Article Text

Abstract
Background Asthma and airway hyper-responsiveness are reportedly more common in children with sickle cell disease (SCD).
Aim To determine airway responsiveness, airway inflammation and clinical features of asthma in SCD.
Methods A prospective, single-centre study of 50 SCD children without overt pulmonary vascular disease and 50 controls. Exhaled nitric oxide (FeNO) and total serum IgE were measured and spirometry and methacholine challenge were performed. The methacholine dose–response slope (DRS) was calculated.
Results Doctor diagnosis of asthma was made in 7 (14%) SCD versus 12 (24%) control subjects (p=0.203). FeNO levels were similar in SCD and controls (p=0.250), and were higher in those with atopy and an asthma diagnosis (OR 4.33, 95% CI 1.7 to 11.1; p<0.05). zFEV1 (p=0.002) and zFEV1/FVC (p=0.003) but not zFVC (p=0.098) were lower in SCD versus controls. DRS was higher in those with asthma (p=0.006) but not in SCD versus controls (p=0.403). DRS correlated with FeNO and blood eosinophil count in controls but not SCD. In SCD, DRS was higher in those admitted to hospital with respiratory symptoms (n=27) versus those never admitted (n=23) (p=0.046). DRS was similar in those with at least one acute chest syndrome episode (n=12) versus those with none (n=35) (p=0.247).
Conclusions SCD children have airflow obstruction despite having minimal evidence of pulmonary vascular disease. Airflow obstruction is not associated with increased methacholine sensitivity or eosinophilic inflammation, at least as judged by FeNO. Airflow obstruction in SCD does not appear to be related to childhood eosinophilic asthma, but its pathophysiology remains ill understood.
- Paediatric lung disease
- sickle cell disease
- airway hyper-responsiveness
- airway obstruction
Statistics from Altmetric.com
Key messages
What is the key question?
-
Is there an increased prevalence of asthma and airway hyper-responsiveness in children with sickle cell disease?
What is the bottom line?
-
Children with sickle cell disease and only minimal evidence of pulmonary vascular disease had airflow obstruction, but no increase in airway responsiveness or exhaled nitric oxide.
Why read on?
-
Airflow obstruction is an early feature of sickle cell disease, but this does not appear to be related to childhood eosinophilic asthma and should not be treated as such.
Introduction
The haemoglobinopathy sickle cell disease (SCD) is characterised by haemolytic anaemia and recurrent vascular occlusive episodes predisposing to chronic tissue ischaemia and infarction. Defective haemoglobin (HbS) synthesis results in the polymerisation of HbS and sickle-shaped erythrocytes under hypoxic conditions. Patients with SCD are either homozygous for HbS (HbSS) or compound heterozygotes (HbSC), the latter probably having a lower incidence of vasculopathy.1
Respiratory morbidity, including asthma2 ,3 and acute chest syndrome (ACS),4–6 is common in children with SCD. Elevated total IgE in SCD is associated with increased wheeze and cough and is an independent risk factor for ACS.7 Diagnosing asthma in SCD is difficult. Airway hyper-responsiveness (AHR) measured using cold air or exercise has been reported in 20–64% in children with SCD3 ,8 ,9 but is not associated with symptoms of reactive airway disease8 or ACS.9 AHR to methacholine is no more frequent in SCD children reporting asthma symptoms than unselected SCD children,10 ,11 suggesting that AHR may be a component of SCD8 while asthma may represent a distinct coexisting condition.2 Ethnicity may be an important factor though, since AHR has been reported in 42% of young, healthy, African-American children, despite a doctor diagnosis of asthma in only 10%.12 Exhaled nitric oxide (FeNO) levels in children with asthma are used as an indicator of eosinophilic airway inflammation, but studies in SCD children are few. FeNO has been reported as higher,13 similar14 or lower15 in SCD patients compared with healthy controls.
