Article Text

Abstract
Background In patients with acute pulmonary embolism (PE), rapid and accurate risk assessment is paramount in selecting the appropriate treatment strategy. The prognostic value of right ventricular dysfunction (RVD) assessed by multidetector CT (MDCT) in normotensive patients with PE has lacked adequate validation.
Methods The study defined MDCT-assessed RVD as a ratio of the RV to the left ventricle short axis diameter greater than 0.9. Outcomes assessed through 30 days after the diagnosis of PE included all-cause mortality and ‘complicated course’, which consisted of death from any cause, haemodynamic collapse or recurrent PE.
Results MDCT detected RVD in 533 (63%) of the 848 enrolled patients. Those with RVD on MDCT more frequently had echocardiographic RVD (31%) than those without RVD on MDCT (9.2%) (p<0.001). Patients with RVD on MDCT had significantly higher brain natriuretic peptide (269±447 vs 180±457 pg/ml, p<0.001) and troponin (0.10±0.43 vs 0.03±0.24 ng/ml, p=0.001) levels in comparison with those without RVD on MDCT. During follow-up, death occurred in 25 patients with and in 13 patients without RVD on MDCT (4.7% vs 4.3%; p=0.93). Those with and those without RVD on MDCT had a similar frequency of complicated course (3.9% vs 2.3%; p=0.30).
Conclusions The PROgnosTic valuE of CT study showed a relationship between RVD assessed by MDCT and other markers of cardiac dysfunction around the time of PE diagnosis, but did not demonstrate an association between MDCT–RVD and prognosis.
- Pulmonary Embolism
Statistics from Altmetric.com
Key messages
What is the key question?
-
What is the prognostic value of right ventricular dysfunction (RVD) assessed by multidetector CT (MDCT) in normotensive patients with pulmonary embolism (PE)?
What is the bottom line?
-
This study does not support the hypothesis that an enlarged RV on MDCT leads to a higher 30-day all-cause mortality or higher rate of life-threatening adverse events.
Why read on?
-
The presence or absence of RVD on MDCT should not drive decision-making regarding outpatient management or thrombolytic therapy for the treatment of acute PE.
Introduction
Early mortality rates for pulmonary embolism (PE) range from less than 5% in clinically stable patients to 58% in patients who have cardiogenic shock.1–4 Based on risk profiles, some patients with PE may safely undergo treatment at home and avoid admission to a hospital,5 while others may require hospitalisation and immediate recanalisation of the occluded pulmonary arteries. Risk stratification tools may help with decision-making regarding appropriate management of patients with acute PE.6
In patients with PE, studies have validated several risk stratification algorithms that use different combinations of clinical and laboratory variables.7 In the most severely affected patients, circulatory failure typically develops progressively within the first hours after onset of PE. Increased pulmonary vascular input impedance overwhelms the adaptive resources of the right ventricle and results in acute cor pulmonale. A number of echocardiographic parameters permit the non-invasive diagnosis of right ventricular dysfunction (RVD) at the bedside. Several registry studies and meta-analyses demonstrated an association between transthoracic echocardiography (TTE) parameters in patients with acute PE and poor inhospital outcomes.8–10 However, reliable and accurate echocardiography requires experienced personnel, and lack of TTE availability may also affect its clinical utility. Alternatively, medical centres typically have available and frequently use multidetector (ie, contrast-enhanced) CT (MDCT) for evaluating and diagnosing patients with suspected PE.11–13 Since MDCT allows the visualisation and measurement of the heart chambers, it has the potential to provide an alternative to echocardiography for the assessment of RV function in patients with acute PE.14–17
The PROgnosTic valuE of CT scan in haemodynamically stable patients with acute symptomatic PE (PROTECT) study was designed to prospectively assess the prognostic significance of MDCT findings and other prognostic factors in haemodynamically stable patients with acute symptomatic PE.
