ethics Committees (1100000618) approved the study and participants (or their guardians) provided their written, informed consent.
Clinical measurements
Subjects attended two study days separated by a mean (SD) 7.5 (4.7) days (range 2–21). A sputum sample was collected from each patient with CF on the day of testing. Cough manoeuvres were supervised by a healthcare professional and emergency equipment was available.
Forced expiratory volume in one-second (FEV1) and forced vital capacity (FVC) were measured on all subjects according to ATS/ERS guidelines.22 Respiratory muscle strength was measured by maximum inspiratory (MIP) and maximum expiratory (MEP) mouth pressures using a Micro Medical Respiratory Pressure Meter at TPCH. Weight, height, age, sex and clinical status (exacerbation or clinically stable) were recorded.
Determining the distance viable cough aerosols travel
A ‘Distance Rig’ (see online supplementary methods) permitted measurement of cough aerosols in a particle-free environment at distances up to 4 m from the subject (see online supplementary figure S1).23 An Andersen Impactor (28.3 L/min) captured and measured viable cough aerosol particles,17 and a Lasair II-110 optical particle counter (OPC) measured real-time particle concentrations and verified the absence of room air aerosol contamination in the Distance Rig. Andersen Impactor and OPC samples were collected through a common circular isokinetic inlet.
Subjects sat with their head in the Rig breathing high-efficiency particulate air (HEPA)-filtered air for 2 min to purge residual room air from their lungs before coughing as frequently and strongly as was comfortable for 5 min. The Andersen Impactor sampled continuously during the voluntary cough phase. Cough numbers were recorded manually. Cough aerosols were collected at 1, 2 and 4 m (order randomised) from each subject, who performed duplicate cough manoeuvres at each distance.
Determining duration of aerosol viability
A Duration Rig (see online supplementary methods) comprised a 0.4 m3 airtight stainless steel cylinder (illustrated in online supplementary figure S3) to assess the duration of aerosol particle viability in the airborne phase. The cylinder was rotated at 1.7 rpm so that gravitational settling and inertial impaction of particles was minimised.24 The system was flushed with HEPA-filtered air before sample collection so that cough aerosols were not contaminated by room air aerosols.
Subjects were seated and fitted with a snorkel-style mouthpiece (CareFusion Australia) connected to 10 cm of flexible tubing. A nose clip was attached and subjects breathed filtered air for 2 min, and then coughed as much as was comfortable for 2 min, with cough numbers recorded manually. The Rig was isolated, and the resultant cough aerosols were aged for 5, 15 or 45 min. Suspended particles were collected with an Andersen Impactor at the conclusion of the ageing period. Measurements after 5 and 15 min ageing were performed in duplicate while, for logistic reasons, only one measurement was performed after 45 min ageing.
Microbiology
Cough aerosol cultures were performed with chocolate bacitracin (300 mg/mL) agar using previously described incubation conditions and colony-forming units (CFU) count protocols.17 Quantitative (sputum) and qualitative cultures were performed on respiratory samples using standard techniques. After presumptive screening, P aeruginosa isolates were confirmed by duplex real-time (RT) PCR assays.11 P aeruginosa isolates were genotyped using enterobacterial repetitive intergenic consensus-PCR and clusters analysed alongside a previously characterised panel of Australian shared P aeruginosa strains.11
Statistical analysis and modelling of airborne P aeruginosa
Continuous variables are reported as mean and SD, and binary variables as frequency and percentage. Analyses were performed using χ2 test, one-way and mixed-effects analysis of variance with subjects as the random factor, followed by the least significant difference procedure. Repeatability was estimated by intraclass correlation using a two-way mixed effects analysis of variance. CFU data were transformed as log(X+1), and their means and 95% CI were back transformed to the original units for ease of interpretation. We also performed a sensitivity analysis to account for the potential ‘stacking’ of organisms in the cascade impactor (see online supplementary methods). P aeruginosa decay over time was assessed using the Duration Rig data (5, 15 and 45 min). The half-life of airborne P aeruginosa was estimated from the slope of the decay curve. A model (see online supplementary methods) estimated the relative effects of ventilation and airborne biological decay on P aeruginosa removal in different healthcare settings, including the study site.20 ,25 Ventilation rates were expressed in the standard units of air changes per hour (ACH), which describe how many times a volume of air equal to the volume of a room enters each hour.