Both obstructive and restrictive lung function have been described in SCD. Lower airway obstruction is reported in 13–35% of unselected SCD children aged 3 months or above16–18 and is associated with an increased incidence of pain and chest crises.16 Others report a lower prevalence of lower airway obstruction and suggest that age may be an important factor, with restrictive lung function developing in older children and young adults due to previous episodes of ACS and chronic lung injury.19
We have previously compared the pulmonary vascular abnormalities in 50 SCD children with controls of a similar age, gender and ethnicity showing that SCD children had pulmonary hypertension related to increased pulmonary blood flow,20 but only subtle abnormalities of pulmonary vasculature manifest on exercise by a failure to increase carbon monoxide transfer (DLCO, a surrogate for pulmonary capillary blood volume).21 We prospectively compared airway function in these two groups, hypothesising that SCD children with minimal pulmonary vascular changes may still have airflow obstruction.
Methods
Patient selection and recruitment
Fifty (26 female) patients aged 10–18 years with known haemoglobin SS or SC disease were recruited from the paediatric haematology clinic at St George's Hospital, London, UK. Full details have been reported before.20 ,21 Inclusion criteria were age >10 years, height >125 cm, genotype SS or SC and at least one Afro-Caribbean parent. Children had to be >125 cm to perform bicycle exercise testing. Exclusion criteria were HIV infection or a history of cerebrovascular accident or congenital heart disease. Fifty-six consecutive patients were originally invited to participate in the study; five declined and one was excluded (HIV-positive). All participants had to be well and free of any vaso-occlusive crises (VOC) for ≥14 days before investigations. Fifty (25 female) unselected, controls of similar age, sex and ethnicity were recruited from 59 patients’ friends and siblings; nine declined and none were excluded. History, including pulmonary symptoms, and examination, including Tanner22 pubertal staging, was performed in all participants. In SCD patients, the number of hospital admissions with painful VOC in the previous 2 years and the total number of admissions with ACS were recorded. A history of doctor-diagnosed asthma was determined by asking the questions: (1) Have you ever been told by your GP that you have asthma? (2) Do you or have you used any inhaled medications for treatment of asthma? A history of atopy was sought by asking subjects and their parents whether their doctor had diagnosed eczema, hay fever or allergic rhinitis at any time. Specific features of asthma and atopy were also sought as part of the examination. Blood was taken for measurement of total IgE, haemoglobin (Hb), reticulocyte count, per cent fetal Hb and Hb electrophoresis. Standing height±1 mm was measured (Harpenden stadiometer, Holtain Ltd. Crymmych, UK) along with weight±0.1 kg using electronic scales (Seca, Birmingham, UK). Ethics approval was granted by Wandsworth Local Ethics Committee ref no 04/Q0803. Informed written consent was obtained for each subject.
Exhaled nitric oxide
Single-breath online FeNO measurement, in accordance with European Respiratory Society/American Thoracic Society (ERS/ATS) guidelines, was always performed before spirometry as forced expiration may decrease FeNO.23 Details are available in the online supplement.
Spirometry
Spirometry was performed according to ATS/ERS guidelines.24 The Global Lungs Initiative (GLI) reference data were used and subjects converted to z scores using the GLI reference equations.25 Details are available in the online supplement.
Methacholine challenge testing
Methacholine challenge was performed according to ATS/ERS guidelines.26 Instead of a baseline FEV1 <60% predicted or <1.5 L as exclusion criteria, FEV1 <65% was used to minimise hypoxic risk. Other exclusions were current wheeze or dyspnoea or a baseline SaO2 of <92%. Heart rate and SaO2 were monitored continuously using a finger probe pulse-oximeter (Nellcor, USA). The methacholine dose–response slope (DRS) for each subject was expressed as per cent decline in FEV1/dose, where the numerator was the per cent decline in FEV1 from the postsaline value to the value after the final administered dose of methacholine and the denominator was the final cumulative methacholine dose administered.27
Statistical analysis
There are no data to inform a power calculation, and sample size was opportunistic. Continuous data are presented as median and 95% CI. Groups were compared using a Mann–Whitney test or Fisher's exact test as appropriate. Categorical variables are presented as N (%), and differences were compared using χ2 analysis. Spearman rank correlation was used to examine the significance of the association of DRS with continuous variables. All analyses were performed using Stata V.12.1 (StataCorp LP, Texas, USA), and a p value of <0.05 was taken as being statistically significant.
