Article Text

Abstract
In the ASTER study, mediastinal staging was more accurate for patients randomised to combined endobronchial and endoscopic ultrasound, followed by surgical staging if endoscopy was negative, versus surgical staging alone. Here, we report survival, quality of life and cost effectiveness up to 6 months, for the UK, The Netherlands and Belgium, separately. Survival in the two arms of the study was similar. In all three countries, the endosonography strategy had slightly higher quality-adjusted life years over 6 months, and was cheaper. Therefore, based on clinical accuracy and cost effectiveness, we conclude that mediastinal staging should commence with endosonography.
- Thoracic Surgery
- Health Economist
- Non-Small Cell Lung Cancer
- Lung Cancer
- Bronchoscopy
Statistics from Altmetric.com
Introduction
Historically, mediastinal staging for lung cancer used cervical mediastinoscopy. We previously reported a multicentre, randomised, controlled study, comparing surgical mediastinal staging with combined endobronchial (EBUS) and endoscopic (EUS) ultrasonography—the ASTER study.1 Among patients with (suspected) non-small cell lung cancer (NSCLC), a staging strategy combining endosonography and surgical staging (if endosonography was negative), compared with surgical staging alone, resulted in greater sensitivity for detection of mediastinal nodal disease. UK-specific cost-effectiveness results showed that the endosonography strategy was cheaper and patients had better quality of life during staging.2 However, a multinational trial permits assessment of consistency of results across three European countries. Here, we report survival, quality of life, and resource use during the trial, together with trial-based, country-specific, cost-effectiveness analyses.
Methods
ASTER was a prospective, randomised, controlled trial carried out at Ghent and Leuven University Hospitals, Belgium; Leiden University Medical Centre, The Netherlands, and Papworth Hospital, UK. Patients with (suspected) NSCLC requiring mediastinal staging based on CT and PET-CT were randomised to surgical staging alone or to combined endoscopic and endobronchial ultrasound followed by surgical staging (if no nodal disease on endosonography). The primary endpoint was diagnostic accuracy of each strategy for mediastinal staging. Secondary outcomes were rates of unnecessary thoracotomies and complications, The health economic study compared survival, quality of life, and cost effectiveness of the two diagnostic strategies over 6 months after randomisation.
Quality of life
Quality of life was measured using local language EuroQoL EQ-5D at baseline, end of staging (before thoracotomy) and at 2 and 6 months after randomisation for all UK patients, and for patients recruited after April 2008 in the Dutch and Belgian centres.3 EQ-5D responses were transformed to utility values for each patient and quality-adjusted life years (QALYs) were calculated as the standard area under the utility curve method up to 6 months after randomisation.
Cost-effectiveness analysis
Costs were estimated from a healthcare payer viewpoint using resources from all patients in the study (see online supplement). An NHS and personal social services perspective was adopted for the UK, and a health service provider and patient copayment perspective in The Netherlands and Belgium. Resource use data for EBUS/EUS, surgical staging, thoracotomy, surgery other than planned thoracotomy, chemotherapy, radiotherapy, hospital and hospice stays was collected prospectively after April 2008, and retrospectively from medical records for patients recruited before April 2008. These were multiplied by unit costs to estimate the total direct healthcare costs per patient. Costing methods depended on nationally available cost data and locally recommended guidelines for costing from health technology assessments (see online supplement).
Statistical and economic analysis
Survival analysis included Kaplan–Meier and log rank methods. Mean utilities were estimated from multivariate linear models including baseline measurement, country and treatment as independent variables. The proportion of patients who had each component of resource use was compared using the Pearson's χ2 test. Bayesian parametric modelling was used to estimate expected costs and QALYs over 6 months from randomisation under each diagnostic strategy. This included information from patients with partially observed resource usage and QALY data, as well as patients with complete data. Technical details of the models have been published previously.2
Results
Two hundred and forty-one patients were randomised, 118 (49%) to surgical staging and 123 (51%) to endosonography. Eighty-one were recruited in The Netherlands, 132 in Belgium (88 Ghent; 44 Leuven) and 28 from the UK. Mean age was 64.5 years (SD 8.9).
