Article Text

Abstract
Background The lung volume reduction (LVR) coil is a minimally invasive bronchoscopic nitinol device designed to reduce hyperinflation and improve elastic recoil in severe emphysema. We investigated the feasibility, safety and efficacy of LVR coil treatment in a prospective multicentre cohort trial in patients with severe emphysema.
Methods Patients were treated in 11 centres. Safety was evaluated by recording all adverse events, efficacy by the St George's Respiratory Questionnaire (SGRQ) as primary endpoint, and pulmonary function testing, modified Medical Research Council dyspnoea score (mMRC) and 6-min walk distance (6MWD) up to 12 months after the final treatment.
Results Sixty patients (60.9 ± 7.5 years, forced expiratory volume in 1 s (FEV1) 30.2 ± 6.3% pred) were bronchoscopically treated with coils (55 bilateral, 5 unilateral), with a median of 10 (range 5–15) coils per lobe. Within 30 days post-treatment, seven chronic obstructive pulmonary disease exacerbations (6.1%), six pneumonias (5.2%), four pneumothoraces (3.5%) and one haemoptysis (0.9%) occurred as serious adverse events. At 6 and 12 months, respectively, ΔSGRQ was −12.1±12.9 and −11.1±13.3 points, Δ6MWD was +29.7±74.1 m and +51.4±76 m, ΔFEV1 was +0.11±0.20 L and +0.11±0.30 L, and ΔRV (residual volume) was −0.65±0.90 L and −0.71±0.81 L (all p<0.01). Post hoc analyses showed significant responses for SGRQ, 6MWD and RV in patients with both heterogeneous and homogeneous emphysema.
Conclusions LVR coil treatment results in significant clinical improvements in patients with severe emphysema, with a good safety profile and sustained results for up to 1 year.
Trial registration number: NCT01328899.
- Emphysema
- Bronchoscopy
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Key messages
-
What is the key question?
-
Is lung volume reduction coil treatment feasible and does it sustainably improve quality of life and clinical outcomes in a broad group of patients with severe emphysema treated in a multicentre setting?
-
What is the bottom line?
-
Bronchoscopic lung volume reduction coil treatment is associated with a good safety profile and significantly improves quality of life, exercise capacity and pulmonary function in a broad group of patients with severe emphysema, with sustained results at 1 year.
-
Why read on?
-
Further post hoc analysis of CT scan heterogeneity showed significant responses in both heterogeneous and homogeneous emphysema, suggesting that lung volume reduction coil treatment may benefit patients with both heterogeneous and homogeneous emphysema disease distribution.
Introduction
For patients with advanced chronic obstructive pulmonary disease (COPD) who, despite optimal medical management still have severe dyspnoea, bronchoscopic lung volume reduction could be a beneficial treatment option.1 ,2 Although lung volume reduction surgery and lung transplantation are still valid treatment modalities for patients with COPD, the use of these interventions is very limited because of strict patient selection criteria, significant morbidity and donor shortage.3–5
To date, bronchoscopic lung volume reduction using one-way endobronchial valves (EBV) has been the most extensively investigated technique in this field.6–8 However, successful clinical outcomes from EBV therapy can only be achieved in patients with no interlobar collateral ventilation and when the one-way valves are placed to entirely block all the airways into the target lobe, which can be technically difficult due to local anatomy and in the absence of significant experience with these devices.6–8 It is estimated that only about 33% of patients with severe emphysema have no collateral ventilation between the target and adjacent lobe and can thus potentially be treated using one-way valves.1 This clearly shows the need for alternative bronchoscopic treatments that work independently of the presence of collateral ventilation.
In 2010 we reported the first human trial using bronchoscopically delivered nitinol lung volume reduction (LVR) coils.9 Up to six shape-memory coils per lung were placed in patients with severe emphysema, resulting in moderate effects only in the patients with heterogeneous emphysema but without any serious adverse events. After that first trial we improved the LVR coil treatment to target the most diseased areas of the lung with approximately 10 coils placed per lobe, in order to maximise re-tensioning of the airway network. The results using this approach in 16 patients with upper lobe predominant heterogeneous emphysema have previously been published, showing feasibility and safety and also demonstrating statistically and clinically significant improvements in pulmonary function, exercise capacity and quality of life.10 Surprisingly, even in this early pilot phase, two-thirds of the patients treated responded beyond the minimal clinically important differences (MCID) for forced expiratory volume in 1 s (FEV1),11 residual volume (RV),12 6-min walk distance (6MWD)13 and St George's Respiratory Questionnaire (SGRQ).14
Following the successful early experiences in these two pilot trials, the current study allowed further investigation into the feasibility, safety and efficacy of LVR coil treatment in a multicentre setting in a larger group of patients.