Methods
Study design
PROTECT is a prospective, multicentre observational cohort study, designed by the authors, and sponsored by the Institute of Health Carlos III, Spain (NCT00880737).18 The institutional review board of each centre approved the protocol and consent forms.
Setting
Patients underwent recruitment from the Emergency Department of five academic and seven general urban hospitals in Spain between 1 January 2009 and 31 May 2011.
Study eligibility and patients
Study eligibility required confirmation of the diagnosis of PE with a positive contrast-enhanced, PE-protocol (MDCT),19 and excluded patients who had haemodynamic instability at presentation (defined as cardiogenic shock, systolic blood pressure <90 mm Hg or use of inotropic support), treatment with thrombolytics at the time of PE diagnosis, life expectancy less than 3 months, pregnancy, geographic inaccessibility that precluded follow-up and age younger than 18 years.18
Multidetector CT
Trained and certified local radiologists assessed MDCT–RVD by measuring the ratio of the right to left ventricular short axis diameters. The maximal distance between the ventricular endocardium and the interventricular septum, perpendicular to the long axis of the heart, determined each ventricular diameter.20 The radiologists performed the measurements approximately at the valvular plane for the two-dimensional axial transverse images, and they allowed for measurement at different levels to capture the maximum dimension of the right and left ventricles. PROTECT a priori defined MDCT-assessed RVD as a ratio of the RV to the left ventricle (LV) short axis diameters of greater than 0.9.18
Transthoracic echocardiography
The study required that patients undergo TTE within 24 h after diagnosis of PE. Trained and certified local cardiologists interpreted each echocardiogram. The study defined echocardiographic RVD as the presence of at least two of the following: dilatation of the RV (end-diastolic diameter >30 mm from the parasternal view or the RV appearing larger than the left ventricle from the subcostal or apical view), hypokinesis of the RV free wall (any view) and estimated systolic pulmonary artery pressure over 30 mm Hg.18 ,21 ,22
Cardiac biomarker determinations
The Hospital Universitario Ramon y Cajal-IRYCIS Biobank processed the biological samples. PROTECT used a core laboratory for blood biomarker measurement. The core laboratory personnel measured cardiac troponin I (cTnI) levels quantitatively by using a microparticle enzyme immunoassay (Abbot, USA). PROTECT defined cTnI concentrations of >0.05 ng/ml as the 99th percentile of a healthy reference population with a coefficient of variation (CV) of <10% and indicative of myocardial injury (cTnI positive).18 ,23 Core laboratory personnel measured brain natriuretic peptide (BNP) levels by microparticle enzyme immunoassay (MEIA) system immunoassay in an AxSYM analyser (Abbott, USA). PROTECT defined BNP concentrations of >100 pg ml−1 as indicative of cardiac myocyte stretch (BNP positive).18 ,24
Study end points and outcome measures
PROTECT used all-cause mortality as the primary end point. Secondary outcomes included: (1) symptomatic recurrent PE (confirmed by the presence of a new at least segmental intraluminal filling defect or an extension of a previous filling defect on CT);19 (2) major bleeding (clinically overt bleeding associated with any of the following: a fall of haemoglobin levels of 2 g/dl or more; transfusion of two or more units of red blood cells; haemodynamic compromise requiring emergency intervention; intracranial, retroperitoneal or critical site bleeding; or bleeding that contributes to death);25 and (3) ‘complicated course’, defined as death from any cause, haemodynamic collapse (defined as need for cardiopulmonary resuscitation, systolic blood pressure <90 mm Hg for at least 15 min, need for cathecolamine administration or need for thrombolysis) or adjudicated recurrent PE within 30 days of follow-up. The study assessed all-cause mortality, symptomatic recurrent PE, major bleeding and complicated course for the first 30 days after the diagnosis of PE. An independent Adjudication Committee, whose members were blinded to initial prognostic test results, adjudicated all serious adverse events.
