Article Text

Abstract
Background Short-term exposure to outdoor fine particulate matter (particles with a median aerodynamic diameter <2.5 μm (PM2.5)) air pollution has been associated with adverse health effects. Existing literature reviews have been limited in size and scope.
Methods We conducted a comprehensive, systematic review and meta-analysis of 110 peer-reviewed time series studies indexed in medical databases to May 2011 to assess the evidence for associations between PM2.5 and daily mortality and hospital admissions for a range of diseases and ages. We stratified our analyses by geographical region to determine the consistency of the evidence worldwide and investigated small study bias.
Results Based upon 23 estimates for all-cause mortality, a 10 µg/m3 increment in PM2.5 was associated with a 1.04% (95% CI 0.52% to 1.56%) increase in the risk of death. Worldwide, there was substantial regional variation (0.25% to 2.08%). Associations for respiratory causes of death were larger than for cardiovascular causes, 1.51% (1.01% to 2.01%) vs 0.84% (0.41% to 1.28%). Positive associations with mortality for most other causes of death and for cardiovascular and respiratory hospital admissions were also observed. We found evidence for small study bias in single-city mortality studies and in multicity studies of cardiovascular disease.
Conclusions The consistency of the evidence for adverse health effects of short-term exposure to PM2.5 across a range of important health outcomes and diseases supports policy measures to control PM2.5 concentrations. However, reasons for heterogeneity in effect estimates in different regions of the world require further investigation. Small study bias should also be considered in assessing and quantifying health risks from PM2.5.
- COPD epidemiology
- Asthma Epidemiology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Key messages
What is the key question?
-
Is there convincing and consistent evidence worldwide that short-term exposure to outdoor fine particulate matter (particles with a median aerodynamic diameter <2.5 μm (PM2.5)) air pollution is associated with increased risk of death and emergency admission to hospital?
What is the bottom line?
-
We found evidence for adverse health effects of short-term exposure to PM2.5 across a range of important health outcomes, diseases and age groups with substantial variation between different regions of the world that needs explanation.
Why read on?
-
Our study provides a systematic, quantitative summary of the time series literature and reports new findings that suggest larger associations for respiratory causes of death than for cardiovascular causes and that the presence of publication bias in the literature could have important implications for public health policy.
Introduction
The adverse health effects of exposure to outdoor particulate matter air pollution are of concern to governments and health organisations worldwide.1 ,2 The evidence for these health effects has come from studies of the clinical, mechanistic and epidemiological evidence of short-term and long-term exposures. While the epidemiological evidence relating short-term exposure to PM10 (particles with a median aerodynamic diameter <10 μm) and related metrics (black smoke, total suspended particles) with health effects is substantial, there are relatively few studies of fine particles measured as PM2.5 (particles with a median aerodynamic diameter <2.5 μm). Reviews of the evidence linking exposure to PM2.5 to adverse health effects have relied upon a small number of published studies, restricted in health outcomes and geographical coverage, or focused on differential PM2.5 toxicity.3–11
To summarise the existing evidence we conducted a comprehensive and systematic meta-analysis of time series studies of daily PM2.5 and daily mortality and hospital admissions published worldwide in the peer reviewed literature to May 2011. This included all disease outcomes for which there were sufficient studies for meta-analysis and combined results from single-city and multicity studies. We focused our analysis on single-pollutant rather than multipollutant models and upon all-year results in order to maximise the number of estimates available for inclusion in the review. We present estimates for WHO regions and assess between-region heterogeneity. We also investigate whether there is evidence of publication (small study) bias between single-city study estimates and between multicity summary estimates.
Methods
Systematic ascertainment of relevant studies
Time series (including case crossover) studies published in peer reviewed journals and indexed in online databases to May 2011 (no start date specified) were identified via search strings using terms relating to study design, pollutant and health outcomes. A sifting process identified (from study titles, abstracts and the full paper) those time series studies suitable for inclusion in the review. Study eligibility depended upon the details of the study design, statistical methods used and presentation of regression estimates and other data in numerical format. Further details are given in the online supplementary material.