Methods
This prospective open-label multicentre feasibility study was conducted in 11 hospitals in France, Germany and the Netherlands and was approved by the ethics committee at each site. The first patient was enrolled in December 2009 and the final patient in October 2011. The initial protocol proposed a follow-up period of 6 months following initial treatment. However, because the Dutch and French ethics committees required a 12-month follow-up period, the protocol was modified to require a 12-month follow-up for patients in the Netherlands and France, while maintaining the original 6-month follow-up period for patients in Germany. This paper reports on all patients in the study at both exit points.
Patients
Patients with COPD with upper or lower lobe predominant bilateral heterogeneous emphysema on chest CT scan as judged by the treating physician were considered for inclusion. All patients were intended to be treated bilaterally, in accordance with the protocol assessment schedule. The inclusion and exclusion criteria are presented in box 1.
Box 1 Main study inclusion and exclusion criteria
Main inclusion criteria
-
>35 years of age
-
CT scan indicates bilateral heterogeneous emphysema
-
Post-bronchodilator FEV1 <45% of predicted
-
Total lung capacity >100% of predicted
-
RV >175% of predicted
-
mMRC >2 (0–4)
-
Stopped smoking for >8 weeks prior to entering the study
Main exclusion criteria
-
Change in FEV1 >20% post-bronchodilator
-
Tlco <20% of predicted
-
History of recurrent clinically significant respiratory infection
-
Pulmonary hypertension: right ventricular pressure >50 mm Hg
-
Inability to walk >140 m in 6 min
-
Previous LVR surgery, lung transplant or lobectomy
-
Clinically significant bronchiectasis
-
Giant bullae more than one-third lung volume
-
Severe destructed homogeneous emphysema by CT scan
-
Patient on antiplatelet agent (eg, clopidogrel) or anticoagulant therapy (eg, heparin or coumadin) or has not been weaned off prior to procedure
FEV1, forced expiratory volume in 1 s; LVR, lung volume reduction; mMRC, modified Medical Research Council dyspnoea score; RV, residual volume; Tlco, carbon monoxide lung transfer factor.
Lung volume reduction (LVR) coil treatment
LVR coil treatment was performed as previously described.10 Briefly, the RePneu LVR coil (PneumRx, USA) (figure 1) is an implantable device composed of preformed nitinol wire which is straightened for delivery via a therapeutic flexible bronchoscope into subsegmental airways using a special delivery catheter, cartridge and loading forceps. Once in place, it is released and recovers to a non-straight predetermined shape upon deployment. Seven sizes of coil were available (70, 85, 100, 125, 150, 175 and 200 mm). All procedures were performed under general anaesthesia and the deployment of the coil was visualised under fluoroscopy. The coils were deployed with the objective of achieving equal subsegmental distribution throughout one target lobe. The contralateral procedure was performed at least 1 month after the first procedure.

Fully deployed nitinol RePneu lung volume reduction coil.
Assessments and follow-up
Screening assessments included medical history, physical examination, dyspnoea assessment by the modified Medical Research Council dyspnoea scale (mMRC), quality of life assessment by the SGRQ,15 echocardiogram, pre- and post-bronchodilator spirometry, lung volume measurements by body plethysmography,16 6MWT,17 chest X-ray and a thoracic CT scan.
The patient was kept at least overnight after the procedure. A 1-month follow-up evaluation was performed, after which the second procedure was scheduled. Patients were then followed at 1, 3, 6 and 12 months (the latter only in France and The Netherlands).
Primary/secondary endpoints and safety objectives
The primary efficacy endpoint was the improvement in SGRQ total score from baseline compared with the score at 6 months. The secondary efficacy endpoints were the comparison between baseline and 6 months for forced vital capacity (FVC), FEV1, RV, residual volume to total lung capacity (RV/TLC) ratio, improvement in 6MWD and mMRC score. The responder rate at 6 months was calculated using the MCID defined for FEV1,11 RV,12 6MWD13 and SGRQ.14
The safety objectives were to identify the number and type of device-related and procedure-related adverse events related to the use of the LVR coil.