Clinical results
Full clinical results have been published previously.1 Briefly, sensitivity for detecting mediastinal nodal metastases was 79% (41/52, 95% CI 66 to 88) for surgical staging alone and 94% (62/66, 95% CI 85 to 98) in the endosonography arm (p=0.02). Corresponding negative predictive values were 86% (95% CI 76 to 92) and 93% (95% CI 84 to 97), respectively (p=0.26). There were 21/118 (18%) unnecessary thoracotomies in the surgical staging arm compared with 9/123 (7%) in the endosonography arm (p=0.02). The complication rate was 7/118 (6%) in the surgical arm versus 6/123 (5%) in the endosonography arm (p=0.78).
Survival
There were 20 deaths within 6 months of randomisation, 9 in the endosonography group; 11 in the surgical staging group (log rank test p=0.57).
EuroQoL EQ-5D
Of the 241 patients, 144 (60%) completed baseline EQ-5D questionnaires. At the end of staging, at 2 months and 6 months, 139 (97%), 132 (92%) and 124 (86%) patients completed the questionnaires. Throughout the 6-month period, endosonography and surgical staging arms had very similar EQ-5D utilities with mean differences lying close to zero, and CIs crossing zero. In the Netherlands and the UK, there was little difference between the groups at any time point, while in Belgium the endosonography strategy resulted in slightly higher utility during staging and slightly lower utility during follow-up. When these utilities are combined with survival, the overall mean (95% CI) increase in quality-adjusted survival due to endosonography staging for the three countries was very similar, being 0.014 QALYs (−0.018 to 0.046) in The Netherlands, 0.016 (−0.020 to 0.054) in Belgium, and 0.016 (−0.021 to 0.056) in the UK. This resulted in an overall increase in QALYS for endosonography compared with surgical staging alone of 0.015 QALYs (−0.023 to 0.052) over 6 months.
Resource use
Staging procedures and thoracotomy were the main drivers of cost. All bar one (surgical arm) patient received the assigned staging strategy. Median length of stay after thoracotomy was longer in Belgium and shorter in The Netherlands (p=0.001) than in the UK. There was variation between countries in the proportion of patients who had additional treatment; Belgian patients were more likely to have chemotherapy in the first 2 months (p=0.054) and Dutch patients less likely to have chemotherapy after 2 months (p=0.0097). Compared with Belgian and UK patients, Dutch patients were less likely to be admitted to hospital in the first 2 months (p=0.0014) and after the first 2 months (p=0.04). However, these therapies had less influence on the overall costs and their average costs were similar between diagnostic strategy groups.
Although there were differences in the cost of resource use in the three countries, there were some consistent patterns. All countries estimated a lower cost due to surgical staging and thoracotomy in the endosonography arm and the sum of these savings outweighed the additional costs of endosonography. The cost of chemotherapy was greater in the endosonography arm in the first 2 months, but greater in the surgical arm after 2 months. In general, the reverse was true for radiotherapy and hospital admissions, which cost more for the surgery arm in the first 2 months and more for the endosonography group after 2 months.