Extraction and coding of data
Study details were entered into a Microsoft Access database (Microsoft Office 2010, Microsoft Corporation) and included citation information (title, authors, date of publication, etc) and details of effect estimates including health outcome (mortality or admission), diagnosis (International Classification of Diseases codes), age, and so on, and details of the pollutants (unit of measurement, range of exposure, etc). These data were used to calculate standardised effect estimates expressed as the percentage change (and 95% CI) in the mean number of daily events associated with a 10 µg/m3 increase in PM2.5 concentration. The short-term relationships between air pollution and health effects are determined for given time lags (in days) between exposure and health events and investigators vary in which lags they study and report.12 Hence an a priori lag selection protocol was devised and used to choose lag estimates for inclusion in the review without introducing bias (see online supplementary material for details). Additional data entry included the coding of the WHO region in which the study occurred (see online supplementary material, table S1). Studies were reviewed by a single statistician/epidemiologist before coding. All papers were read by RWA and data range checked prior to meta-analysis.
Meta-analysis
In the time series literature many cities have been studied on more than one occasion, in single-city studies and as part of a larger, coordinated multicity investigation. To ensure results from a city only appeared once in any one meta-analysis we applied an a priori estimate-selection protocol (see online supplementary material for details).
We conducted meta-analyses only if there were 4+ single city estimates or if the set of estimates contained a multicity study summary estimate. Within each WHO region we conducted a two stage meta-analysis using a random-effects model for each stage.13 In the first stage, single-city estimates were pooled to provide a summary estimate of the evidence from single-city studies. In the second stage, these summary estimates were pooled with the selected multicity study estimates to obtain a WHO region-specific summary estimate of the evidence. To assess heterogeneity between WHO regions we used the I2 statistic which indicates the proportion of total variability between effect estimates due to heterogeneity.14 I2 statistics in the range 0 to 30, 30 to 50 and >50 generally indicate low, moderate and high heterogeneity, respectively. Finally, a global summary estimate was calculated from WHO region-specific single-city summary estimates and multicity study estimates.
Assessment of small study bias
We investigated our selected single-city estimates and our pooled single-city and selected multicity estimates for evidence of small study bias using the methods of Begg and Egger.15 ,16 The former uses an adjusted rank correlation method to examine the association between study estimates and their variance whereas the latter uses a regression approach. The impact of adjustment for small study bias was assessed using the ‘trim and fill’ method.17 This method removes studies until symmetry in the funnel plot is achieved, recalculating the centre of the funnel before the removed studies are replaced together with their ‘missing’ mirror-image counterparts. A revised summary estimate is then calculated using all of the original studies, together with the hypothetical ‘filled’ studies. Our overall assessment of the evidence for small study bias was based upon the combined evidence presented by all three techniques.
All analyses were conducted in STATA (STATA/SE V.10, StataCorp Texas).
Results
One hundred and ten time series studies of daily mortality (68) and hospital admissions (54) indexed in medical databases to May 2011, and providing numerical effect estimates, reported results for PM2.5 (see online supplementary material, table S2). Table 1 details the number of studies tabulated by outcome, disease, WHO region, age group and multicity versus single-city study design. The majority of studies of PM2.5 and daily mortality and hospital admissions have been conducted in North America and Europe with a small number of studies in other regions of the world. The most frequently reported estimates for daily mortality were for the all-ages group, followed by the 65 + years group. For most populations the latter comprised a large proportion of the all-ages group so we confined our mortality analyses to the all-ages group. For hospital admissions we focused upon age-specific estimates in children and the elderly (ages 0–14 years and 65+ years, respectively). While the majority of studies were conducted in single cities, a substantial number reported findings from multicity studies.
