Article Text

Abstract
Background Atypical carcinoids (AC) of the lung are rare intermediate-grade neuroendocrine neoplasms. Prognostic factors for these tumours are undefined.
Methods Our cooperative group retrieved data on 127 patients operated between 1980 and 2009 because of an AC. Several clinical and pathological features were studied.
Results In a univariable analysis, T-status (p=0.005), N-status (p=0.021), preoperative M-status (previously treated) (p=0.04), and distant recurrence developed during the outcome (p<0.001) presented statistically significant differences related to survival of these patients. In a multivariable analysis, only distant recurrence was demonstrated to be an independent risk factor for survival (p<0.001; HR: 13.1). During the monitoring, 25.2% of the patients presented some kind of recurrence. When we studied recurrence factors in a univariable manner, sublobar resections presented significant relationship with locoregional recurrence (p<0.001). In the case of distant recurrence, T and N status presented significant differences. Patients with preoperative M1 status presented higher frequencies of locoregional and distant recurrence (p=0.004 and p<0.001, respectively). In a multivariable analysis, sublobar resection was an independent prognostic factor to predict locoregional recurrence (p=0.002; HR: 18.1).
Conclusions Complete standard surgical resection with radical lymphadenectomy is essential for AC. Sublobar resections are related to locoregional recurrence, so they should be avoided except for carefully selected patients. Nodal status is an important prognostic factor to predict survival and recurrence. Distant recurrence is related to poor outcome.
Statistics from Altmetric.com
Key messages
What is the key question?
-
What clinical factors are affecting prognosis in atypical carcinoids of the lung, related to survival and recurrence?
What is the bottom line?
-
Complete lobar surgical resection, N and M status remain as main behaviour markers.
Why read on?
-
Although there is no consensus about what prognostic marker should be observed, our series is probably one of the largest series published to date about this infrequent tumour.
Introduction
Atypical carcinoids (ACs) of the lung are rare intermediate-grade neoplasms which are part of a wide spectrum of neuroendocrine tumours ranging from the typical carcinoid to small cell lung carcinoma. Although this type of neoplasm can be found throughout the body, the bronchial tree is the most frequent location for approximately 25% of carcinoid tumours.1
In 1998, Arrigoni's2 long-standing histological criteria for the diagnosis of AC (presence of five or more mitoses in 2 mm2 or focal necrosis)2 were modified by Travis and colleagues and then accepted by WHO and the International Association for the Study of Lung Cancer (IASLC) in 1999. Atypical carcinoid was thence defined as a tumour with neuroendocrine morphology and mitotic counts of two or more and less than 10 per 2 mm2 of viable tumour (10 high-power fields), or the presence of punctate foci of coagulative necrosis.3 Large areas of geographic necrosis typical of high-grade neuroendocrine carcinomas are not seen.4
Although the aggressive behaviour of AC is well known, factors predisposing to poor prognosis are uncertain. Regional disease with spread to local lymph nodes occurs frequently in AC tumours. Published studies related a variable rate of lymph node disease of anywhere from 20% to 60% of cases.5–7 Nevertheless, the main prognostic factors in these neoplasms are undefined in the literature. We present our experience in this kind of neuroendocrine tumours.
Material and methods
The Spanish Multicenter Study of Neuroendocrine Tumours of the Lung (EMETNE is the Spanish acronym) is a cooperative multicenter group composed of 26 hospitals throughout Spain. All resected neuroendocrine lung tumours at any of the participating institutions from 1980 were registered and classified into one of the following categories: typical carcinoid, AC, large cell neuroendocrine carcinoma (LCNEC), and small cell lung carcinoma. We collected 127 AC tumours that were operated between 1980 and 2009. Before 1998, cases were retrieved retrospectively. From 1998, new cases were collected in a prospective manner. Local lung pathologists reviewed all samples to classify them following the 1999 WHO classification, including Travis's new criteria for AC. Patients underwent complete surgical resection of the tumour in all cases. From 1980 to 1997, a mediastinal lymph node sampling was associated. In the prospective group, systematic nodal dissection was carried out.
We studied clinical behaviour in these tumours, analysing prognostic significance and patterns of nodal affection and recurrence. Clinical variables considered were: age, gender, location of the tumour, size, surgical procedure and nodal status using the tumour-node-metastasis (TNM) classification.8 Histological feature variables were: tumour differentiation, tumour pattern, angio-lymphatic invasion and immunohistochemical markers (chromogranin, synaptophysin and neuron-specific enolase in all cases). The resection extent was also studied, dividing the series into lobar resections (LR) (lobectomy, bi-lobectomy and pneumonectomy) and sublobar resections (SR) (segmentectomy and isolated bronchial resection), as well as adjuvant treatment (chemotherapy (ChT), and radiotherapy (RT)). Survival analysis data were collected from a systematic follow-up database. Local recurrence and distant metastasis were also assessed.
Statistical analysis was carried out using a SPSS V.19.0 statistical package programme. Categorical variables were compared using χ2 test. Mean differences were assessed using t test or analysis of variance. Cumulative survival probabilities were estimated by the Kaplan–Meier test. A multivariable analysis was performed in order to determine prognostic factors using linear regression or Cox's regression. A p value of <0.05 was considered significant.