Statistical analyses
The study reported categorical data as proportions and continuous data as mean±SD or median (first–third IQR). We used unpaired two-tailed t tests or the Mann–Whitney U test (for those variables found not to follow a normal distribution) for comparisons in the distributions of continuous variables between patients with or without MDCT–RVD, and χ2 or Fisher's exact tests compared categorical data between both groups. Sample size calculation was done for the primary end point. We a priori calculated a power of 95% (two-sided type 1 error, 5%) to reject the null hypothesis that the presence of RV enlargement on chest CT will not predict the primary end point in the available sample of 850 patients, using the following assumptions: presence of RV enlargement on chest CT in 40% of the sample, and a 30-day mortality rate of 10% in patients with and 5% without RV enlargement, based on observed mortality rates in patients with and without RV dysfunction from the International Cooperative Pulmonary Embolism Registry.1 We used receiver-operating characteristic curve analysis to assess the discriminative power of MDCT for RV dysfunction, and echocardiography served as the reference standard.
The study used logistic regression to assess for an independent association between potential baseline predictors and the outcome of complicated course in the cohort. For the manual backward stepwise multivariable logistic regression model, we assessed variables that had a significance level of p less than 0.05 in univariable analyses. The model primarily assessed the prognostic information of cardiac predictors (ie, MDCT, echocardiography, BNP and troponin testing) and adjusted for clinical confounders deemed statistically significant on univariable analyses (heart rate >110/min (vs other) and systolic blood pressure <100 mm Hg (vs other)).
To test the robustness of the model, we assessed the effect of excluding patients with prior cardiopulmonary disease. We also performed similar analyses that used a different ratio of the RV to the LV cut-off to define the groups with (>1) and without (≤1) RV dysfunction on MDCT. Statistical significance was defined as a two-tailed p value of <0.05 for all analyses. Analyses were performed using SPSS V.15.0 for the personal computer (PC) (SPSS, Inc. Chicago, Illinois, USA).
Results
Study sample
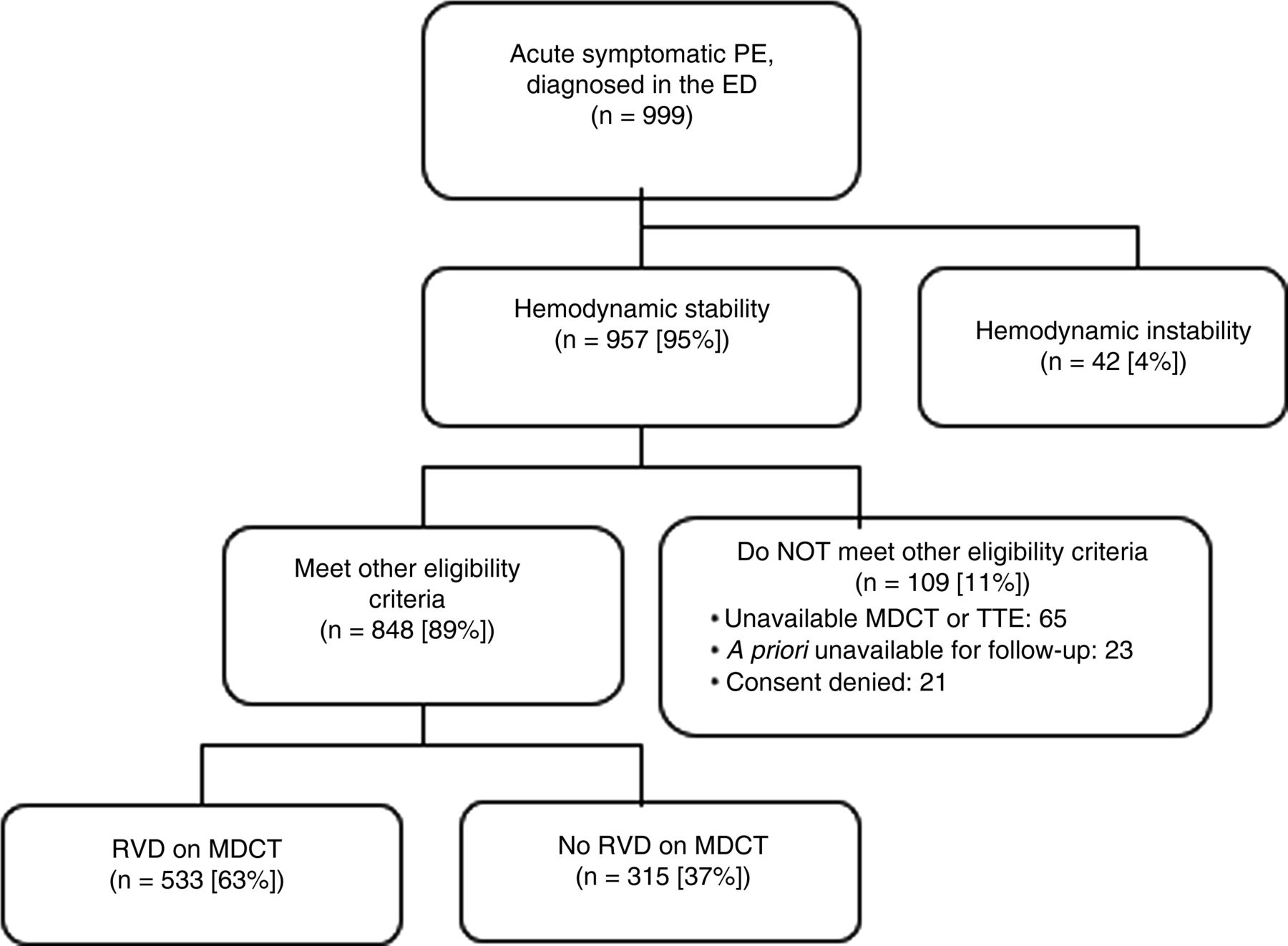
The study staff screened 999 consecutive patients with acute PE for eligibility. Haemodynamic instability excluded 42 (4.2%) patients from participation. Of the remaining 957 haemodynamically stable patients, the study excluded 6.8% (65 of 957 patients) because they did not have a technically adequate MDCT (n=28; 2.9%) or a transthoracic echocardiogram (n=37; 3.9%). Other reasons for exclusion included unavailability for follow-up (n=23) and refusal to give informed consent (n=21). The study enrolled the remaining eligible 848 patients (416 men and 432 women) (figure 1).