Time series studies of PM2.5 and mortality and hospital admissions
Mortality
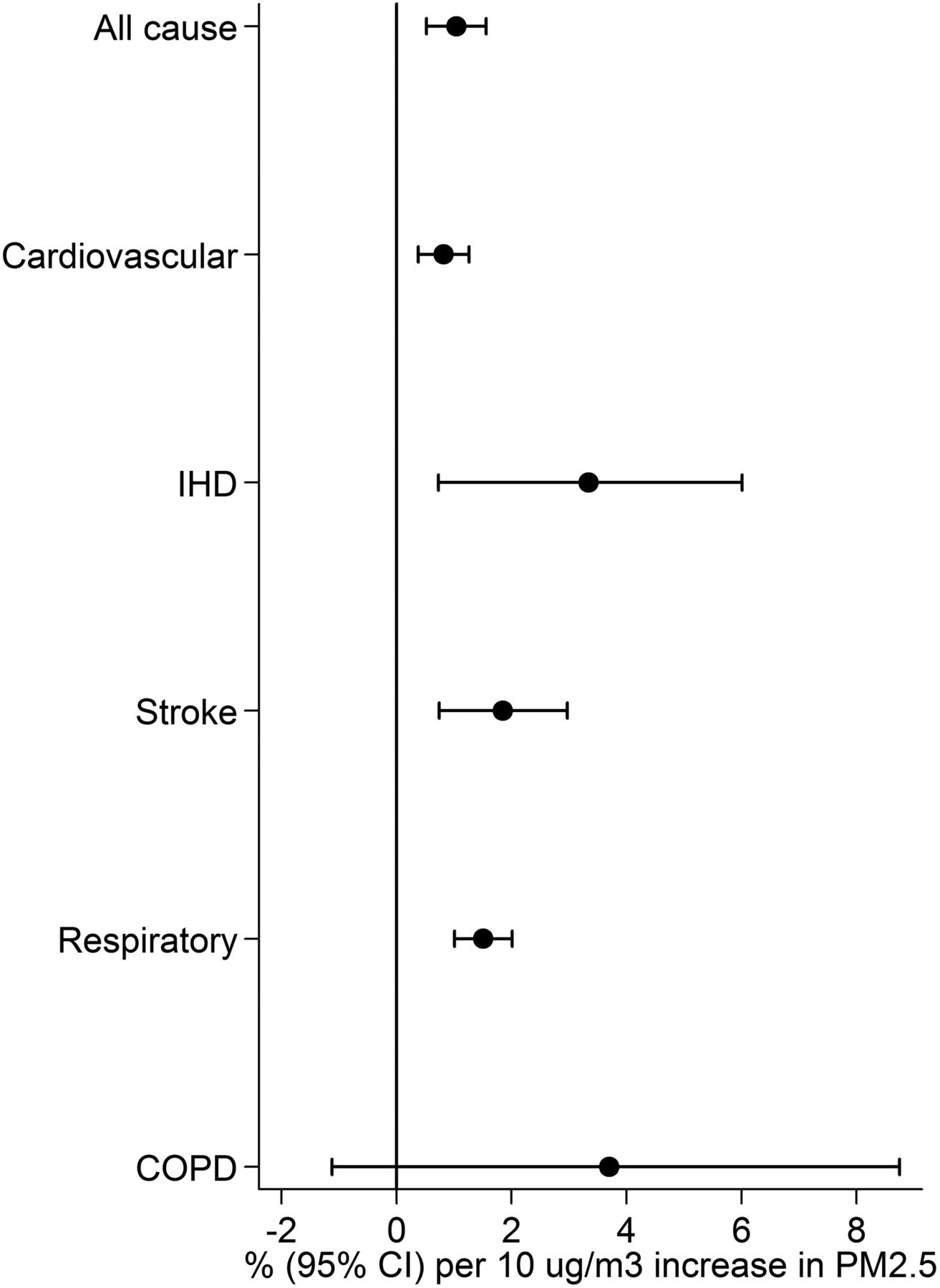
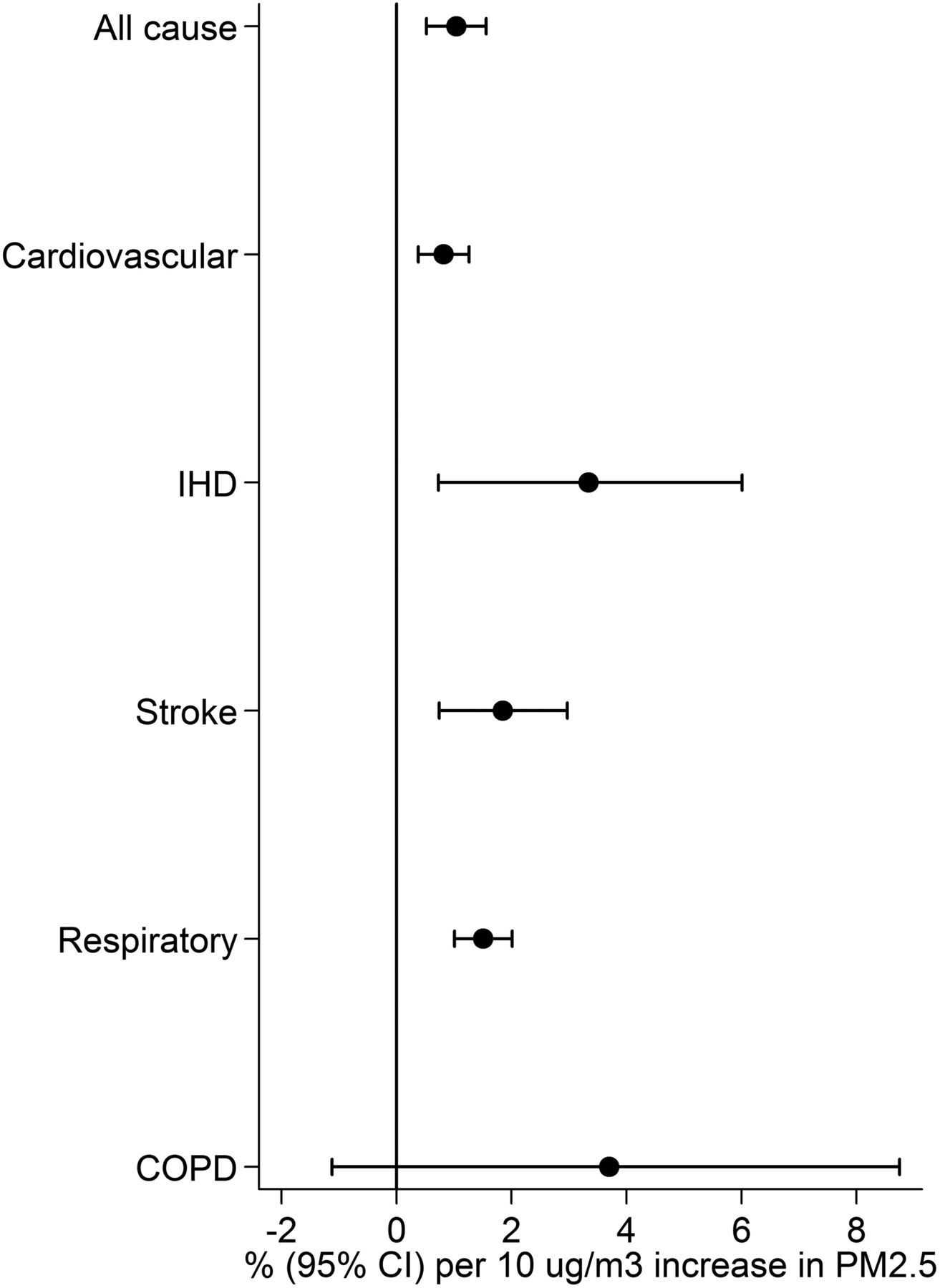
Summary estimates (95% CIs) per 10 µg/m3 increment in PM2.5 and all-age, all-cause and cause-specific mortality are presented in figure 1. All associations were positive and for all, except chronic COPD, lower CIs were above unity. For all-cause mortality, 23 single-city and multicity study estimates were selected for meta-analysis from the 43 estimates identified in the review (see online supplementary material, figure S1). The overall random effects summary estimate was 1.04% (95% CI 0.52% to 1.56%) per 10 µg/m3 increment in PM2.5. WHO region-specific summary estimates varied substantially (I2=93%) from 0.25% to 2.08% (table 2).
Meta-analysis results for all-age, all-cause mortality and cause-specific mortality by WHO region
Summary estimates (95% confidence intervals) for all-cause and cause-specific mortality.
While fewer estimates were available for cardiovascular (see online supplementary material, figure S2) and respiratory (see online supplementary material, figure S3) mortality, the overall summary estimate for all respiratory causes of death was larger than for all cardiovascular causes, 1.51% (95% CI 1.01% to 2.01%) versus 0.84% (95% CI 0.41% to 1.28%), respectively. For both causes of death, associations were positive in all WHO regions (table 2) and heterogeneous for cardiovascular deaths (I2=76%) but not respiratory deaths (I2=0%). Associations between PM2.5 and death from ischaemic heart disease, stroke and COPD were 3.36% (0.68%, 6.10%), 1.85% (0.74%, 2.97%) and 2.86% (−0.12%, 5.93%) per 10 µg/m3, respectively, although the evidence was restricted to a small number of single-city and multicity studies (see online supplementary material, table S3 and figures S4–S6).
Hospital admissions
Table 3 gives summary estimates for all-age, cardiovascular and respiratory causes of hospital admissions with individual study results presented in online supplementary material, figures S7 and S14.