Results
From the 1082 patients affected by a neuroendocrine lung tumour registered in our database in December 2009, 127 corresponded to an AC. These represent 11.7% of total cases. Demographics and clinical features are given in table 1. Bronchoscopy was the main diagnostic procedure. In 72 cases (56.7%), the tumour was visualised endoscopically. Bronchial biopsy was diagnostic in 41 cases (32.3%). Nevertheless, surgery was necessary to obtain the definitive diagnosis of AC in 45 patients (35.3%). Seventeen of these 45 cases were central tumours and another 28 cases were peripheral tumours.
Demographics and clinical characteristics
In all, 77 lobectomies (60.65%), 12 bi-lobectomies (9.4%) and 22 pneumonectomies (17.3%) were performed. Bronchoplastic procedures were associated in 6 cases (4.7%): 4 sleeve lobectomies and 2 isolated bronchial resections. In 16 patients (12.6%), SRs were carried out: 14 wedge resections and the 2 bronchial resections mentioned previously. There was no postoperative mortality in the series. Mean tumour size was 32.38 mm (SD: 16.170; range 9–99 mm). Pathological features are described in table 2. Thirty-five cases (27.6%) were pT1 tumours, 81 (63.8%) pT2, 6 (4.7%) pT3 and 5 were (3.9%) pT4. Forty-three patients (33.9%) presented some kind of nodal affection: 18 pN1 (14.2%), 24 pN2 (18.9%) and 1 pN3 (0.86%). From these N+ patients, eight cases were classified as T3 or T4 tumours (table 3).
Pathological features
T-staging in N+ cases
Multimodal therapy after surgery was indicated in an individualised manner. Eighteen patients underwent any kind of adjuvant treatment (11 ChT, 6 RT and 3 ChT-RT). Four patients of this group were N0 (3 ChT because of the size of the tumour (larger than 7 cm, cT3) and 1 RT because of sublobar resection). Fourteen of these patients were classified as N+.