Results
Patient characteristics and demographics
Patients (n=50) and controls (n=50) were of similar age, race and gender. Patients of either sex were significantly shorter than controls (males, p=0.002; females, p=0.021) (table 1). SCD genotype was HbSS (n=34) and HbSC (n=16). Four patients were on a blood transfusion programme and two were taking hydroxyurea; of these six, one was receiving both treatments. None of the five female controls admitting to smoking cigarettes had a history of respiratory illness or asthma. None of the patients or male controls admitted to smoking.
Demographics and relevant clinical data
Doctor-diagnosed asthma was not more common in SCD, occurring in 7/50 (14%) SCD subjects and 12/50 (24%) controls (p=0.203). Two controls were prescribed inhaled budesonide in doses of 200 and 400 μg/day and two SCD subjects 400 μg/day each. Of 27 SCD patients with previous hospital admissions for chest symptoms, 12/27 had at least one confirmed episode of ACS. Confirmed ACS occurred in 4 of 7 with doctor diagnosed asthma compared with 8/43 SCD patients without asthma, (p=0.024).
There was no difference in total serum IgE between SCD and controls or in the prevalence of atopy, defined as total serum IgE >75 ku/L. IgE was >75 ku/L in 28/48 (56%) SCD children versus 33/50 (64%) controls (p=0.453; table 1).
Exhaled nitric oxide
FeNO levels in HbSS and HbSC subjects and controls were similar; HbSS 10.1 (6.9 to 13.4), HbSC 8.7 (1.9 to 15.6), controls 13.1 (10.5 to 15.8) ppb; p=0.250 (figure 1). Twenty-two subjects (9 SCD, 13 controls) had FeNO >20 ppb; p=0.334. In SCD and controls combined, FeNO levels were higher in those with atopy and doctor-diagnosed asthma (OR 4.33 (1.7 to 11.1); p<0.05).

FeNO measurements were similar in HbSS (10.1 (6.9 to 13.4)), HbSC (8.7 (1.9 to 15.6)) and control (13.1 ppb (10.5 to 15.8)) subjects (n=100); p=0.25.
Spirometry
FVC z scores were similar in SCD subjects and controls (p=0.098; table 2, figure 2A), but FEV1 z scores were lower in SCD subjects compared with controls (p=0.002; table 2, figure 2B), resulting in zFEV1/FVC also being lower in SCD subjects compared with controls (p=0.003; figure 2C, table 2). Within the SCD group, zFEV1 and zFVC were lower in HbSS compared with HbSC (p=0.018 and 0.004, respectively), resulting in no difference in zFEV1/FVC between HbSS and HbSC (p=0.308, table 3). zFEV1/FVC in SCD subjects with prior admission to hospital for chest symptoms (−0.88 (−1.27 to −0.51), n=27) was similar in SCD subjects with no such prior admissions (−1.07 (−1.31 to −0.47), n=23; p=0.99) and similar in SCD subjects who had experienced ACS (−0.81 (−1.41 to −0.22), n=12) compared with those who never had (−0.92 (−1.24 to −0.60), n=38; p=0.75). Analysis of these variables excluding SCD subjects on transfusion programmes or hydroxyurea treatment (n=5) did not change the significance of the results, nor did further analysis excluding smoking controls (n=5) (data not shown).