Meta-analysis results for all-age, cardiovascular and respiratory hospital admissions by WHO region
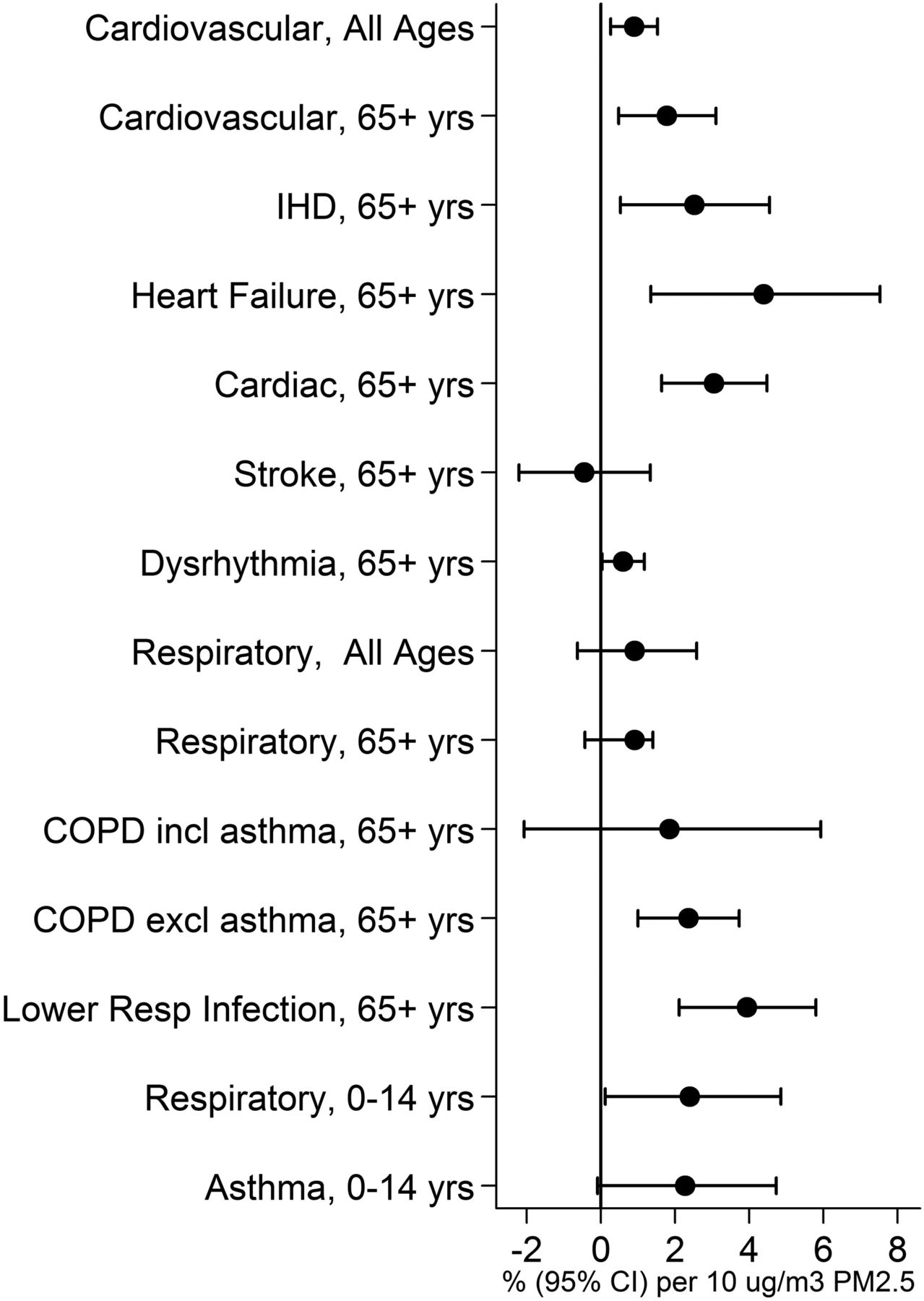
PM2.5 concentrations were positively associated with increases in risk of admission for cardiovascular diseases, 0.90% (95% CI 0.26% to 1.53%) and respiratory diseases, 0.96% (95% CI −0.63% to 2.58%) per 10 µg/m3, respectively, with heterogeneity between WHO regions for respiratory diseases (I2=80%) but not cardiovascular diseases (I2=0%). Figure 2 illustrates summary estimates for specific cardiovascular diseases in ages 65+ years and for respiratory diseases in ages 65+ years and children aged 0–14 years. All associations were positive except for stroke and for all, except COPD including asthma, lower CIs exceeded 0%. Details of WHO-specific summary estimates are given in online supplementary material, tables S4 and S5, and study-specific estimates in online supplementary material, figures S7–S13 and S15–S20.