Thirty-two out of 127 patients (25.2%) presented some kind of recurrence during the outcome: 5 corresponded to locoregional recurrences (3.9%), 22 were distant metastasis (17.3%) and 5 patients had both types (3.9%). The most prevalent location for locoregional recurrence was mediastinal lymph nodes, while the liver was the most typical location for distant metastasis.
Twenty-three patients died during monitoring, 12 because of the tumour and 11 from other causes (not attributable to tumour progression). Median survival for death from any cause in the AC follow-up was 47 months. Five-year overall survival rate in AC was 80%. None of the pathological tumour characteristics (differentiation grade, tumour pattern, bone metaplasia and immunohistochemical markers) were found to be significant for survival influence. In a univariable analysis, T-status categories presented statistical signification related to survival of these patients (p=0.005). As to the prognostic significance of nodal disease in survival of patients affected by AC, 5-year survival for N0, N1 and N2 cases was 88%, 68% and 64%, respectively. We discarded the only N3 case for prognostic analysis. When we compared N0 survival with N+ survival in these patients, differences observed were statistically significant (p=0.021) (figure 1). In the N+ patients, there were no statistical differences in survival or recurrence between patients receiving or not receiving adjuvant treatment. Six patients presented solitary M1 disease at the time of lung surgery (metastatic tumour was previously curatively treated). These M1 patients had a significantly worse survival prognosis than the M0 (estimated mean survival time 171.3 months in M0 group vs 73.7 months in M1 group; p=0.040) (table 4).
Kaplan–Meier univariable survival analysis
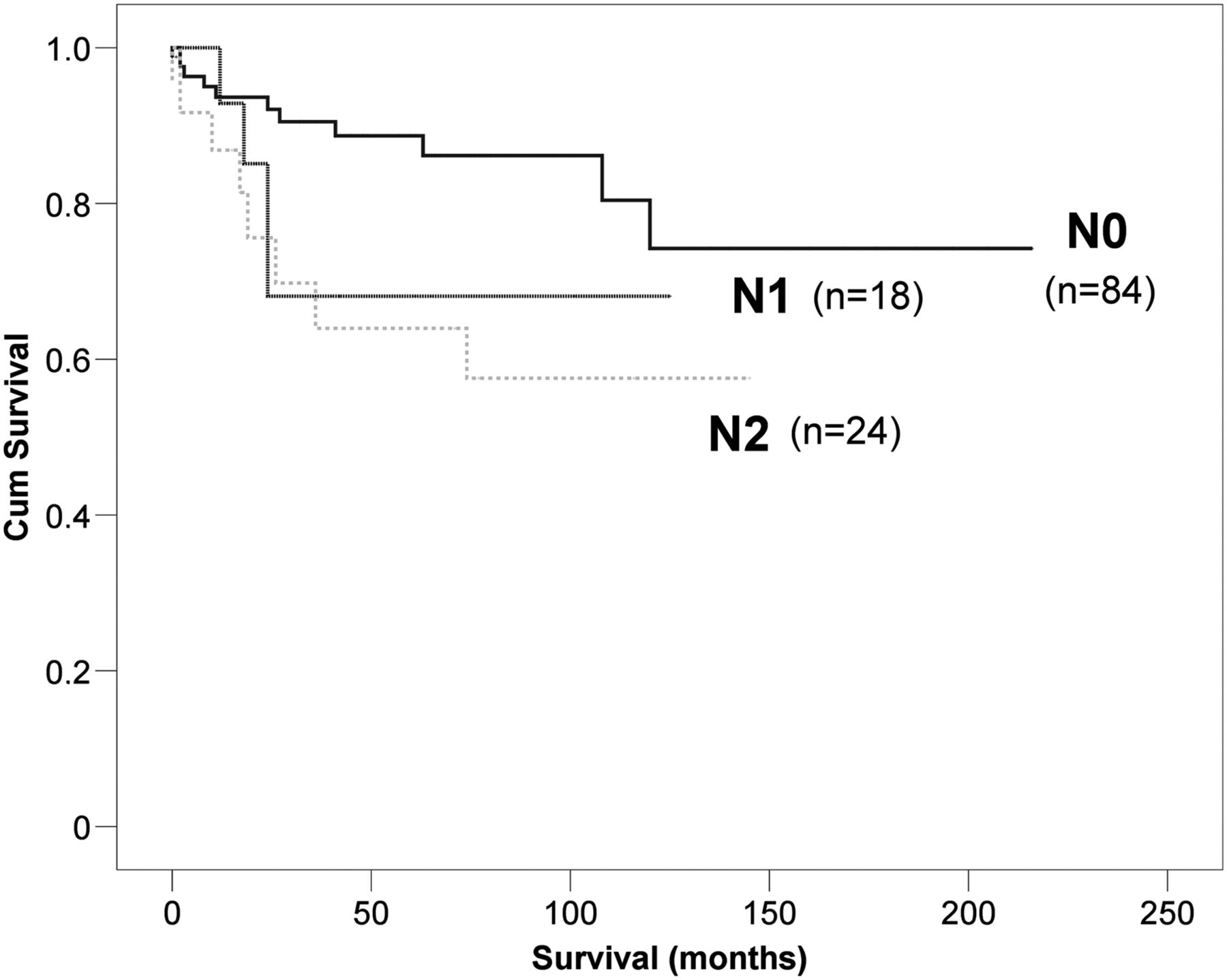
Prognostic influence of N-status in atypical carcinoid. Univariable analysis (Kaplan–Meier) (p=0.049).
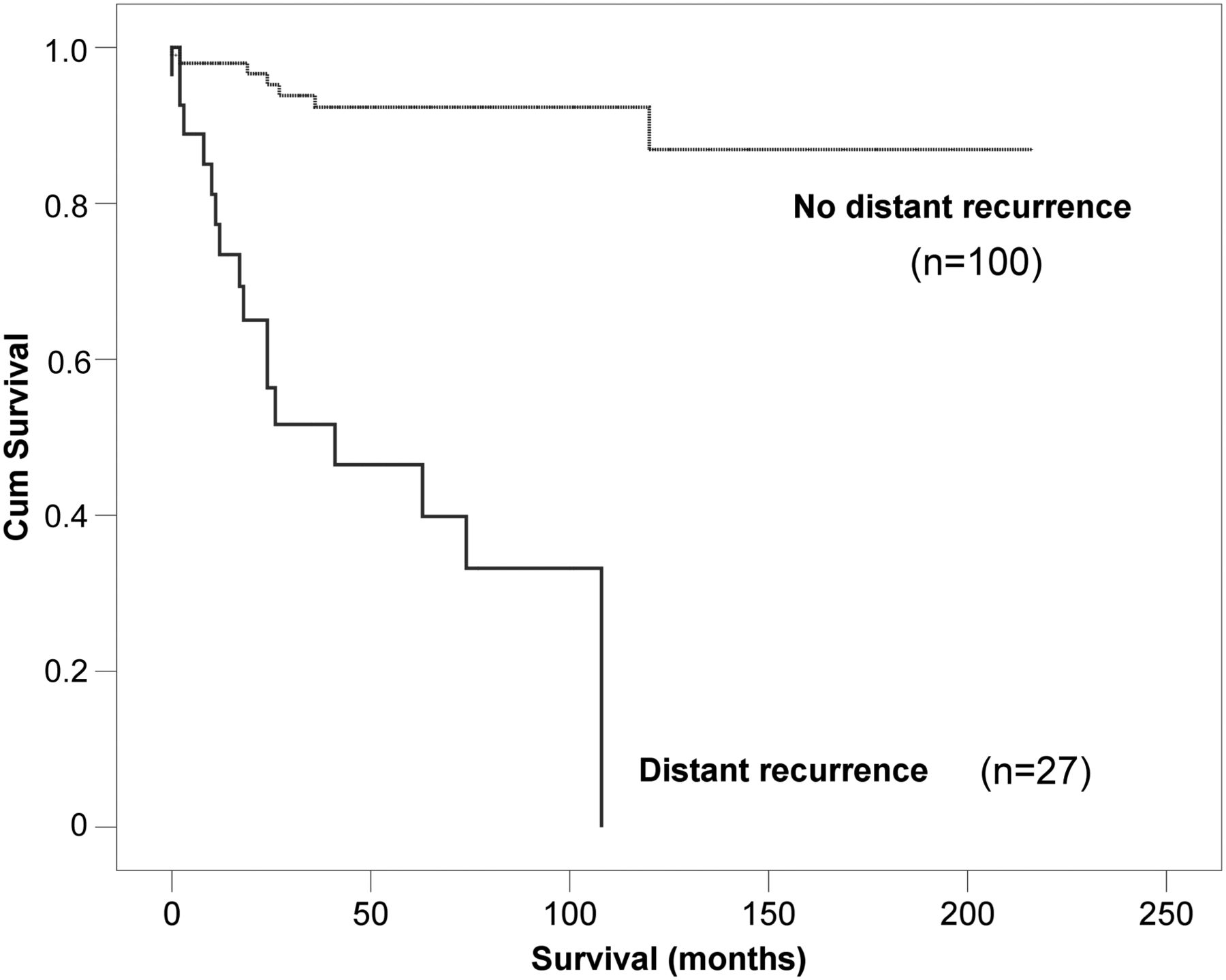