Cost effectiveness
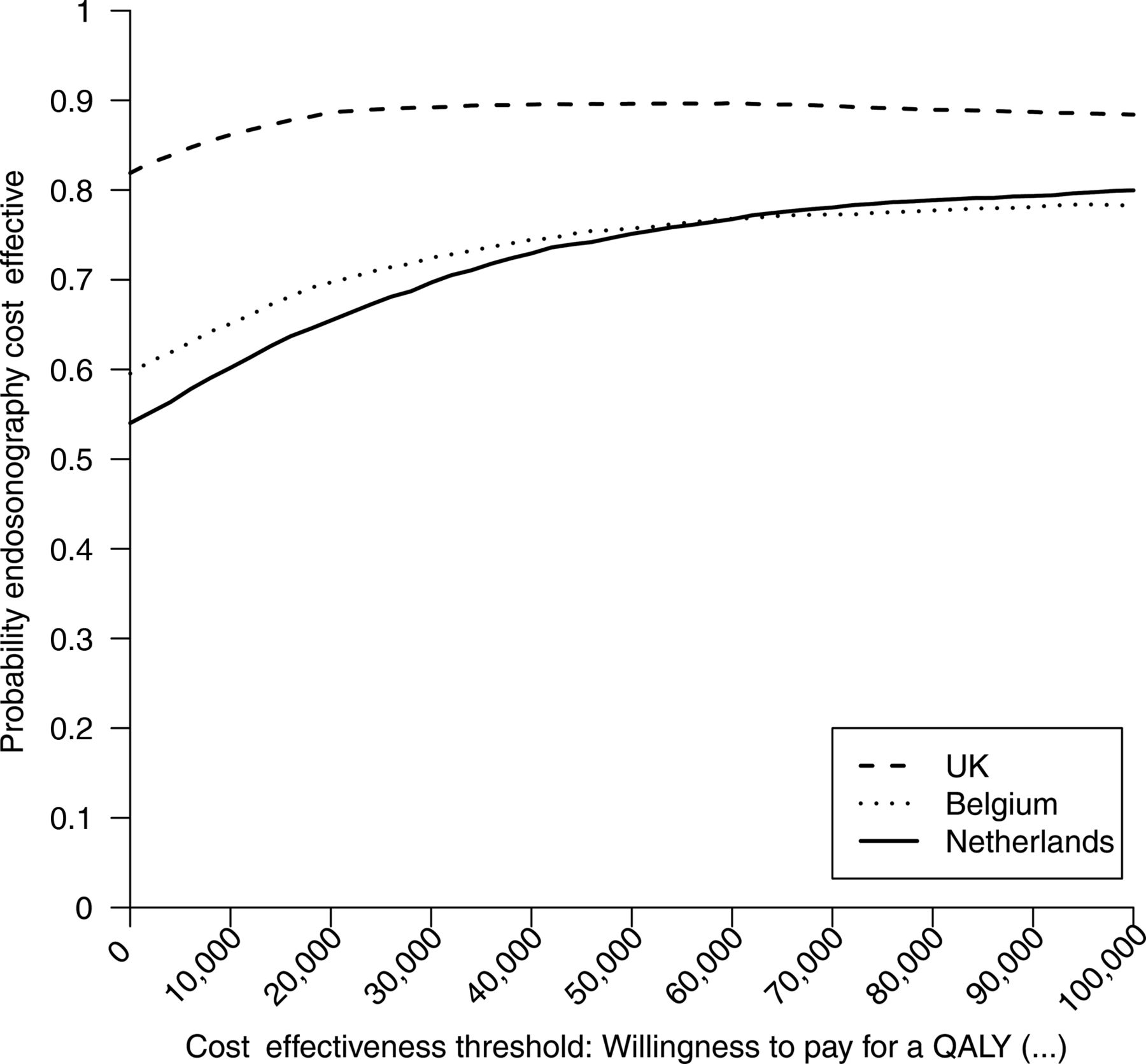
The cost effectiveness acceptability curve (figure 1) shows the probability that the endosonography strategy is cost effective (ie, represents value in terms of delivering health outcomes, given the cost) against the amount a decision maker is prepared to pay for one additional QALY (the cost-effectiveness threshold). Total costs over the 6 months for each country, and the mean difference in costs between the two arms are shown in the online supplement. All three countries reported a mean cost saving for the endosonography strategy, which was greatest in the UK.
{kind=link}
Cost effectiveness acceptability curve under base-case full Bayesian model: costs compared between three countries.
Discussion
We examined intercountry cost effectiveness of mediastinal staging strategies within the ASTER trial.1 In all three countries, the endosonography strategy had lower mean cost and greater mean QALYs. Despite differences in patient management, resource use and unit costs, the mean difference in 6-month costs for all three countries was lower using the endosonography strategy. The cost effectiveness acceptability curve (figure 1) shows that, if a decision maker is not prepared to pay any additional euros, then the probability that the endosonography strategy is cost effective compared with surgical staging varies from 55% in The Netherlands to 82% in the UK. Thus, it is likely that endosonography delivers greater health outcomes at lower or equal cost, or alternatively, cost savings with equal health outcomes.