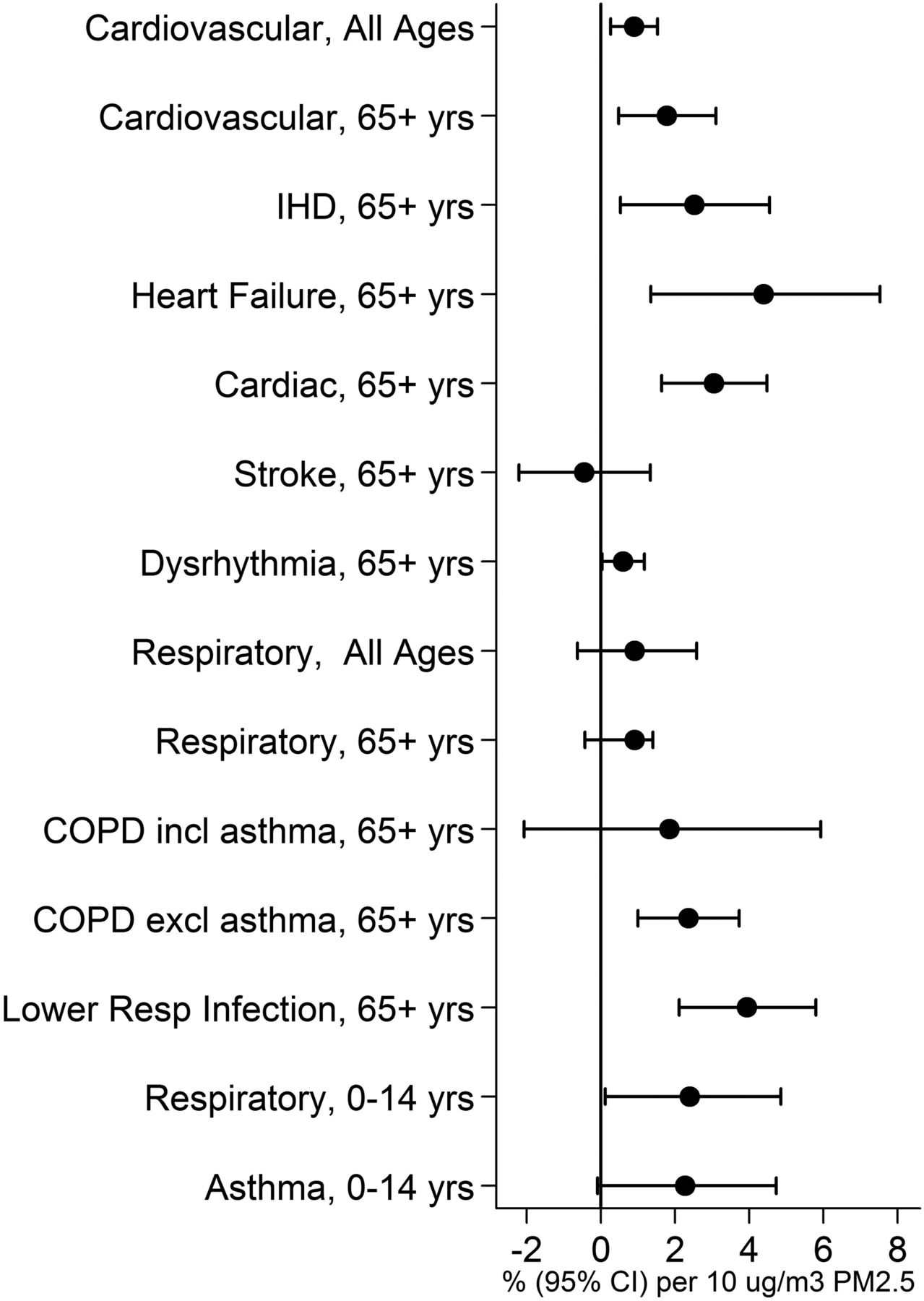
Summary estimates (95% confidence intervals) for cardiovascular and respiratory hospital admissions.