Recurrence also affected survival adversely. When we studied the prognostic behaviour of patients presenting locoregional recurrence, we found clinical differences. Estimated mean survival time for locoregional recurrence was 90.4 months (95% CI 63.2 to 117.6), against 169.4 months for patients without locoregional recurrence (95% CI 150.8 to 188.0). However, this difference was not statistically significant (p=0.435). Patients who developed distant metastasis during follow-up presented significantly poorer survival than those who did not (p<0.001) (figure 2), presenting a 5-year survival rate of 39%. Median survival time for distant disease, locoregional disease and recurrence-free patients was 38, 114 and 180 months, respectively. In a multivariable analysis, the development of distant recurrence was demonstrated as the main independent risk factor for survival of these patients (p<0.001; HR=13.095; 95% CI for HR: 5.048 to 33.974).

Prognostic influence of distant metastasis during the outcomes. Univariable analysis (Kaplan–Meier) (p<0.001).
Recurrence relationship between type of resection practiced and recurrence was assessed. We observed that patients who underwent SR developed locoregional recurrence more frequently (6 patients; 37.5%) than those who received LR (4 patients; 3.9%) (p<0.001) (figure 3). Ninety-eight percent of patients who underwent LR were free of locoregional recurrence 2 years after surgery (71% for the SR group).

Influence of the extent of resection in locoregional recurrence. Univariable analysis (Kaplan–Meier) (p<0.001).
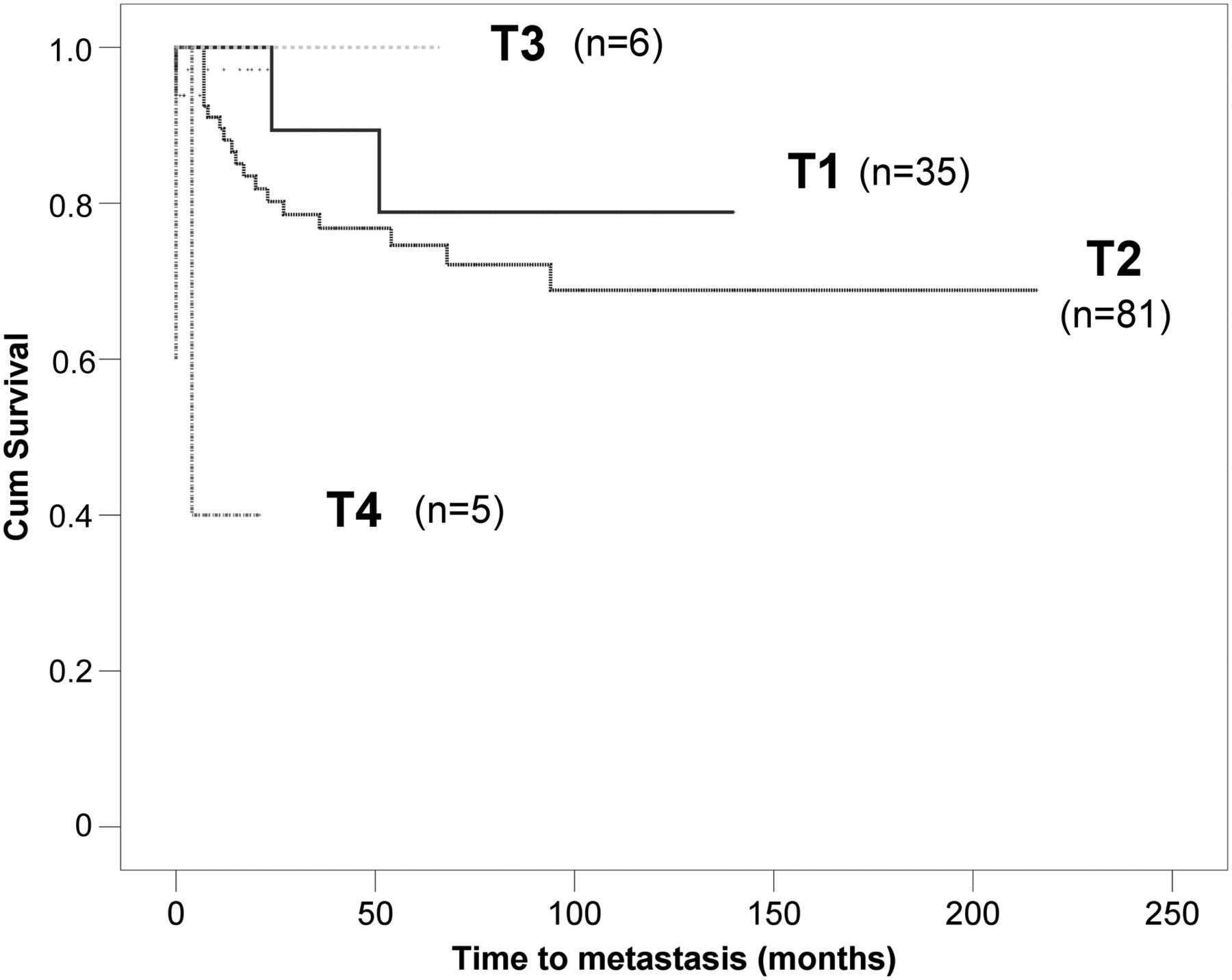
When analysing distant recurrence, tumour size according to TNM system cut-off presented clinical differences in this aspect, but without statistical significance (p=0.550), possibly due to sample size. With respect to distant recurrence, T-status did present statistical differences related to the time to metastasis in the univariable recurrence analysis (p<0.001) (figure 4).