Post hoc CT scan analyses
Since inclusion in this trial was based on the treating physicians’ visual chest CT judgement, a post hoc analysis was performed on these CT scans to analyse the relationships between the response to LVR coil treatment at 12 months follow-up and the level of heterogeneity assessed by a blinded qualitative visual 4-point tissue destruction score scale (0–25%, 26–50%, 51–75%, >75% visible tissue destruction), as well as by calculating the percentage area of destruction below −950 Hounsfield Units (HU) between the upper and lower lobes of both lungs. Quantitative CT analyses were blinded and performed with CIRRUS Lung 13.10 (Diagnostic Image Analysis Group Nijmegen, The Netherlands; Fraunhofer MEVIS, Bremen, Germany). The lungs and lobes were automatically segmented and visually inspected. Emphysema was quantified per lobe as an emphysema score: the percentage of voxels below −950 HU.18
For the visual assessment, a patient was classified as heterogeneous if there was a difference of >1 point between ipsilateral lobes on both sides. For the computerised assessment, a patient was classified as heterogeneous when the difference for both lungs in the lung tissue destruction score was >25% at −950 HU between ipsilateral upper and lower lobes.
Statistics
This trial was powered on the statistical significant difference in expected SGRQ total score between baseline and the 6-month follow-up time point using an α<0.05 with a power of 0.90, taking a patient loss to follow-up of 10% into account.10
Data are presented as mean±SD, except for the presentation of the five unilateral cases and descriptive statistics on the detailed procedural results (table 2) where data are expressed as median (minimum−maximum) or median when appropriate. The statistical significance of changes from baseline was assessed by the paired Student t test. A linear regression analysis was performed to associate outcome at 6 months for changes in SGRQ and 6MWD, using as baseline regressors RV% pred, RV/TLC, FEV1% pred, FVC, age, carbon monoxide lung transfer factor (Tlco) and emphysema type (homogeneous or heterogeneous disease). The models were simple linear with no interactions or terms higher than first order included; p<0.05 was considered statistically significant. SAS V.9.3 was used for all analyses. All data in this trial were independently monitored by a contract research organisation.
Results
Patients and procedures
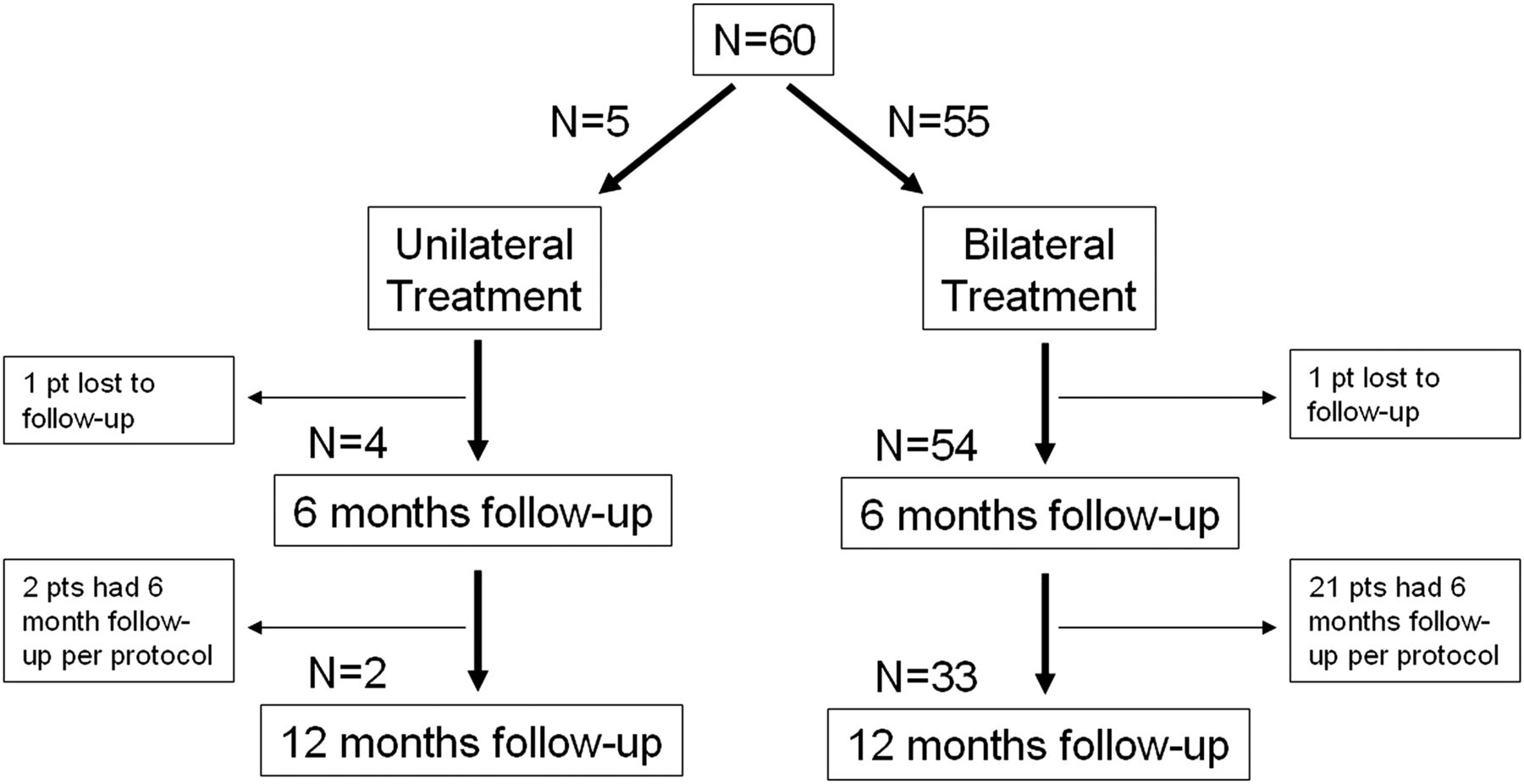
Sixty patients were enrolled between December 2009 and October 2011 and their baseline demographics are shown in table 1). A total of 115 procedures were performed (5 patients had unilateral treatment, figure 2) in which a total of 1125 LVR coils were placed. A median of 10 coils (range 5–15) was placed per lobe (table 2).