Small study bias
The impact of adjustments for small study bias in single-city studies within WHO regions and between the pooled single-city and multicity estimates for all-age, all-cause and cause-specific mortality are shown in table 4. We found evidence for small study bias in single-city mortality studies and in multicity studies of cardiovascular disease.
Assessment of bias in single-city studies and in pooled estimates for all-cause mortality and cause-specific mortality
Figure 3 illustrates, for cardiovascular mortality, this adjustment using a funnel plot of individual study estimates and showing the random effects summary estimates with, and without, inclusion of the two ‘filled’ estimates identified by the ‘trim and fill’ procedure. We did not find evidence of small study bias in either single-city or multicity estimates for cardiovascular or respiratory hospital admissions (data not shown).

{kind=link}
{kind=link}
{kind=link}
Funnel plot of pooled single-city and multi-city summary estimates for cardiovascular mortality including ‘filled’ estimates. Random effects summary estimates without (long-dash line) and with (short-dash line) adjustment using the Trim & Fill procedure.
Discussion
In this systematic review we identified 110 ecological time series studies of short-term exposure to outdoor PM2.5 and daily mortality and hospital admissions indexed in medical databases up to May 2011. Our meta-analysis of effect estimates from these studies indicated positive associations with daily all-cause and cause-specific mortality and cause-specific and age-specific hospital admissions, with some evidence of heterogeneity. We also found evidence for small study bias in single-city estimates and between pooled and multicity estimates.
There are a number of plausible biomedical explanations for associations between short-term exposure to fine particles and adverse health outcomes.5 ,6 It is hypothesised that small effects cause clinical events when experienced by individuals who are already vulnerable due to existing chronic or acute disease. Our review indicates that such effects are observed even at the relatively low levels of fine particles found in developed countries. Our results reinforce the public health importance of fine particles on health. While the estimates are small, the impact is substantial because the entire population is exposed. Impact assessments of PM2.5 on mortality are based on cohort rather than time-series evidence because this enables years of life lost to be estimated.18 ,19 However, most cohort evidence is from North America or Western Europe. Our finding that short-term associations occur worldwide supports the generalisation of cohort based estimates globally19 while at the same time indicating that there may also be some heterogeneity.
Our study extends the literature reviewing the evidence for health effects of short-term exposure to PM2.5 derived from time series studies. The numbers of single-city and multicity studies have increased substantially in recent years, from 55 in 200511 to 110 identified in this review. In 2009 the Environmental Protection Agency (EPA) summarised evidence from studies of mainly US populations5 published between 2002 and May 2009. Also in 2009, the American Heart Association issued an updated statement on the effects of particulate air pollution on cardiovascular disease including evidence from time series studies published to March 2009.6 A more recent review in 20128 focused upon studies of PM2.5 components indexed in the Science Citation Database up to October 2010. Our study complements these previous reviews by providing a meta-analysis for a much larger, more recent (indexed in medical databases to May 2011) and broader literature incorporating studies irrespective of geographical location and disease outcome.
Across the five WHO regions studied, our summary estimates for all-age, all-cause mortality ranged from 0.25% to 2.08% with an overall estimate of 1.04%, comparable with the summary estimate of 1.2% derived from seven studies by Levy et al.8 While we found evidence of statistical heterogeneity across region-specific estimates both values are consistent with a mortality hazard from short-term exposure to fine particulate matter. The reasons for this variability in effect estimates between WHO regions warrant further investigation but may reflect variations in population vulnerability and/or differential toxicity of sources, pollutant mixtures and pollution monitoring.
Our finding that the association for respiratory mortality (1.51%) was larger than for cardiovascular mortality (0.84%)—a finding observed within all WHO regions—was also reported by the EPA in their review.5 However, the EPA noted the coherence in associations between PM2.5 and cardiovascular mortality and morbidity outcomes and the lack of such coherence for respiratory diseases. We were only able to assess the extent of coherence by comparing associations for mortality and admissions. For cardiovascular diseases our overall summary estimates for PM2.5 and admissions and mortality were comparable confirming the coherence reported by the EPA although we note substantial disagreement between region-specific summary estimates for each outcome including North America. We also note the negative, although statistically not significant, associations observed in three single-city studies in Europe and the Western Pacific region for hospital admissions for stroke in adults over the age of 65 years. For respiratory diseases, we found that the overall summary estimates for PM2.5 and mortality and admissions were broadly comparable although for respiratory admissions the summary estimate was approximately two-thirds that for mortality and the CI for the summary estimate straddled 0% due to the negative association reported in a single-city study from North America. We note however that while the same ICD codes are used for mortality and admissions, the way they are used is different—underlying cause of death for the former and immediate cause of admission for the latter. This might affect comparability of certain categories such as pneumonia or heart failure though they would still fall within the broad cardiovascular or respiratory rubric.