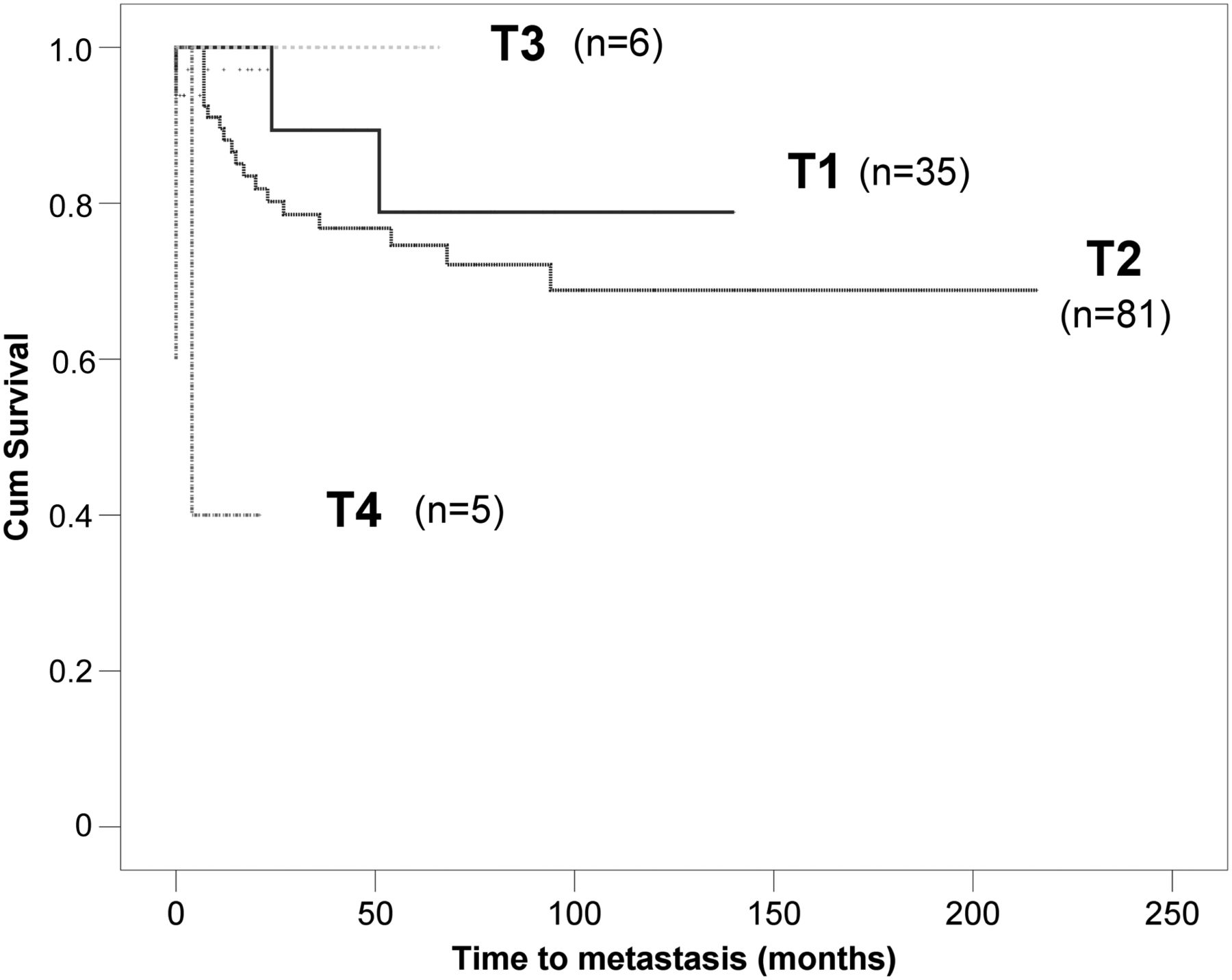
Influence of T-status in distant recurrence. Univariable analysis (Kaplan–Meier) (p<0.001).