Patient demographics and baseline characteristics (n=60)
Lung volume reduction coil procedural results

{kind=link}
{kind=link}
Study flow chart.
Safety
No periprocedural serious adverse events occurred in the 115 bronchoscopies performed under general anaesthesia. No death or respiratory failure was reported. A summary of all serious and non-serious respiratory adverse events is listed in table 3. All events were treated and resolved with routine medical care and without sequelae.
Adverse events
Efficacy
All patients
Of the 60 patients who were bilaterally treated, 58 were evaluable at 6 months and 34 at 12 months (24 patients from Germany exited the study at 6 months). Because the German cohort exited the study at 6 months, we segregated the data to compare patients with 1-year follow-up data against their own 6-month results to analyse the sustainability of the clinical improvements within the same population (table 4). Across key clinical parameters, FEV1% pred, RV% pred and SGRQ results were sustained while mean 6MWD actually improved between 6 and 12 months. The MCID responder percentages for FEV1, RV, 6MWD and SGRQ are shown in table 5.
Efficacy results at 6 and 12 months
Responder rates at 6 and 12 months
Unilateral patients
Five patients were treated unilaterally. The reasons for treating only one lung were: lost to follow-up in two patients; second lung on second look not suitable for treatment (bullae) in one patient; and second lung declined by two patients (one improved satisfactory and one did not want to proceed with the trial). At 6-month follow-up in four evaluable patients, the median change in FEV1 was +4.7% (range −17.8% to +17.0%), median change in 6MWD was +29 m (range −46 m to +92 m) and RV and RV/TLC remained stable.
Heterogeneous versus homogeneous disease
In the 33 bilaterally treated patients with 12 months follow-up, the post hoc visual qualitative CT score of the degree of tissue destruction classified 20 patients as heterogeneous and 13 as homogeneous. When using the CT software analysis, 16 patients were classified as heterogeneous and 17 as homogeneous. Regardless of the classification method, both heterogeneous and homogeneous patients showed significant improvement at 1 year (table 6).
Results at 12 months after bilateral LVR coil treatment for patients classified as heterogeneous and homogeneous emphysema
Upper versus lower lobe disease
In this trial lower lobe treatment was performed in 10 patients, of whom nine could be evaluated at the 6-month endpoint. Except for FEV1 (+0.04±0.08 L for lower lobe vs +0.15±0.23 L for upper lobe; p=0.026), there were no statistically significant differences in the clinical responses between patients with upper versus lower lobe disease for RV, 6MWD and SGRQ.