Results
Subjects were well matched for age, sex and height, but those with CF had lower weight, body mass index and lung function (table 1). All subjects completed the cough manoeuvres safely. Four patients with CF were studied during a pulmonary exacerbation. Within the CF group there was no significant change in spirometry between study days (intraclass correlation coefficient (95% CI) 0.79 (0.48 to 0.92)). Similarly, total CFUs for P aeruginosa in cough aerosols, cough counts and log P aeruginosa sputum concentration within subjects were highly repeatable (see online supplementary table S1).
Demographic, clinical and microbiological characteristics of the study subjects at time of initial cough aerosol experiment, according to type of subject*
Eighteen patients with CF produced sputum and one provided a cough swab (table 1), with P aeruginosa isolated from all and 15/19 (79%) yielding at least one mucoid isolate. Sputum P aeruginosa concentrations ranged from 4.0×106 to 4.2×109 CFU/mL. Genotypic analysis revealed 12 strains shared commonly within the Australian CF community11; AUST-01 (1), AUST-02 (7), AUST-06 (2), AUST-07 (1) and AUST-19 (1), and seven unique strains. Five patients harboured two different strains. Other organisms cultured are detailed in table 1.
P aeruginosa was cultured in cough aerosols from all patients with CF, but not from any controls. Viable P aeruginosa was isolated at 4 m from 17/18 (94%) and at all distances from 16/18 (89%) of the CF group (figure 1). Aerosolised P aeruginosa remained viable for 45 min from 14/18 (78%) subjects in the duration experiments (figure 2). Most viable P aeruginosa isolates were cultured from