Spirometry in SCD patients and controls
Spirometry in SCD subgroups
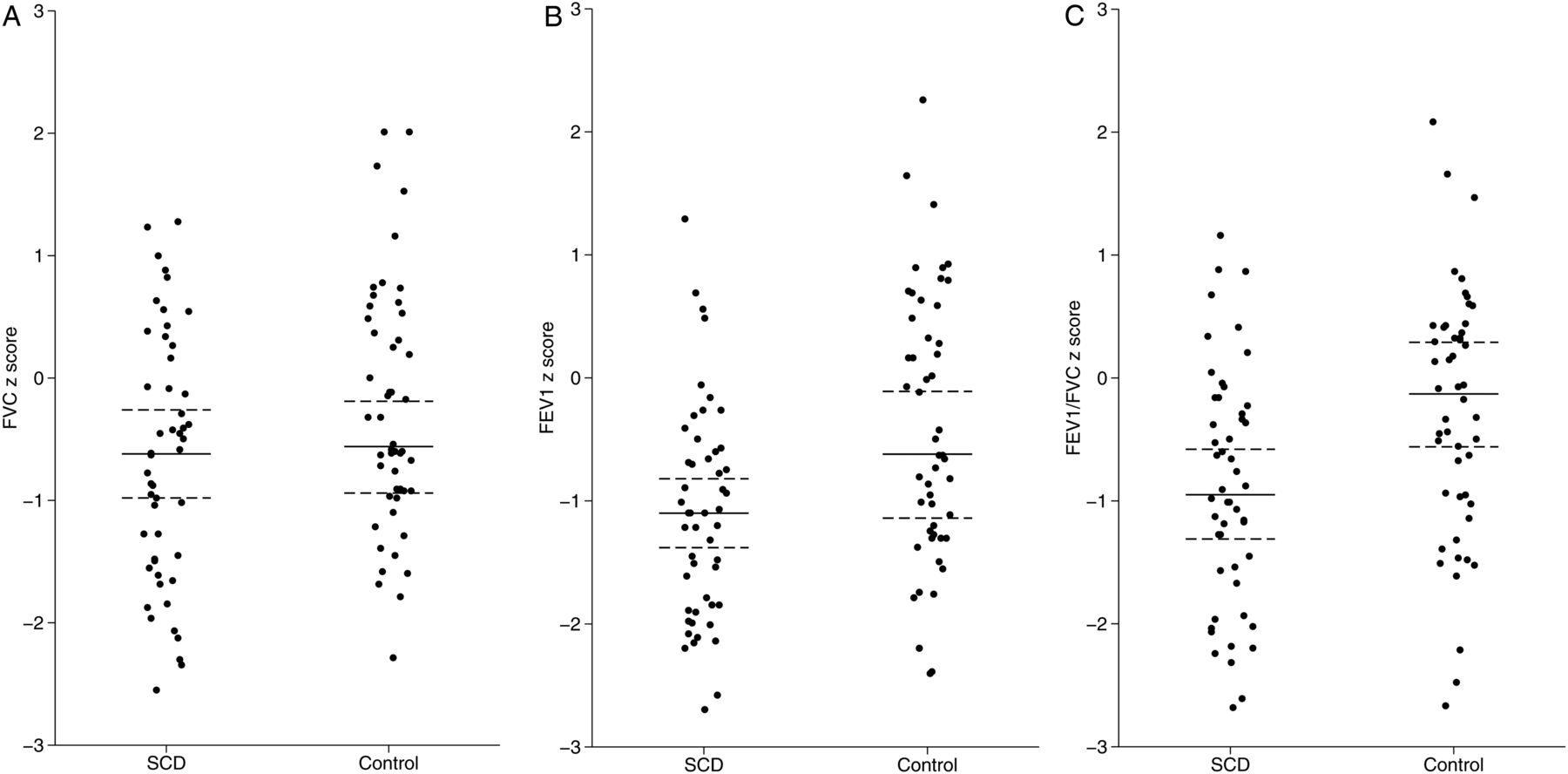
(A) zFVC (median, 95% CI) in sickle cell disease (SCD) and control subjects (n=100); p=0.098. (B) zFEV1 (median, 95% CI) in SCD and control subjects (n=100); p=0.002. (C) zFEV1/FVC (median, 95% CI) in SCD and control subjects (n=100); p=0.003.
Methacholine challenge and sensitivity
Ninety-three subjects completed methacholine challenge testing (MCT). Of the seven who did not, five failed to attend or refused to complete the test, FEV1 was too low (n=1) and SaO2 was too low (n=1).