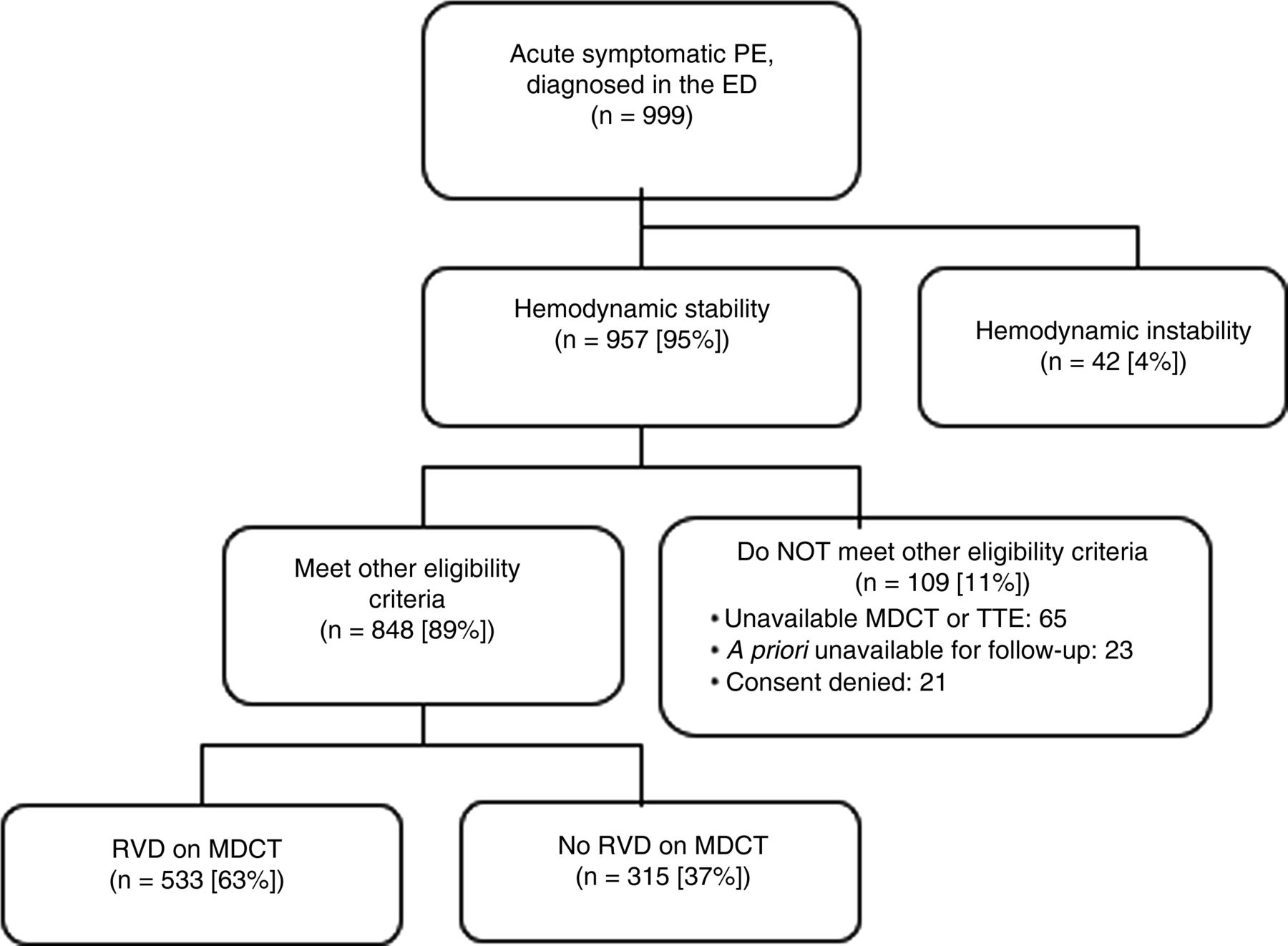
Patient flow diagram. PE, pulmonary embolism; ED, emergency department; MDCT, multidetector computed tomography; TTE, transthoracic echocardiography; RVD, right ventricle dysfunction.
Table 1 shows the patients’ clinical symptoms, predisposing conditions and relevant findings at presentation. Of these 848 haemodynamically stable patients with acute symptomatic PE, 192 (22.6%; 95% CI 19.8% to 25.5%) had echocardiographic RVD, 139 (16.4%; 95% CI 13.9% to 18.9%) had elevated cTnI levels and 380 (44.8%; 95% CI 41.5% to 48.2%) had elevated BNP levels. On MDCT evaluation, right to left ventricular diameter ratio ranged from 0.5 to 3.25 and had a median value of 1.0 (25th–75th percentile, 0.82–1.24). Overall, 533 patients (62.8%; 95% CI 59.6% to 66.1%) had RVD on MDCT. As shown in table 1, those patients with RVD on MDCT were older and had more signs of clinical severity (syncope, tachycardia and hypoxemia) compared with those without RVD on MDCT. Compared with those without RVD on MDCT, patients with RVD on MDCT had more frequent echocardiographic RVD (30.6% vs 9.2%, p<0.001) and higher BNP (269±447 vs 180±457 pg/ml, p<0.001) and cTnI levels (0.10±0.43 vs 0.03±0.24 ng/ml, p=0.001). When using echocardiography as the reference standard for RVD, MDCT-detected RVD had an area under the receiver-operating characteristic curve of 0.72 (95% CI 0.68 to 0.76).