particles <3.3 μm (table 2) and the strains cultured from cough aerosols were genotypically indistinguishable from those isolated in respiratory samples from the same patient. Stenotrophomonas maltophilia and Arxula adeninivorans were also cultured in cough aerosols and sputum from two patients. No other respiratory pathogens cultured in sputum were isolated from cough aerosols. No P aeruginosa or other microbes identified in cough aerosols were isolated from surface swabs or blank aerosol samples taken during the studies (see online supplementary methods).
Colony-forming unit (CFU) counts of Pseudomonas aeruginosa isolated from the cough aerosol cultures of subjects with cystic fibrosis (CFUs in total aerosol, and in large and small particle fractions are shown)*
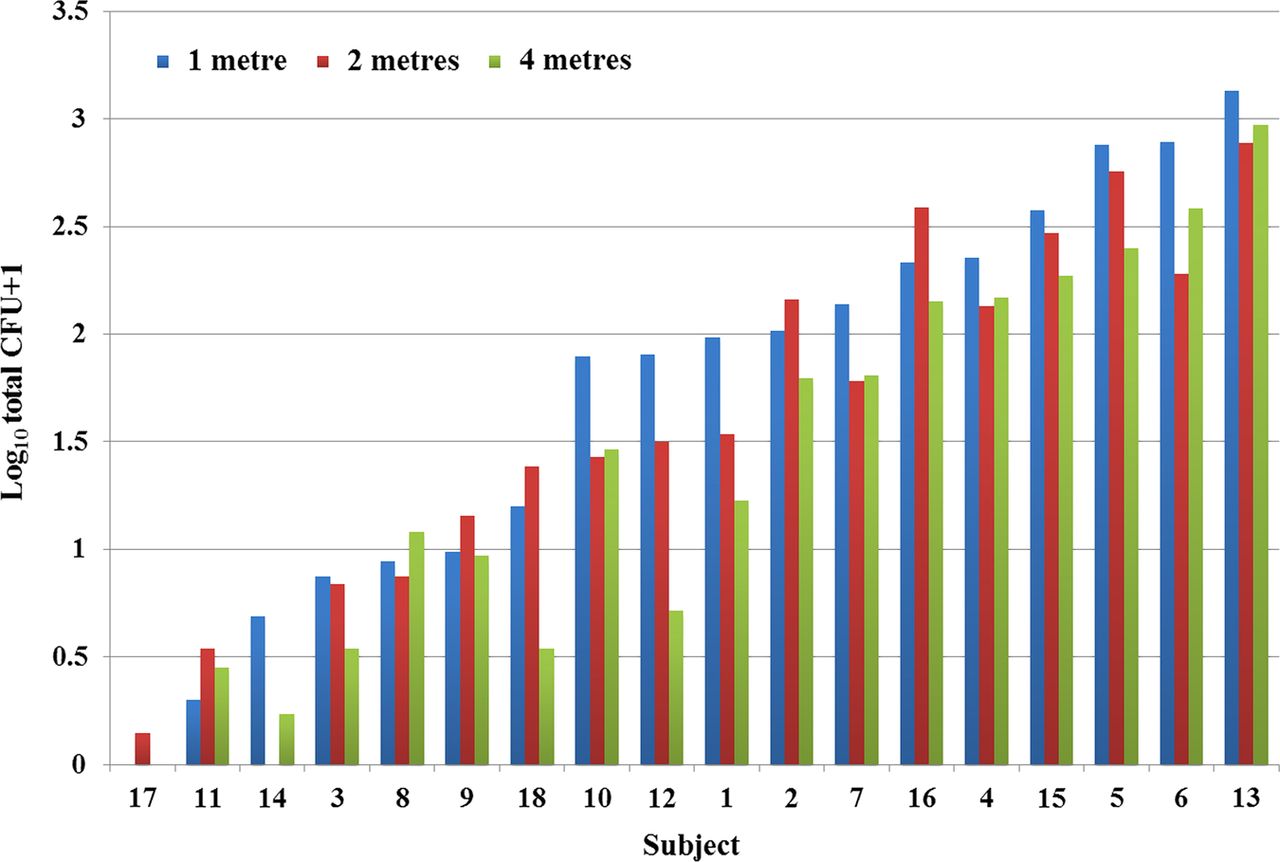
Log10 combined total colony-forming unit counts of Pseudomonas aeruginosa isolated at 1, 2 and 4 m from the Distance Rig cough aerosol cultures of subjects with cystic fibrosis.

Log10 combined total colony-forming unit counts of Pseudomonas aeruginosa isolated after 5, 15 and 45 min from the Duration Rig cough aerosol cultures of subjects with cystic fibrosis.
Marked intersubject heterogeneity was seen in the total numbers of viable P aeruginosa cultured from cough aerosols (figure 1; see online supplementary table S2). Measured P aeruginosa CFUs decreased with the distance the aerosol travelled and with the ageing time; CFUs were significantly higher at 1 m than 4 m, and at 5 min than 45 min (table 2). CFUs remained significantly higher for both distance and duration when corrected for the effects of stacking (see online supplementary table S3). In