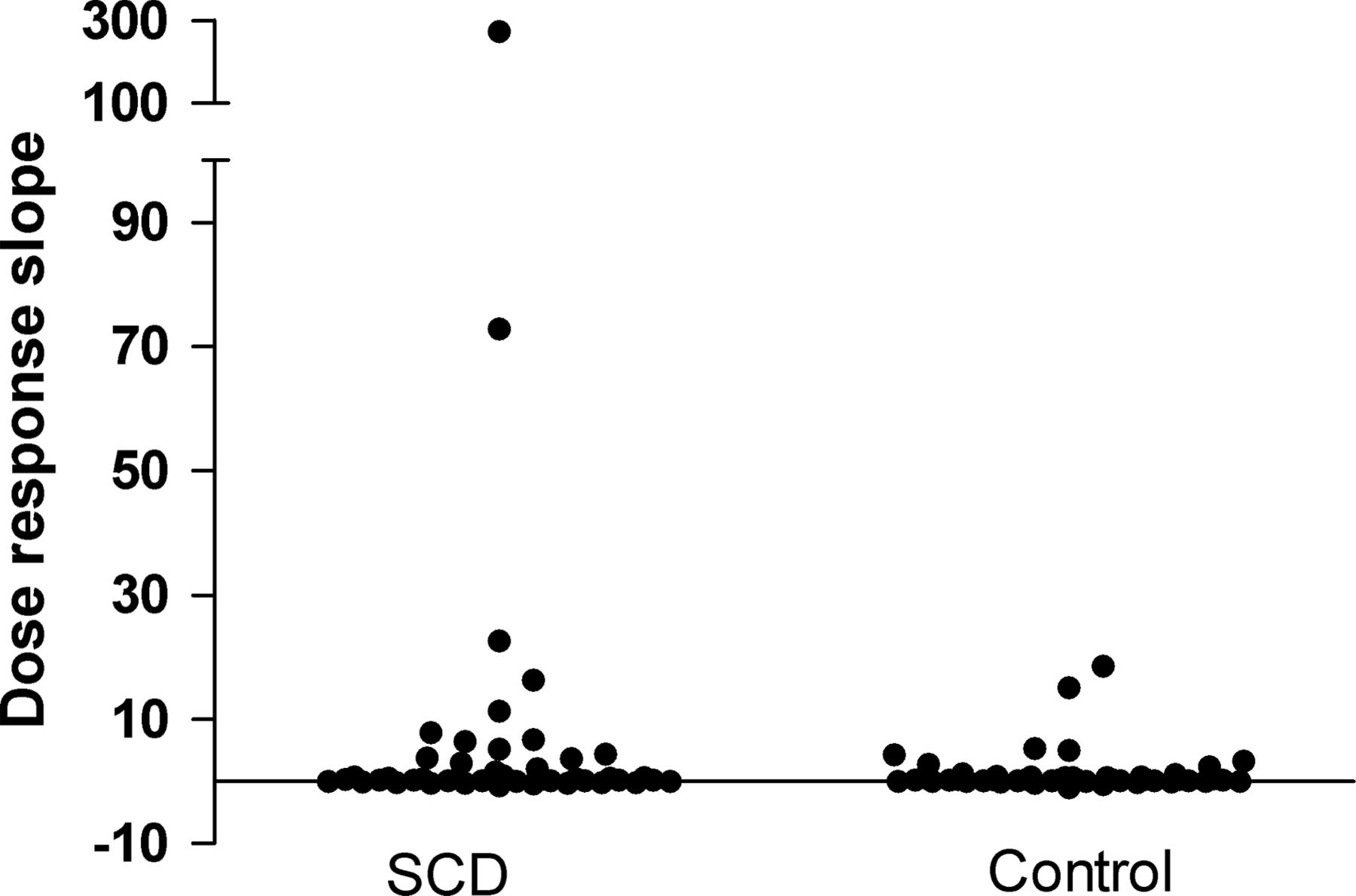
Median (95% CI) calculated DRS was similar in SCD and control children: 0.36 (0.17 to 0.62) vs 0.30 (0.20 to 0.74) (p=0.403; figure 3). In all subjects, an asthma diagnosis was associated with a significantly higher DRS: 4.46 (0.27 to 6.76) vs 0.30 (0.18 to 0.36) for those without asthma (p=0.006). DRS correlated with zFEV1/FVC, FeNO and blood eosinophil count in control but not SCD children (table 4). There was no correlation in either group between DRS and total IgE, age, Hb and reticulocyte count (table 4). Multiple linear regression analysis in SCD subjects with DRS as the dependent variable using age, sex, SS or SC, zFEV1, zFVC, zFEV1/FVC, IgE, FeNO, VOC, ACS as independent factors showed that no factor was significant, neither together (p=0.327) nor in a stepwise fashion. The same analysis in controls showed that FeNO was highly significant (p<0.001) explaining 28% of the variance in DRS, but no other factors were significant. Eosinophil count was not included in the regression analysis since this result was available for only 57/93 (61%) of subjects.