Baseline characteristics and treatment information for haemodynamically stable patients with acute symptomatic pulmonary embolism
Outcomes
Regarding the primary outcome, 38 of the 848 (4.5%; 95% CI 3.1% to 5.9%) patients died during the 30-day follow-up period. Investigators adjudicated death as fatal PE in 11 of these patients (29.0% of the total deaths; 95% CI 14.5% to 43.4%), and this corresponded to a cumulative rate of fatal PE of 1.3% (95% CI 0.5% to 2.1%) at 30 days after PE diagnosis. Cancer (28.9%; 11 of 38 patients), other types of cardiopulmonary disease (23.7%; 9 of 38), bleeding (7.9%; 3 of 38 patients) and other miscellaneous diseases (10.5%; 4 of 38 patients) caused the other deaths. Three of 848 patients (0.3%; 95% CI 0% to 0.7%) had recurrent symptomatic PE (one non-fatal and two fatal), 19 patients (2.2%; 95% CI 1.2% to 3.2%) suffered a major bleeding episode and 63 patients (7.4%; 95% CI 5.7% to 9.2%) had a complicated course. In addition to the 38 deaths (including the two from recurrent PE), complicated course was due to haemodynamic collapse in 28 patients and non-fatal symptomatic recurrent PE in one patient (table 2).
Thirty-day clinical events after diagnosis and treatment for haemodynamically stable patients with acute symptomatic PE
MDCT and outcomes
Regarding 30-day all-cause mortality, 25 deaths (4.7%; 95% CI 2.9% to 6.5%) occurred in the group of 533 patients entering the study with RVD on MDCT, whereas 13 deaths (4.3%; 95% CI 2.0% to 6.6%) occurred in the group of 302 patients who did not have RVD on MDCT (absolute difference 0.4%; 95% CI of the absolute difference, −2.5%–3.3%; p=0.932). PE-related mortality within 30 days of PE diagnosis occurred somewhat more frequently in patients with RVD on MDCT (1.9% vs 0.3%; absolute difference 1.6%; 95% CI of the absolute difference, 0.3% to 2.9%; p=0.053). Haemodynamic collapse within 30 days of PE diagnosis occurred in 21 patients (3.9%; 95% CI 2.3% to 5.6%) entering the study with RVD on MDCT, and in seven patients (2.3%; 95% CI 0.6% to 4.0%) without RVD on MDCT (absolute difference 1.6%; 95% CI of the absolute difference, −0.8% to 4.0%; p=0.293) (table 2).
After excluding patients with prior cardiopulmonary disease, RVD on MDCT did not have a significant association with all-cause mortality (4.3% vs 4.0%; p=0.866), PE-related death (1.3% vs 0.4%; p=0.302) or a complicated course (8.3 vs 6.5%; p=0.398) at 30 days. We found similar results when we stratified analyses by a ratio of the RV to the LV>1.
Cardiac predictors of a complicated course at 30 days
Based on univariate logistic regression analyses, significant baseline predictors of a complicated course during follow-up included echocardiographic RVD (OR 2.62; 95% CI 1.54 to 4.45; p<0.001), elevated troponin level (OR 2.84; 95% CI 1.62 to 4.98; p<0.001), elevated BNP level (OR 3.21; 95% CI 1.80 to 5.73; p<0.001), systolic blood pressure <100 mm Hg (OR 2.85; 95% CI 1.13 to 3.80; p=0.026) and heart rate ≥110/min (OR 2.20; 95% CI 1.27 to 3.80; p=0.005). RVD on MDCT did not show a significant association (OR 1.29; 95% CI 0.75 to 2.24; p=0.358). Multivariable logistic regression analysis indicated that a positive cTnI (OR 1.98; 95% CI 1.08 to 3.56; p=0.026) and a positive BNP (OR 2.70; 95% CI 1.47 to 4.94; p=0.001) independently predicted a complicated clinical course (table 3). Of note, age, gender and echocardiographic RVD dropped out of the model, and forced entry of these variables did not improve the model characteristics. The combination of a positive BNP and a positive cTnI was associated with a threefold elevated risk of a complicated clinical course (p<0.001). The complication rate of patients with elevated BNP levels or elevated troponin levels was 11.3% and 15.1%, respectively, but the rate increased to 17.6% for those who had the combination of elevated BNP and troponin levels (figure 2).