Responder analysis
To identify LVR coil treatment responders we performed a multivariable analysis for the primary endpoint SGRQ and for the 6MWD. None of the input regressors (RV% pred, RV/TLC, FEV1% pred, FVC, age, Tlco and emphysema type) were useful in associating patient outcomes at 6 months.
Discussion
This prospective multicentre study assessed the long-term safety and improvements in patient-related outcome measures of LVR coil treatment in 60 patients with severe emphysema. The results show an acceptable safety profile associated with a significant and sustained improvement over 12 months in relevant clinical and functional parameters including FEV1, RV, 6MWD and SGRQ.
This is the largest LVR coil study to date, and also evaluated longer-term results of LVR coil treatment. In our first pilot study (n=16) using the current treatment approach (median 10 coils per lung) and coil design, significant clinical and functional improvements were seen at 6 months including SGRQ (−14.9 points), FEV1 (+14.9%), RV (−11.4%) and 6MWD (+84 m) with an acceptable safety profile.10 Recently, Shah et al19 reported the results at 90 days after bilateral LVR coil treatment for 46 patients included in a randomised controlled study and demonstrated a significant improvement in SGRQ (−8.1 points), FEV1 (+14%), RV (−0.51 L) and 6MWD (+51 m), with no difference in serious adverse events between treatment and control groups.
In the present multicentre study involving 11 centres, no serious adverse events were reported during the LVR coil treatment procedures, demonstrating procedural safety. Serious adverse events (table 3) mainly occurred in the 30 days after the procedure, with all events resolving with regular medical care and without sequelae. Our results confirm the acceptable safety profile for LVR coil treatment with a rate of adverse events similar to previous reports on LVR coil treatment.10 ,19 The rate of post-procedure exacerbations and pneumonia is comparable to reported events with endobronchial one-way valves.6 ,8 Importantly, the total rate of these COPD-related events following endoscopic implants did not exceed the number of exacerbations and pneumonia that were reported in the EASE trial sham bronchoscopy control group.20 LVR coil specific procedure-induced events that occur are typically very mild haemoptysis or coloured sputum requiring no intervention in about 50% of subjects and temporary chest discomfort for a few days requiring either a standard painkiller regimen for a few days or no intervention at all in about one-third of subjects treated.
Regarding efficacy, our results show significant improvements in clinical and functional parameters at 6 months with a magnitude of response in line with the two recent reports on LVR coil treatment,10 ,19 reporting on 6- and 3-month follow-up, respectively. Our study provides the first longer-term analysis of data over 12 months after bilateral LVR coil treatment and demonstrates a sustained response at 12 months. To better analyse the relevance of the efficacy results, we analysed the MCID in FEV1,11 RV,12 6MWD13 and SGRQ14 and found a significant responder rate at 6 and 12 months for these clinical endpoints (table 5).
The cohort trial design can, of course, induce bias. However, the results reported are higher than reported MCID for our endpoints and show similar efficacy across multiple centres. Furthermore, we have previously shown that, even in a sham-controlled bronchoscopic interventional trial design, no real placebo effect could be observed in patients with severe COPD.20
To better understand the predictors of response to LVR coil treatment, we conducted a multivariate analysis to assess the relationship between the response to treatment and baseline variables typically identified as predictors of outcome, such as hyperinflation and emphysema heterogeneity. Using the 6-month endpoints, none of the evaluated baseline variables provided a meaningful predictor of response to LVR coil treatment. Other potential variables could include nuanced emphysema phenotypes beyond heterogeneous or homogeneous classification, such as more or less small airways disease, centrilobular versus panlobular emphysema and variability in placement strategies including proximal versus distal placement within the subsegmental airways and/or the number and size of coils deployed. The current active clinical trials (NCT0182279521 and NCT01608490) and future meta-analysis data of patients treated in the four European clinical studies thus far may increase the statistical power sufficiently to perform this analysis better. In our study, where broad selection criteria were purposely used in order to evaluate the effectiveness in a population of patients representative of the patients we see in daily practice, we found a large variability of response between patients. However, responder rates overall for several endpoints were already high (table 5).