both distance and duration studies, strong correlations were seen between total, small and large fraction cough aerosols (r=0.90–1.0). A positive correlation was found between sputum and aerosol P aeruginosa CFUs in both distance (r=0.73–0.78) and duration (r=0.85–0.90; see online supplementary table S4) studies, although there was no significant correlation found between clinical or demographic variables and cough aerosols produced in either study. Correlations for these variables were unchanged when measured CFUs were corrected for stacking (see online supplementary table S5)
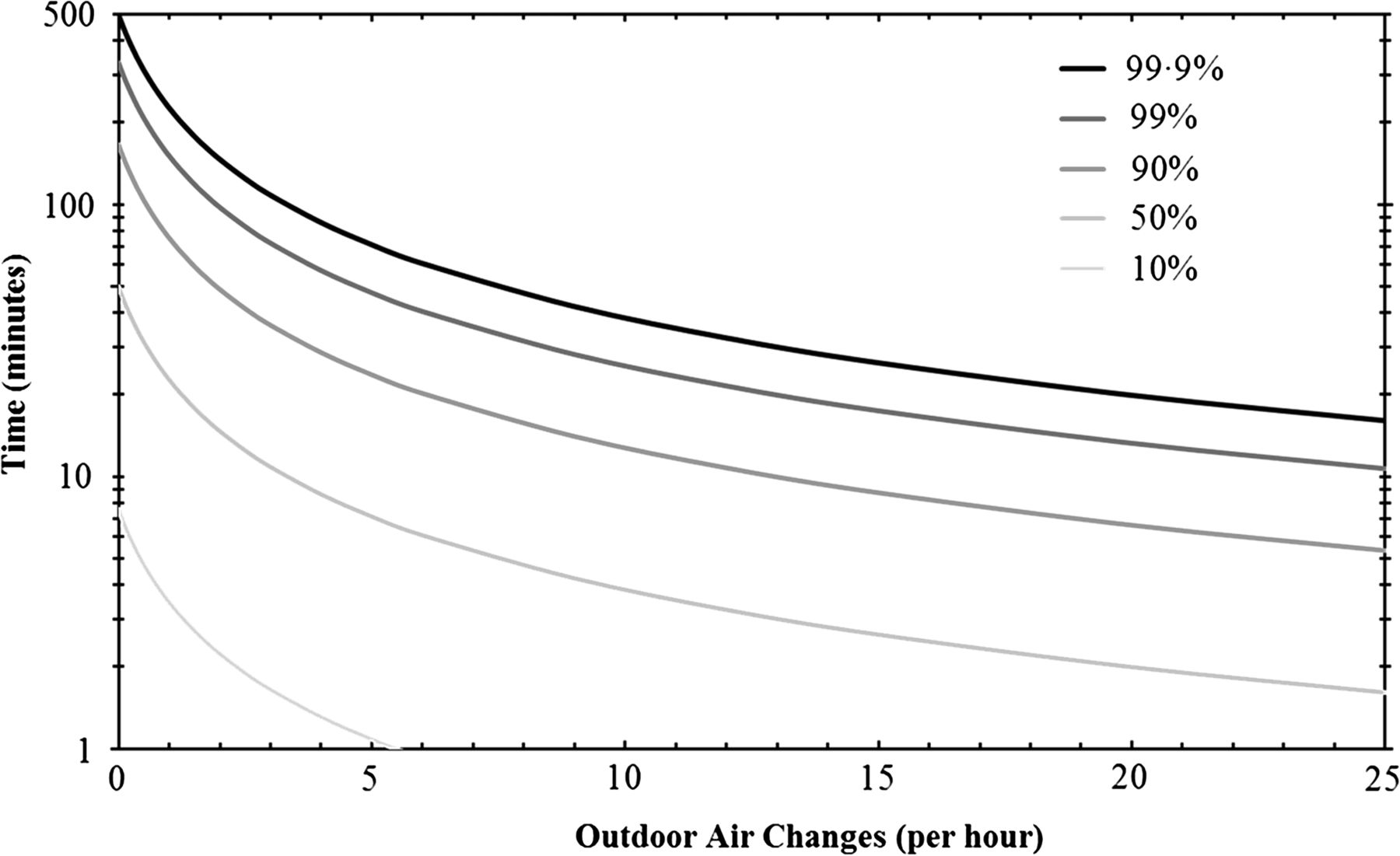
The influences of biological decay and room ventilation on P aeruginosa in cough aerosols were modelled (see online supplementary methods). Environmental conditions in the Duration Rig were similar to those in the air-conditioned clinical setting. The number of viable P aeruginosa in cough aerosol followed an exponential decay with a half-life of 50 min (95% CI 30 to 151 min). Room ventilation removed additional viable P aeruginosa and became the dominant mechanism of removal at ventilation rates above the biological decay rate of the cough aerosol (ie, approximately 0.85 ACH). Figure 3 shows the time taken to achieve 10, 50, 90, 99 and 99.9% reductions in airborne P aeruginosa following the departure of a source patient, including the combined effects of biological decay and room ventilation. At 2 ACH, 90% of viable airborne P aeruginosa are removed in approximately 49 min (95% CI 41 to 61 min), decreasing as ventilation rate increases to approximately 24 min (95% CI 22 to 26 min) at 5 ACH and to 13 min (95% CI 12 to 13 min) at 10 ACH.