The main strengths of our study are: (1) a protocol driven approach to the identification, coding and selection of effect estimates for meta-analysis to minimise selection bias throughout the review process; (2) inclusion of all health outcomes for which sufficient estimates were available for meta-analysis; (3) no limitations on study location or language, and (4) stratification of results by WHO region. However, in common with other reviews, our study is limited by: (1) the need for numerical, rather than graphical, presentation of data to facilitate quantitative meta-analysis; (2) the authors’ choice of results to publish; and (3) having no assessment of the ‘grey’ literature. It is therefore important to assess the extent to which the inferences and quantitative estimates presented here have been affected by small study bias, a process that leads to the published literature being unrepresentative of the totality of evidence.20
Our analysis of small study effects, a generic term also encompassing publication bias and a range of other potential biases,21 suggests that this may be an important issue in the meta-analysis of single-city and multicity estimates. The former has been noted previously in relation to time series studies of PM1011 but the observation that meta-analysis of multicity estimates can be similarly affected is new. Sterne et al suggested that the greater investment of time and money in larger studies (such as multicity time-series studies) meant such studies would be more likely to be of high methodological quality and published even if their results are negative.21 Sterne et al also noted that the ‘trim and fill’ procedure detects ‘missing’ studies in a substantial proportion of meta-analyses, even in the absence of bias. Thus, there is a danger that the application of the procedure could mean adding and adjusting for non-existent studies in response to funnel plot asymmetry arising from nothing more than random variation. Our finding that the ‘trim and fill’ adjustment substantially reduced the magnitude and precision of the associations between PM2.5 and cardiovascular mortality should therefore be interpreted with some caution, especially so given the unremarkable p values from the Begg and Egger tests and the funnel plot presented in figure 3.
Other potential sources of bias in our study methodology could be: (1) the selection of estimates from the individual papers; and (2) the selection of study estimates for meta-analysis. Bias arising from the former is possible given the tendency of investigators to assess associations at different time lags between exposure and health event. To address this we used a protocol for estimate selection that was independent of the direction of an association. In previous work this has been shown not to introduce bias but increase between-estimate heterogeneity11 so we believe that it is unlikely that we are overstating the magnitude of associations. Our protocol for the selection of estimates (from those available) for meta-analysis similarly did not consider direction of associations, instead basing the selection upon geographical coverage, publication date and length of study period. It also ensured that no single location appeared more than once in a summary estimate. While our approach was just one of many analytical strategies that could have been adopted, we believe that the resulting summary estimates were unlikely to be systematically biased since none of our selection criteria included the direction or magnitude, of the individual study effect estimates. The relevance of these issues cannot be overstated since results from meta-analyses can be important in underpinning the use of more limited cohort data in worldwide health impact assessments.19
Our review points to adverse associations between short-term exposure to daily concentrations of PM2.5 and daily mortality and hospital admissions across a range of diseases and age groups which supports continued policy measures to control PM2.5 levels worldwide. However, we note that the evidence for these associations is concentrated in a small number of geographical regions of the world and also limited to the broader categories of disease. Further studies from other developed countries, in particular Asia and Eastern Europe, are needed to confirm the observed associations. Also, new studies including specific, rather than broad, categories of diseases would increase understanding of the populations at risk and may also add to our understanding of mechanism of effect. In addition, the reasons for the heterogeneity in effect estimates in different regions of the world require further research as they may be relevant to the formulation of policy measures. Our findings also suggest that, for the purpose of health impact assessment, some consideration of, and adjustment for, small study bias in results from multicity as well as single-city studies should be undertaken.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Acknowledgements This is independent research commissioned by the Policy Research Programme in the Department of Health. The views expressed are not necessarily those of the Department.
-
Contributors All authors contributed to the design of the study and to the drafting of the paper and have seen and approved the final version. Data analysis was carried out by RWA.
-
Funding Policy Research Programme in the Department of Health (002/0037).
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.