Cardiac predictors of 30-day complicated course in 848 haemodynamically stable patients with acute symptomatic pulmonary embolism

{kind=link}
{kind=link}
Frequency of 30-day complicated course according to baseline cardiovascular tests. MDCT, multidetector computed tomography; BNP, brain natriuretic peptide; Ctnl, cardiac troponin 1. “Complicated course”, defined as death from any cause, heamodynamic collapse (defined as need for cadiopulmonary resuscitation, systolic blood pressure >90 mm Hg at least for 15 minutes, need for cathecolamine administration, or need for thrombolysis), or adjudicated recurrent PE within the 30-days of follow-up
Discussion
The PROTECT study investigated the prognostic value of RVD on MDCT in haemodynamically stable patients who had acute symptomatic PE. The findings of this study do not support the hypothesis that an enlarged right ventricle on MDCT in this setting leads to a higher 30-day all-cause mortality or higher rate of life-threatening adverse events. The study found an association between RVD on MDCT and PE-related mortality and haemodynamic collapse within 30 days of PE diagnosis, though it did not achieve statistical significance.
Studies have shown that the right to left ventricular dimensional ratio at MDCT has a good accuracy when compared with echocardiography for the assessment of RVD in patients with acute PE.26 ,27 However, the current literature is not clear regarding the association between MDCT-assessed RV enlargement at the time of PE diagnosis and prognosis.14 ,16 ,20 A retrospective study of 82 stable and unstable patients diagnosed with PE found that several CT variables predicted mortality.28 Two retrospective cohort studies14 ,16 suggested that RV dilatation on spiral CT independently predicted mortality in patients with PE. In contrast, a study of 157 haemodynamically stable patients who were enrolled in the Prospective Investigation of Pulmonary Embolism Diagnosis II investigation found that RV enlargement alone in patients with PE did not seem to indicate a poor prognosis or the need for thrombolytic therapy.20 Pooled results from these three studies did not show an association between MDCT-detected RV enlargement and prognosis in patients with acute PE.10 In contrast, a larger prospective multicentre study of 457 stable and unstable patients who had acute PE confirmed by MDCT detected an association between MDCT-detected RVD and the combined outcome of inhospital death and clinical deterioration,26 but did not find an association with inhospital all-cause mortality alone. The study's strikingly high PE-related mortality rate of 68% suggests that it selectively enrolled a cohort of more severely ill patients than those enrolled in the PROTECT study. Of note, the attending physicians who adjudicated the cause of death for the study were not blinded with respect to echocardiography results. The PROTECT study's large sample size, adjustment for potential confounders, central adjudication of adverse events with blinding to baseline MDCT and echocardiogram results add robustness to the findings that MDCT-assessed RVD at the time of acute PE diagnosis does not predict all-cause death or a complicated course in normotensive patients. However, given the relatively low outcome event rates, the study was not powered to detect an association among RVD on MDCT and cause specific, PE-related mortality and haemodynamic collapse within 30 days of PE diagnosis.