{kind=link}
{kind=link}
{kind=link}
Time taken to achieve 10, 50, 90, 99 and 99.9% reductions in airborne Pseudomonas aeruginosa due to the combined effects of biological decay and room ventilation.
Discussion
Cross-infection between patients with CF can adversely affect health outcomes, but how this occurs and the transmission pathways involved remain uncertain. We have shown that patients with CF produce aerosols containing viable P aeruginosa during coughing. Particles within the respirable range persist over distance and time, providing a potential vehicle for airborne transmission between patients. Marked intersubject heterogeneity of aerosol production was observed, suggesting that some patients may be ‘super-spreaders’ of P aeruginosa. Finally, sputum P aeruginosa concentration was a strong predictor of viable cough aerosol concentrations.
Evidence of highly prevalent shared P aeruginosa strains within CF populations suggests person-to-person transmission.10 ,11 ,26 Using air sampling equipment both in the clinical setting, viable P aeruginosa have been demonstrated close to patients with shared strain P aeruginosa infection.18 ,19 The clinical significance of these findings was unclear and led us to study the size distribution of cough aerosols, and we have previously demonstrated P aeruginosa can be present in aerosols generated by coughing.17 However, we were unable to determine how far these aerosols travelled or the duration they remained viable in the airborne phase. An in vitro aerosol production system has demonstrated that artificially produced P aeruginosa aerosols can survive up to 45 min and that survival was greater with mucoid P aeruginosa.20 ,21 The present study confirms aerosols produced during coughing by infected patients contain viable P aeruginosa that travel up to 4 m and stay suspended for at least 45 min. These data add to existing evidence that airborne transmission is likely to play a role in patients with CF acquiring P aeruginosa.
Our study demonstrates that droplet nuclei, generated by coughing, and containing viable P aeruginosa, are small enough to stay airborne for extended periods and over long distances. They are also well within the size range to deposit within the tracheobronchial tree following inhalation.27 Such droplets can be efficiently disseminated to locations far from their origin by mechanical room air ventilation systems, which often recirculate up to 80–90% of air used for heating or cooling. The role of room ventilation as a potentiator of airborne transmission of microbes such as M tuberculosis, measles, SARS-coronavirus and varicella zoster is well documented.4
Published guidelines for ventilation in hospitals suggest that 2 ACH of fresh (ie, non-recirculated) air are required for clinic rooms and general wards, 3 ACH are recommended for procedure rooms and 12 ACH are needed for isolation rooms.28 ,29 We have previously published results of measuring ACH in various clinical locations within TPCH and found that these meet or exceed recommended levels in most cases, with an extreme example of almost 24 ACH in an isolation room in the emergency department.25 However, the data from the present study suggest that a clinic room with the recommended two ACH may require almost an hour after a patient harbouring P aeruginosa leaves the room before 90% of the viable bacteria are removed from the air (see online supplementary methods). These data have substantial implications for CF infection control practices. Our modelling suggests that increasing room ventilation provides some benefit; however, the time required to remove 90% of potentially infectious aerosols still exceeds 10 min despite substantial increases in ACH (figure 3). A new paradigm may be needed, such as employing within CF centres advanced ventilation and ultraviolet germicidal irradiation (UVGI) techniques to achieve infection control, as is done for TB clinics.30 ,31
This study has several important limitations. The infectious inoculum required to establish P aeruginosa infection in CF is unknown and may vary between patients.20 Thus, it is impossible to estimate to what extent viable aerosols of P aeruginosa need to be removed to eliminate the risk of infection in susceptible patients. In many CF clinical settings, contact and droplet infection control measures have been implemented, but reduced rates of shared P aeruginosa strain infections have been reported only in centres employing strict cohort segregation based upon molecular typing surveillance.15 It therefore remains uncertain whether these simpler measures are sufficient, and if preventing airborne transmission should also be considered when strict segregation of large patient cohorts attending major CF centres is not always feasible.14
Our study included a small number of older patients with chronic P aeruginosa infection and moderately severe airflow obstruction. Thus, we cannot comment on viable aerosol production during coughing by younger or healthier patients or in those with transient P aeruginosa infections. In addition, we used culture media that selected for aerobic gram-negative bacteria and we cannot provide data on other microbes, including Staphylococcus aureus, non-tuberculous mycobacteria or respiratory viruses.14 ,32 ,33 Future studies using other selective media to determine the viability of other microorganisms in cough aerosols are now required. Due to bactericidal effects, it is also possible that the bacitracin used in the culture media reduced the recovery of some P aeruginosa organisms. Finally, modelling data assume that the room air is perfectly mixed, which is rarely the case. As such, our estimates of the time taken to remove viable P aeruginosa from a clinic room may be overestimates or underestimates of real-world scenarios (see online supplementary methods).