Associations with methacholine sensitivity expressed as DRS in SCD and control subjects
{kind=link}
{kind=link}
{kind=link}
Dose–response slope results for all subjects (n=93; p=0.403).
There was no difference in DRS between HbSS and HbSC subjects: 0.43 (0.05 to 3.01) vs 0.28 (0.16 to 3.73) (p=0.816). DRS was significantly greater in those requiring admission to hospital with respiratory symptoms (n=27) compared with those never admitted (n=23): 0.44 (0.23 to 7.85) vs 0.22 (0.16 to 0.65) (p=0.046), while there was no difference in DRS between those who had experienced at least one episode of ACS (n=12) compared with those who had not (n=35): 0.42 (0.05 to 22.64) vs 0.34 (0.18 to 0.74) (p=0.247). Reanalysis of these data excluding SCD subjects on transfusion programmes or hydroxyurea treatment (n=5) and then excluding smoking controls (n=5) made no difference to the significance of the results (data not shown).
No subject experienced significant hypoxia (SaO2 <91%) during MCT. Nineteen SCD patients received salbutamol following methacholine challenge, as did 18 controls. Symptoms were reported by a total of nine children (four chest tightness with wheeze, three cough only, two dyspnoea). The degree of bronchodilator reversibility was similar in SCD and controls: 33 (22 to 39) vs 33 (17 to 40) % (p=0.796). No child with SCD experienced a chest crisis subsequent to MCT.
Discussion
For the first time, we show that child and adolescent patients with SCD and minimal evidence of pulmonary vascular disease have reduced forced expiratory flow but no increased methacholine responsiveness or elevated FeNO compared with controls of similar age, gender and ethnicity, as might have been expected if their airway obstruction was due to asthma. The reported asthma prevalence in our controls was 24%, similar to prevalence rates of 23% and 33% reported in black African and black Caribbean UK adolescents, respectively,28 and similar to the reported asthma prevalence of 14% in the SCD subjects in our study. Reported asthma prevalence may be considerably lower than AHR prevalence. Despite only 10% of non-sickle, middle-class, suburban-dwelling African-American children having an asthma diagnosis in one study, AHR prevalence was 42% and DRS did not correlate with total serum IgE.12 Other authors have reported a high prevalence of AHR in SCD children, varying from 55%29 to 78%,10 ,11 but these studies lacked control groups for comparison. We chose to report methacholine responsiveness expressed as DRS rather than an arbitrary definition of AHR using cut-off values in order to enable the precise calculation of airway responsiveness for all subjects.27 We found that methacholine responsiveness was the same in control and SCD subjects, but was significantly increased in SCD subjects admitted to hospital for respiratory symptoms. It was not increased however in SCD subjects with at least one confirmed ACS episode, but our numbers are small. Others have reported a lack of association of AHR with ACS.9 In a different study,29 methacholine responsiveness correlated with IgE, a younger age and lactate dehydrogenase (LDH), a marker of haemolysis. We found no such correlation with age and IgE, but we did not measure LDH. Instead, we measured reticulocyte count as an indicator of haemolysis since the usefulness of LDH as a marker of haemolysis was not established at the time of this study, but we found no correlation with methacholine responsiveness. Rather, we found correlation with markers of eosinophilic inflammation in control but not in SCD children. Additionally we found total serum IgE levels and atopy prevalence were similar in SCD and controls, but children with a reported doctor diagnosis of asthma and atopy had significantly higher FeNO, irrespective of whether or not they had SCD.