The findings of the PROTECT study have important implications. Different studies suggest the need for clinical prognostic models, alone or in combination with cardiac biomarkers, for identification of patients with PE at low-risk of overall death who might benefit from outpatient PE therapy.7 ,29 The findings of PROTECT study do not support the use of MDCT to identify low-risk patients with PE based on a lack of RVD. Alternatively, some authors have proposed that normotensive patients with RVD on MDCT should potentially undergo thrombolytic therapy.30 The findings from this study do not adequately justify use of thrombolytic therapy in this population. The PROTECT study was not powered to detect a significant difference in PE-related adverse outcomes for those normotensive patients with and those without RVD on MDCT. Although a larger sample size might have detected a significant association between MDCT–RVD and PE-related adverse outcomes, the magnitude of such association would not be strong enough to drive decision-making regarding thrombolytic therapy in most patients.
While previous studies measured RVD on MDCT by a complex procedure that required reformatted images,31 the PROTECT study used a simple assessment using only two-dimensional axial transverse images that did not require multiplanar reconstruction. This approach made the assessment of RVD on MDCT easy and rapid. Of note, the study did not use ECG-gated MDCT. Though the gating process allows more accurate evaluation of the heart, the technique requires longer acquisition times and higher radiation doses.32
Limitations of the PROTECT study include measurement of MDCT–RVD by a simple criterion, and its generalisability only to normotensive patients who undergo evaluation in the Emergency Department. Though the study had a relatively large sample size, the limited number of outcome events in the study might have limited the predictive ability of the models.
In conclusion, PROTECT did not confirm that RVD assessed by MDCT adversely affected prognosis in normotensive patients with acute PE. Thus, the study does not support using the presence or absence of RVD on MDCT to drive decision-making regarding outpatient management or thrombolytic therapy for the treatment of acute PE.
References
Footnotes
-
Collaborators The PROTECT investigators.
-
APPENDIX Coordinator of the PROTECT Study: David Jiménez
PROTECT Steering Committee Members: David Jiménez, José Luis Lobo, Manuel Monreal, Remedios Otero, Roger D. Yusen
PROTECT Study Coordinating Center: S & H Medical Science Service
Adjudication Committee: Francisco Conget, Dolores Nauffal, Mikel Oribe, Fernando Uresandi
Radiology Panel: Ignacio Gallego, Luis Gorospe, Agustina Vicente
Blood Sample Processing: José Manuel del Rey
Statisticians: Víctor Abraira, Javier Zamora, Alfonso Muriel
-
INVESTIGATORS OF THE PROTECT STUDY Consolación Rodríguez, Jorge Vivancos, Jesús Marín (Bormujos), Mikel Oribe, Aitor Ballaz, Jose María Abaitúa, Sonia Velasco (Galdakao), Manuel Barrón, María Lladó, Carmen Rodrigo, Luis Javier Alonso (Logroño), Ramón Rabuñal, Olalla Castro, Concepción Iglesias, Ana Testa (Lugo), David Jiménez, Vicente Gómez, Luis Gorospe, Sem Briongos, José Manuel del Rey (Madrid), Celso Álvarez, Nuria Rodríguez, Amador Prieto, María Martín (Oviedo), Carmen Navarro, Mónica López, Eva Castañer, Eva Guillaumet (Sabadell), Remedios Otero, Teresa Elías, Pilar Serrano, Francisco López (Sevilla), Reina Valle, María Victoria Piret, Pilar Lucio, José María Cuesta (Sierrallana), Dolores Nauffal, Marta Ballester, José Pamies, Ana Osa (Valencia), José Luis Lobo, Vanesa Zorrilla, Delfina Pozo, Ángel Alonso (Vitoria), Francisco Conget, Miguel Ángel Santolaria, Mariano González, José Luis de Benito (Zaragoza).
-
Contributors Study concept and design; drafting of the manuscript: DJ, JLL, MM, LM, DA, RDY. Acquisition of data; analysis and interpretation of data; statistical analysis; critical revision of the manuscript for important intellectual content: DJ, JLL, MM, LM, MO, MB, RO, DN, RR, RV, CN, CRM, CA, FC, FU, DA, RDY. Study supervision: DJ, RDY.
-
Funding FIS 2008 (PI 08200), SEPAR 2008, NM 2010.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Ramon y Cajal Hospital Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.