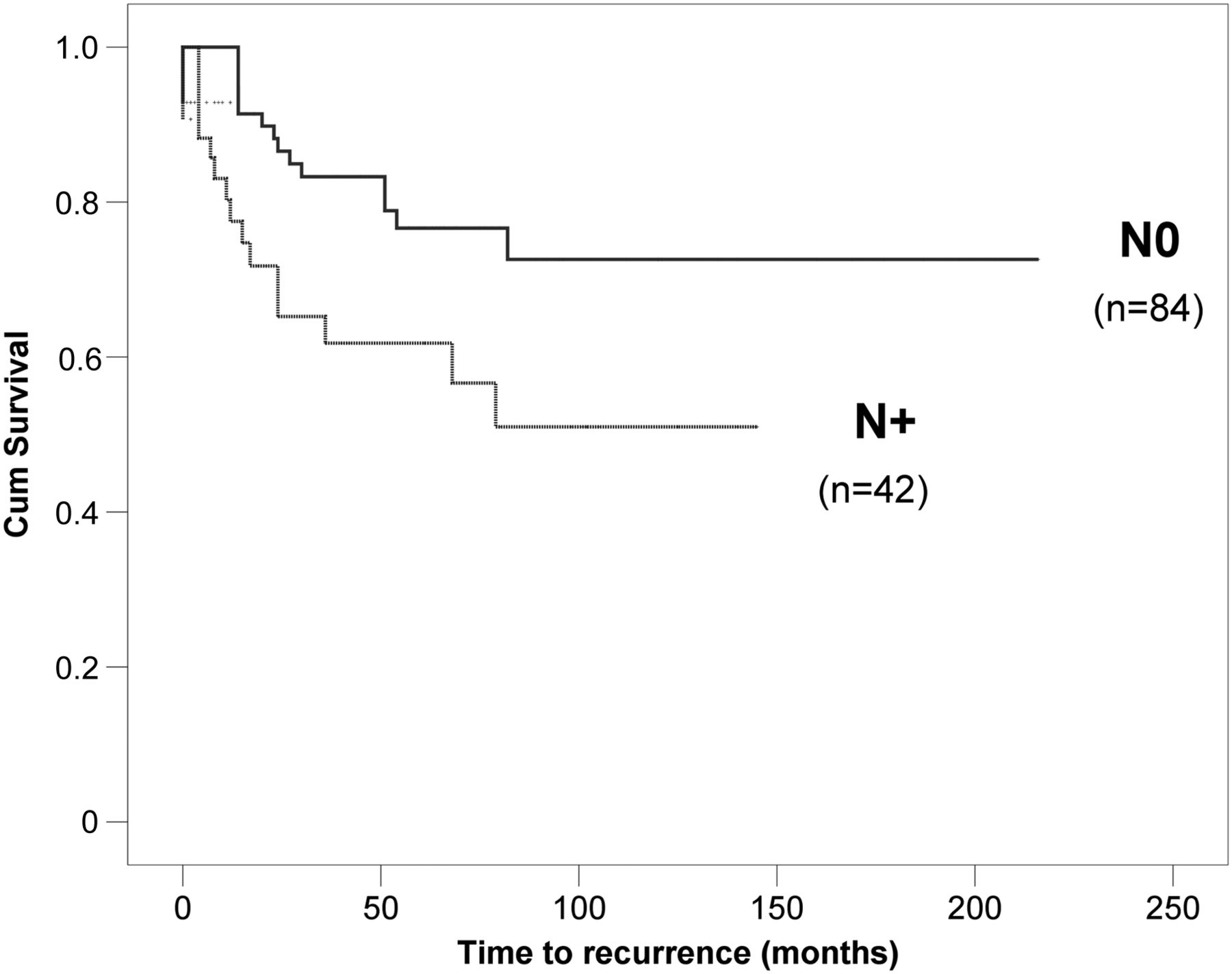
Another important topic is the relationship between nodal invasion and recurrence. We observed that the higher the N-status of the patient, the higher the frequency of distant metastasis (16.7%, 27.8% and 33.4% for N0, N1 and N2, respectively). For locoregional recurrence, differences were not so important, perhaps because of the few cases collected for this group (7.1%, 5.5% and 8.3% for each step of N-status). Although we could not demonstrate statistical signification for these clinical differences (p=0.961 for locoregional recurrence and p=0.154 for distant metastasis), we found significant differences between N0 and N+ patients when considering any kind of recurrence (locoregional and/or distant) (p=0.019) (figure 5). In fact, when we analysed the frequency of locoregional recurrence between the LR group and the SR, stratifying data by N-status, we could confirm statistical differences (p<0.001). The estimated mean for time to locoregional recurrence in N0 patients was 204.33 months (95% CI 187.92 to 220.74) for the LR and 83.82 months (95% CI 59.99 to 107.65) for the SR group; in N+ patients, it was 131.98 months (95% CI 115.14 to 148.82) for the LR group, and 57.14 months (95% CI 30.37 to 83.92) for the SR group. We did not find any differences for the case of distant recurrence in this aspect. Finally, patients classified as M1 (preoperatively treated tumours) at the time of lung surgery, presented shorter locoregional (p=0.004) and distant (p<0.001) recurrence-free intervals than M0 cases (estimated mean for time to locoregional recurrence of 195 months in M0 patients vs 44.8 months in M1 patients; 168 months vs 14.5 months, respectively, for the time to distant recurrence).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Influence of nodal affection in global recurrence (locoregional and/or distant). Univariable analysis (Kaplan–Meier) (p=0.019).