The present study uses bacterial infection in patients with CF to demonstrate the potential for aerosol transmission in healthcare settings and adds to studies suggesting similar mechanisms for M tuberculosis and for B pertussis in non-human primate models.5 ,6 Our results provide further evidence, which challenges the dogma that CF bacterial pathogens within droplet nuclei have limited survival in air. Indeed, airborne transmission may be a more important mechanism of cross-infection within the CF community than previously considered to be the case. Furthermore, our data add to the controversy generated by the current USA CF Foundation guidelines that only one person with CF attend a CF Foundation-sponsored or CF Centre-sponsored event34; recommendations strongly opposed by some adults with CF.35
In summary, this study indicates that when patients with CF harbouring P aeruginosa cough, they produce an aerosol containing viable organisms capable of travelling 4 m and persisting in the air for 45 min. These data challenge current CF infection control guidelines that remain in place in many parts of the world, including the separation of patients by 1–2 m to prevent cross-infection by respiratory bacteria.13 ,36 Consequently, further studies on transmission are needed and infection control practices recommended currently for the CF community may need to be re-evaluated.
Acknowledgments
We are grateful to all the participants and research nursing staff including Andrea Beevers (The Prince Charles Hospital, Brisbane), Sue Edwards, Rebecca Jackson, Heather Saddington and Emma Sanderson (Royal Children's Hospital, Brisbane) for the support in subject preparation and supervision during studies. We thank Dr Boris Polak from the Sir Albert Sakzewski Virus Research Centre and Clinical Medical Virology Centre, The University of Queensland for his assistance preparing the online supplementary figures.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
LDK, GRJ and TJK contributed equally; LM and SCB contributed equally.
-
Contributors LDK, GRJ, TJK, LM and SCB contributed equally to the work. LDK, GRJ, KG, PDS, CEW, LM and SCB conceived the study and led the funding application. All authors contributed to the experimental design and management of the study. LDK and GRJ supervised by LM led the development and verification of the sampling Rigs and collection of the cough aerosol samples. JC, MW, CEW and SCB contributed to subject recruitment and collection of clinical data and samples. TJK, JAK and KAR led the microbiological sampling, culture, identification and genotyping. PKO led the statistical analyses. Manuscript was written by LDK, TJK, PDS and SCB, with input from coauthors. SCB had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
-
Funding The study was funded by grants from The Prince Charles Hospital Foundation (#MS2010-42), Children's Health Foundation Queensland (#50005), Institute of Health and Biomedical Innovation-Queensland University of Technology (Collaborative Research Development Grant Scheme to LM, LDK and GRJ (#2010002239); Early Career Researchers Grant to GRJ (#2009001211)), Australian Research Council Discovery Grant to LM (DP0558410), Perpetual Philanthropy, Queensland Health Office of Health and Medical Research (Health Fellowships for PDS (QCOS008476), CEW (QCOS012808) and SCB (QCOS013795)), National Health and Medical Research Council (NHMRC) Early Career (Australian Public Health) Fellowship to LDK (#1036620) and a NHMRC Australia Senior Principal Research Fellowship (#1002035) to PDS.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Royal Children’s Hospital Human Research Ethics Committee, The University of Queensland Medical Research Ethics Committee, Queensland University of Technology Human Research Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.