SCD subjects had significantly worse obstructive airway disease compared with controls despite similar degrees of methacholine responsiveness and asthma and atopy prevalences. Moreover, HbSS children had significantly reduced zFEV1 and zFVC compared with HbSC children despite no difference in methacholine responsiveness. Although hospital admission for respiratory symptoms was associated with increased methacholine responsiveness, it was not associated with poorer spirometry in these subjects. Similarly, spirometry was not worse in SCD subjects who had experienced ACS compared with those who had not. Methacholine responsiveness therefore may not be an important aetiological factor in the evolution of airway obstruction in SCD patients. Lower airway obstruction in SCD children becomes more prevalent with age.30 It does not seem to be associated with an asthma diagnosis but is associated with the number of chest and painful crises,16 although we did not observe this. We could not identify any clinical parameter that was associated with lower airway obstruction in SCD. We hypothesise that sickling within the bronchial circulation may lead to airway ischaemia and mucosal injury with the subsequent development of fibrosis and progressive airway obstruction. This would imply that at least some of the obstruction may be fixed. Although bronchodilator reversibility has been reported in HbSS children with lower airway obstruction, not all obstruction was reversible.17 In support of our hypothesis is the finding of generalised pulmonary inflammation, airway mucosal injury and subsequent fibrosis in patients undergoing cardiopulmonary bypass, unifocalisation procedures and lung transplantation in whom the bronchial circulation is either severely compromised or interrupted.31–33
Our study is strengthened by the inclusion of an ethnically matched control group. However, this control group is relatively small, and much larger population-based studies are needed to confirm our findings of a similar degree of airway responsiveness in healthy, black Afro-Caribbean and SCD children. The relatively low zFEV1 and zFVC values observed in controls may be explained by the use of GLI data that do not include ethnically adjusted prediction equations but do include reference data from this racial group. Ideally, we would have performed plethysmography to measure lung volumes, particularly functional residual capacity for evidence of air trapping and airways resistance that may have shown evidence of small airway obstruction in children with a normal FEV1. It is possible therefore that we underestimated the prevalence and degree of lower airway obstruction. The current study was part of a larger study of cardiopulmonary function in children with SCD, and in order to minimise the demands on children's time, spirometry only was performed.
Other weaknesses in our study include the relatively small numbers possibly obscuring a small increase in the prevalence of true asthma in SCD. However, we were able to show the expected elevated FeNO in atopic children, a useful positive control. We also relied on an indirect measurement of eosinophilic airway inflammation, namely FeNO, and more direct methods such as sputum induction would have been preferable. However, virtually all our patients were steroid naïve, the group in which the best agreement between FeNO and airway eosinophilia has been reported.34 Our methods would have missed any neutrophilic inflammation present, but this does not affect our conclusion that asthma medications should be used cautiously in these patients because neutrophilic inflammation is generally not steroid sensitive. We have shown that MCT can be performed safely in children with SCD, but our relatively small numbers may have underestimated the risks. A previous study of methacholine responsiveness in 99 SCD children was complicated by a painful episode requiring hospital admission in one child.29 We may have overestimated the prevalence of atopy in control and SCD children by using an arbitrary cut-off value for total serum IgE. Total IgE increases with age and there are ethnic differences, such that total IgE is approximately 1.3 times higher in Afro-Caribbean compared with white British children.35 These reference data however were derived from a study of 58 Afro-Caribbean children, and larger population-based studies are needed.
In summary, children with SCD and minimal changes of pulmonary vascular disease had evidence of airflow obstruction but without the signature features of childhood asthma, namely atopy, increased airway responsiveness to methacholine and elevated FeNO. MCT revealed that increased methacholine responsiveness in SCD children and controls was associated with a doctor diagnosis of asthma. A diagnosis of asthma and atopy was equally common in SCD and controls and was associated with higher FeNO. Our findings suggest that the similar degrees of methacholine responsiveness in SCD and controls may be related to Afro-Caribbean ethnicity rather than SCD, but this finding needs confirmation in a larger study. The implications of this study are that airway obstruction is an early feature of HbSS and HbSC SCD and is not related to asthma-like pathology. Careful consideration should be given before prescribing conventional asthma treatment in these children.
Acknowledgments
L Perry and J Jaye (respiratory technicians at Royal Brompton Hospital) assisted with 10% of all airway studies. M Roughton, medical statistician, assisted with statistical analyses.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors RAC recruited all subjects, supervised 90% of all tests and wrote the first draft of the paper. MR and AB assisted with writing and project supervision. RAC, MR and SC analysed the data. SC designed the whole study, completed writing and supervised the project. All authors agreed on the final version of the manuscript.
-
Funding Sobell Institute and St George's Hospital Charitable trust.
-
Competing interests None.
-
Ethics approval Wandsworth Local Ethics Committee ref no 04/Q0803.
-
Provenance and peer review Not commissioned; externally peer reviewed.