In a multivariable analysis, SR was considered as an independent prognostic factor to predict locoregional recurrence in these patients (p=0.002; HR=18.111; 95% CI for HR: 2.893 to 113.362).
Finally, the prognostic effect of adjuvant ChT was analysed. Patients who underwent adjuvant ChT did not present any statistical differences regarding survival and recurrence (p=0.327 and p=0.294, respectively) (table 4). At any rate, adjuvant treatment was infrequent and varied considerably, so it is difficult to arrive at any further conclusions.
Comment
Atypical carcinoid represents an infrequent lung neoplasm, included in the neuroendocrine spectrum and defined by Travis’3 modified histological criteria. The criteria for diagnosis of AC includes the existence of 2–10 mitoses per 2 mm2 area, or the presence of small punctuate foci of necrosis. Additionally, nucleoli can be seen in AC.9 Recently, the seventh edition of the Union for International Cancer Control/American Joint Committee on Cancer TNM system has been recommended for the classification of pulmonary carcinoid tumours.8 Frequency ranges for AC reported in the literature vary from 14% to 33% of carcinoid tumours,10–13 which is consistent with our data. Almost one-third of patients remain asymptomatic at the moment of the diagnosis,14 which agrees with our observations. Accepting these facts, although many AC characteristics are known, the role of prognostic factors is not completely defined.
Intermediate prognosis in AC has been described for many years. Garcia-Yuste and colleagues,10 Cardillo and colleagues15 and Filosso and associates16 reported an improved prognosis of N0 patients compared to N+ cases. Stamatis and colleagues17 reported a high frequency of nodal hilar and mediastinal metastases in AC, but they did not indicate any prognostic factors for this kind of neuroendocrine neoplasms. Thomas and associates12 found AC histology to be an important prognostic factor related to survival of patients with carcinoid tumours. Many other authors agree with this observation.18 ,19 However, the authors did not describe specific prognostic factors for AC. Although tumour size and recurrences are related to life expectancy, in our experience, nodal disease remains an important prognostic factor to predict survival and recurrence.
Nodal disease is a frequent feature in AC. In fact, its relationship with prognosis has been reported in these patients.20 The investigation for lymph node metastases seems to be an unavoidable requisite to establish prognosis and to evaluate therapeutic strategies.11 Invasive mediastinal staging with mediastinoscopy inspection has been recommended for cN1 and cN2 tumours.14 Our data support this statement, because of the poorer prognosis of patients with nodal involvement as well as the higher frequencies of recurrences in this group. This supports the requirement of an appropriate and reliable mediastinal staging (endobronchial or transesophageal endoscopic ultrasound-guided needle aspiration biopsy, mediastinoscopy or thoracoscopy) before surgical treatment.
In the same line as our work, nodal involvement and complete resection were recognised as prognostic predictors in AC during the 2007 International Workshop on Advances in Pulmonary Neuroendocrine Tumours.21 Intermediate survival for patients with AC was reported, with distal site recurrence being more common than local recurrence. In our experience, nodal affection and recurrence are closely related. Davini and colleagues13 stated that ACs are more likely to recur regardless of stage, but their data did not support this affirmation. By contrast, Rea and colleagues11 observed that 50% of recurrences observed in AC were N+. Other authors have noted the relevance of lymph node micrometastasis detected by immunohistochemical techniques,22 worsening the prognosis of these patients for survival and recurrence. This would support radical lymphadenectomy in these cases. The analysis of our data allows us to demonstrate that a higher N-status influences the probability of tumour recurrence, confirming the need to determine lymph node involvement systematically in these patients.
Surgery represents the cornerstone of treatment of AC tumours. Complete standard surgical resection and mediastinal lymph node dissection is the treatment of choice. Atypical resections have been related to an increased number of recurrences in AC.23 In our series, 24% of patients who underwent SR presented locoregional recurrence at some time during follow-up. Furthermore, patients who underwent these SRs presented a higher incidence of locoregional recurrence when compared with LR, independently of N-status. This observation could suggest that the magnitude of resection is a predictive variable for locoregional recurrence, not only lymph node invasion. Emphasising this issue, Yendamuri and colleagues24 have attempted to ascertain whether SRs are sufficient for carcinoid tumours. They have recommended avoiding lobectomies in typical carcinoid tumours, although they find the atypical histology to be an adverse prognostic factor. Nevertheless, they make no indication about AC. In the same direction, Fox and colleagues25 have recently published the experience of the Surveillance Epidemiology and End Results (SEER) database about this aspect. Even when they do not find any disease-specific mortality in patients undergoing SR because of AC, the authors make no recommendation regarding these tumours. Moreover, they could not perform any recurrence analysis because of the lack of information in coding the data from SEER database. Our series, one of the largest published to date, specifically focused on AC, shows that SR should be reserved for patients at high cardiopulmonary risk, based on locoregional recurrence rates. As to surgical indication in cases of M1 preoperatively treated patients, we did not find any recommendations in the literature. In our experience, these patients present lower life expectancy and a higher recurrence rate than those staged as M0.