The difficulty of identifying strong predictors of success has been previously demonstrated by a predictive multivariate effort completed in a much larger patient cohort (n=608) for outcome after lung volume reduction surgery. In this large group, only a very weak signal for RV/TLC and emphysema distribution could be demonstrated.22
Lung hyperinflation is a major feature of emphysema and is associated with dyspnoea, exercise intolerance and compromised daily physical activity.23 ,24 In this study, neither baseline RV nor RV/TLC predicted the response to LVR coil treatment. This is possibly due to the fact that RV >175% pred was an inclusion criterion, resulting in treatment of severe static hyperinflated patients (mean baseline RV 249.2±53.2% pred). On the other hand, the magnitude of change in RV after LVR coil treatment was associated with more favourable mean clinical and functional outcomes in this study, suggesting that RV changes may be viewed as a marker of response to treatment and that, by selecting patients with more potential for significant RV decrease, the likelihood of significant clinical benefit may be increased. The finding that RV is reduced by LVR coil treatment might be related to mechanical volume compression of lung tissue exerted by the coils, as well as improvement in elastic recoil achieved by decreasing airway resistance.25
When comparing the results for patients with upper lobe versus lower lobe treatment, no outcome differences were observed for RV, 6MWD and SGRQ. The lower FEV1 results seen with lower lobe coil treatments is comparable to the experience with lung volume reduction surgery in the lower lobes where the effect on improving FEV1 is also limited compared with other outcome variables.26 However, because FEV1 in general shows poor correlation with performance in patients with severe emphysema,27 and that patient-relevant outcomes such as 6MWD and SGRQ show strong improvement even in lower lobe subjects, lower lobe treatment with coils appears to be a clinically valid treatment option with clear patient benefit. Future work will evaluate whether, as currently hypothesised, the much bigger lower lobes require a greater number of coils to optimise results.
Our post hoc CT analysis showed that a large number of patients were classified as homogeneous when using both a visual and a digital assessment, even though the inclusion criteria called for heterogeneous patients per clinicians’ visual assessment. This finding should be cautiously considered, since this trial was not designed to prospectively identify homogeneous emphysema patients and the two methods of creating a heterogeneous versus a homogeneous group are arbitrary. Our results show that LVR coil treatment also benefits patients with less pronounced heterogeneous to homogeneous disease. Our data showed a statistically and clinically significant benefit for both groups compared with baseline, with overall a potentially increased mean efficacy for the heterogeneous patient group. The fact that LVR coil treatment also shows efficacy in patients with homogeneous emphysema is a very important finding, challenging the assumption that only patients with heterogeneous emphysema will respond to LVR coil treatment, as has been shown for surgical lung volume reduction28 and EBV.6 ,7 Of note, other bronchoscopic techniques such as thermal vapour ablation29 and sealant therapy30 are also restricted to upper lobe predominant heterogeneous emphysema, leaving a broad group of patients with non-upper lobe predominant and homogeneous disease without a treatment option. It can be hypothesised that LVR coil treatment is similarly efficient in both heterogeneous and homogeneous emphysema because of a different mechanism of action from true ‘lung volume reducing’ therapies, as the primary mechanism of action of coils appears to be mechanical re-tensioning of the airway network rather than just reducing absolute lung volume alone. However, additional studies are necessary to better characterise the mechanisms of action of coils and also to confirm the efficacy of LVR coil treatment in homogeneous emphysema, which represents a large number of patients usually excluded from other surgical and bronchoscopic lung volume reduction treatment options.
In conclusion, this study provides multicentre evidence for the feasibility, procedural safety and efficacy of LVR coil treatment in patients with both heterogeneous and homogeneous emphysema. Further studies are underway to confirm efficacy in long-term randomised trials. Additional studies are needed to improve the understanding of the predictive factors of response in order to better select the responders to LVR coil treatment.
References
Footnotes
-
Contributors GD, KK and DS operated as a writing committee and drafted the manuscript until it reached its final form. GD, KK, MH, FS, RK, C-HM, CW, SB, WG, FJFH, JH and D-JS all participated as investigators in this trial, recruited patients, performed the treatments and commented on the manuscript and its revisions. EMvR wrote the sections on CT and performed all the imaging analysis.
-
Competing interests The sponsor designed the trial together with GD and D-JS, and facilitated monitoring of safety and independent audit, collection and storage of data. The authors had full access to all the data in the study and had final responsibility to submit for publication. The hospitals of the local PIs (GD, MH, FS, RK, C-HM, CW, SB, WG, FJFH, JH and D-JS) were reimbursed for study-related costs. KK received and MH receives consultancy fees from PneumRx. D-JS and GD are physician advisors to PneumRx and received travel reimbursements and speaker fees for educational sessions. EMvR has no competing interest.
-
Ethics approval Ethics approval was obtained from the ethics committee at each site.
-
Patient consent All subjects gave written informed consent.