Few studies have examined cost effectiveness of mediastinal staging. Work using retrospective data and economic models have made multiple assumptions to compare alternative strategies.4 The 2011 National Institute of Health and Care Excellence guideline for lung cancer diagnosis and treatment includes an economic model for a number of potential diagnostic pathways but was limited by the lack of empirical evidence and was largely based on expert judgement.5
Limitations
Although our results come from a rigorously conducted study, the small sample size within each country combined with variation in management of individual patients, means cost effectiveness was measured imprecisely. Consistency of cost estimates and QALY differences in the three countries is reassuring but confirmatory studies of cost effectiveness in larger cohorts are required. The later start of the cost-effectiveness component of the study resulted in some missing EQ-5D questionnaires and some resource use components. Although we used modern, sophisticated, statistical methods in an attempt to minimise any bias this may have introduced, we cannot be sure that this was completely eradicated.
Conclusions
A strategy of endosonography-lead mediastinal staging appears cost effective compared with surgical staging alone. Despite differences in patient management and costing between countries, the endosonography strategy was cheaper and had slightly higher mean QALY in all three countries.
Acknowledgments
We are grateful to the ASTER trial steering committee members who oversaw the running of the trial and met regularly to discuss study progress. The international group comprised Jouke Annema, Kurt Tournoy, Christophe Dooms, Robert Rintoul, Klaus Rabe, Ellen Deschepper and Olaf Dekkers. The Papworth ASTER management group comprised Robert Rintoul, Linda Sharples, Robert Buttery, Martin Buxton, Alistair Grant, Gethin Griffith, Victoria Hughes, Nicholas Carroll and Lavinia Magee. We are also grateful for the advice of the independent data monitoring committee members: Mick Peake (Chairman), Edwin Chilvers, John Edwards and Sarah Barry (independent statistician). We also thank all the staff at the participating centres, the referring chest physicians and the patients for their participation. We thank Clazien Bouwmans-Frijters of the Institute for Medical Technology Assessment, Erasmus University, Rotterdam, The Netherlands and Ann Tanghe and Jorgen Bauwens of Hict, Bruges, Belgium for providing unit costs for The Netherlands and Belgium, respectively.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement 1
Footnotes
-
Contributors RCR and LDS conceived and designed the cost-effectiveness study, contributed to data collection and trial monitoring in the UK, supervised the cost-effectiveness analysis and wrote the first draft of the paper. MJG obtained resource use costs from each centre, performed resource use modelling and drafted the sections of the report relating to this analysis. CJ designed and implemented the final Bayesian cost-effectiveness model and drafted the sections of the report relating to this analysis. VH contributed to the design of the cost-effectiveness study and managed the UK arm of the trial. KGT, CD and JTA took responsibility for the conduct of the trial in their respective centres and supervised local clinical and health economic data collection. All authors reviewed and approved the final draft of the manuscript.
-
Funding The study was funded by a grant from the UK National Health Service R&D Health Technology Assessment programme (project no. 06/302/216). LDS and CJ were funded by the Medical Research Council programme number U015232027. RCR was supported, in part, by the NIHR Cambridge Biomedical Research Centre and Cambridge Experimental Cancer Medicine Centre. Local support for data collection at Ghent University Hospital was provided by the Zorg-programma Oncologie Ghent (ZOG). The trial was registered as ISRCTN 97311620 and with ClinicalTrials.gov as NCT00432640.
-
Competing interests Papworth Hospital acts as a reference centre for Olympus UK. Olympus UK provide a non-entailed educational grant towards the Papworth EBUS course for which RCR is the director.
-
Ethics approval Cambridge.
-
Provenance and peer review Not commissioned; internally peer reviewed.
-
Data sharing statement All available data for this study has been submitted in the on-line version of this paper.