Focusing on adjuvant treatment of these tumours, there is no consensus about which patients could benefit from multimodal therapy. Some authors have tried to identify potential candidates for adjuvant ChT. Survival of N+ AC patients is poorer than survival in N0 patients. That is the reason why these patients could be candidates for adjuvant therapy. However, there is insufficient evidence to assess the efficacy of this treatment and the agent of choice.21 Data about this are scarce and inconsistent in our series, so we cannot draw a conclusion on the results obtained in this aspect.
In conclusion, nodal status, extent of resection and recurrence will affect prognostic evolution of these patients. Bearing in mind these data, standard surgical resection with radical lymphadenectomy is essential. In our experience, limited resections should be avoided except for special patient conditions, because of higher recurrence. Further studies with larger sample sizes and new prognostic marker analyses are recommended.
References
Footnotes
-
Collaborators Addendum: Emetne members: Mariano García-Yuste, MD PhD, Jose-Maria Matilla, MD PhD, Felix Heras, MD PhD, and Henar Borrego, MD (University Hospital, Valladolid); Ignacio Escobar, MD and Joan Moya, MD, PhD (Bellvitge Hospital, Barcelona); Juan Lago, MD, David Saldaña, MD PhD and Pilar Garrido, MD (Ramon-y-Cajal Hospital, Madrid); Francisco Cerezo, MD and Javier Algar, MD (Reina-Sofia Hospital, Cordoba); Federico Gonzalez-Aragoneses, MD, Carlos Simon, MD, Emilio Alvarez, MD and Maria Cebollero, MD (Gregorio-Marañon Hospital, Madrid); Jose-Manuel Rodriguez-Paniagua, MD (University Hospital, Alicante); Ricardo Guijarro, MD, PhD and Antonio Arnau, MD, PhD (General-University Hospital, Valencia); Luis Lopez-Rivero, MD, PhD, Santiago Quevedo, MD and Maria-Carmen Camacho, MD (Insular Hospital, Las-Palmas); Julio Astudillo, MD and Javier Perez, MD (Germans-Trias-Pujol Hospital, Badalona); Laureano Molins, MD (Clinic Hospital, Barcelona); Jose-Manuel Mier (Sagrado-Corazón Hospital, Barcelona); Antonio Cueto, MD, Abel Sanchez-Palencia, MD and Angel Concha, MD (Virgen-de-las-Nieves Hospital, Granada); Jorge Freixinet, MD, PhD, Pedro Rodriguez, MD and Teresa Romero, MD (Dr-Negrin Hospital, Las Palmas); Juan Torres, MD, PhD and Juan Bermejo, MD (Virgen-Arrixaca Hospital, Murcia); Nicolas Moreno, MD, PhD and Ana Blanco, MD (Virgen-Rocio Hospital, Sevilla); Jose-Maria Borro, MD and Mercedes de-la-Torre, MD and Ana Capdevilla, MD (University Hospital, Coruña); Ramon Moreno, MD (La-Princesa Hospital, Madrid); Mireia Serra and Ramon Rami-Porta, MD (Mutua-Terrassa Hospital, Terrassa); Ricardo Arrabal, MD, and Antonio Benitez, MD (Carlos-Haya Hospital, Malaga); Andres Varela, MD and Mar Cordoba, MD (Puerta-Hierro-Majadahonda Hospital, Madrid); Miguel-Angel Cañizares MD, PhD, Eva Garcia-Fontan, MD, Montserrat Blanco-Ramos, MD, PhD and Ana Gonzalez-Piñeiro, MD (University Hospital, Vigo); Ignacio Muguruza, MD, PhD and José Zapatero, MD, PhD, (Fundación-Jiménez-Díaz Hospital, Madrid); Juan-Jose Rivas and MD, Patricia Menal, MD (Miguel-Servet Hospital, Zaragoza); Genaro Galan, MD, PhD (Clinic Hospital, Valencia); and Emilio Ansotegui, MD (La-Fe Hospital, Valencia).
-
Contributors MAC was the main writer of the text. JMM, MG-Y and EG-F worked as internal revisers. MAC and AC coworked in the initial design of the project. AG-P assessed about pathological aspects of the paper. JA, NM-M, IM studied the state of art in published data about atypical carcinoid, introducing discussion topics. RG, RA and RA verified reliability of data. MAC and JMM performed statistical analysis, with the support of Statistics Department of Valladolid University. All of them participated in obtaining data for the database and all of them revised the final manuscript. EMETNE-SEPAR is the acronym of the Spanish Multicenter Study of Neuroendocrine Tumours of the Lung. All the authors take responsibility for the content of this work.
-
Competing interests None.
-
Ethics approval Ethics Committee from every participant hospital.
-
Provenance and peer review Not commissioned; externally peer reviewed.